Development and validation of prognostic nomogram based on log odds of positive lymph nodes for patients with gastric signet ring cell carcinoma
2021-01-18ZijieXuJingJingGuiliangMa
Zijie Xu ,Jing Jing ,Guiliang Ma
1Department of General Surgery,Qingdao Municipal Hospital,Qingdao University,Qingdao 266071,China;2 Department of Endocrinology,Qingdao Municipal Hospital,Qingdao University,Qingdao 266071,China
Abstract Objective:Our aims were to establish novel nomogram models,which directly targeted patients with signet ring cell carcinoma (SRC),for individualized prediction of overall survival (OS) rate and cancer-specific survival (CSS).Methods:We selected 1,365 SRC patients diagnosed from 2010 to 2015 from Surveillance,Epidemiology and End Results (SEER) database,and then randomly partitioned them into a training cohort and a validation cohort.Independent predicted indicators,which were identified by using univariate testing and multivariate analyses,were used to construct our prognostic nomogram models.Three methods,Harrell concordance index (C-index),receiver operating characteristics (ROC) curve and calibration curve,were used to assess the ability of discrimination and predictive accuracy.Integrated discrimination improvement (IDI),net reclassification improvement (NRI) and decision curve analysis (DCA) were used to assess clinical utility of our nomogram models.Results:Six independent predicted indicators,age,race,log odds of positive lymph nodes (LODDS),T stage,M stage and tumor size,were associated with OS rate.Nevertheless,only five independent predicted indicators were associated with CSS except race.The developed nomograms based on those independent predicted factors showed reliable discrimination.C-index of our nomogram for OS and CSS was 0.760 and 0.763,which were higher than American Joint Committee on Cancer (AJCC) 8th edition tumor-node-metastasis (TNM) staging system (0.734 and 0.741,respectively).C-index of validation cohort for OS was 0.757 and for CSS was 0.773.The calibration curves also performed good consistency.IDI,NRI and DCA showed the nomograms for both OS and CSS had a comparable clinical utility than the TNM staging system.Conclusions:The novel nomogram models based on LODDS provided satisfying predictive ability of SRC both in OS and CSS than AJCC 8th edition TNM staging system alone.
Keywords:Log odds of positive lymph nodes;nomograms;prognosis;signet ring cell
Introduction
Gastric cancer (GC) is a severe threat to human health,ranking fifth for most commonly diagnosed cancers and third for cancer mortality worldwide.There were over one million newly-diagnosed cases and an estimated 783,000 deaths in 2018 (1).Incidence rates are significantly rising in East Asia,whereas a generally low incidence was observed in Northern America and North Europe (1).Although the morbidity of GC has declined in recent years,some western studies demonstrated the morbidity of signet ring cell (SRC) carcinoma was still high (2).According to the definition of World Health Organization (WHO),SRC was characterized as isolated or small groups of malignant non-cohesive cells (3).In other classifications,SRC was defined as an undifferentiated carcinoma by the Japanese Gastric Cancer Association and as a diffuse type by Lauren (4).
The prognosis of SRC is still controversial in the literature.Many studies indicated that SRC patients had a relatively better prognosis for early stage as compared to other histological types,but a worse prognosis in advanced stage (5-9).However,Kimet al.reported that SRC had no significant effect on prognosis (10).Given the conflicting conclusion of SRC,we considered that it is necessary for SRC patients to establish a more reliable,specific and precise clinical model predicting their actual clinical outcome rather than a common one for all GC patients.
The metastasis of regional lymph nodes is an essential indicator in predicting gastric cancer prognosis (11).Based on the absolute amount of lymph node metastasis,the American Joint Committee on Cancer (AJCC) tumornode-metastasis (TNM) staging system is widely used in guiding clinical management and predicting patient survival.Nevertheless,this system is susceptible to stage migration,particularly when a small quantity of lymph nodes are dissected,which may lead clinical physicians to underestimate severity of the disease (12).Recent evidence indicates that positive lymph node ratio (LNR) and the log odds of positive lymph nodes (LODDS) could provide a more satisfactory predictive ability compared with AJCC N stage in assessing postoperative survival rate of gastric cancer patients (13-16).
Therefore,our study sought to build a SRC-specific nomogram model based on LODDS predicting overall survival (OS) rate and cancer-specific survival (CSS) by using the Surveillance,Epidemiology,and End Results(SEER) database.
Materials and methods
Ethics statements
All patient data extracted from the SEER database(http://www.seer.cancer.gov), anonymized and publicly available,didn`t contain any identifier.For this reason,our study was approved by the Ethics Committee of Qingdao Municipal Hospital of Qingdao University (Shandong,China).
Patient selection
In this research,clinical data were obtained from SEER database by SEER*Stat software (Version 8.3.8;www.seer.cancer.gov/seerstat;Surveillance Research Program,National Cancer Institute,USA).The current SEER database was consisted of 18 population-based cancer registries,covering up to 28% of the total American population.Patients with SRC gastric carcinoma (third edition of the International Classification Disease for Oncology,histology code:8490/3) were included.Other inclusion criteria were shown as described below.Patients diagnosed in 2010-2015,with only one primary tumor lesion,complete TNM stage information,operation and complete survival data were enrolled into the study.Patients with missing information in grade,race,tumor size or SEER cause-specific death classification were excluded.To minimize confounding factors,those patients with less than 1 month survival period were excluded,which might die from perioperative complications rather than tumor progression (17,18).Finally,1,365 patients were included and then assigned to the training cohort and the validation cohort,by using a random sampling method.The detailed screening process for SRC patients is shown inFigure 1.We obtained approval to access the SEER of the National Cancer Institute in the United States using the reference number 12092-Nov2019.
Prognostic variables
We collected variables of patients including age,grade,race,sex,tumor site,tumor size,AJCC TNM stage,the total amount of lymph nodes retrieved,the amount of metastatic lymph nodes,cause-specific death classification,survival time and survival status.All patients were restaged according to the AJCC criteria as described in AJCC 8th edition staging manual.LNR was defined as a ratio of the amount of metastatic lymph nodes to total amount of lymph nodes retrieved.The LODDS was formulated by loge([0.5+the amount of metastatic lymph nodes]/[0.5 +the amount of negative lymph nodes]) (13).
The first endpoint was OS which was calculated from the date of diagnosis to the date of death from any cause,the second endpoint was CSS which was calculated from the date of diagnosis to the date of death of cancer.The patients were divided into three groups according to their age,the young age group (<45 years),the middle age group(45-59 years),the old age group (≥60 years).The optimal cut-off value of LNR and tumor size was calculated by using X-tile software (Version 3.6.1,Yale University School of Medicine,USA) (19) (Figure 2).Based on the optimal cut-off value,tumor size was divided into <3.5 cm,3.5-6.8 cm and >6.8 cm groups.And LNR was divided into three subgroups,namely LNR1 (0-0.11),LNR2(0.11-0.57) and LNR3 (0.57-1).The LODDS was divided into four categories:LODDS1 (LODDS≤-2.5),LODDS2(-2.5<LODDS≤-1),LODDS3 (-1<LODDS≤0.9) and LODDS4 (LODDS>0.9) (13).
Statistical analysis
Survival analysis was performed using Kaplan-Meier method and log-rank test while comparison of categorical variables was performed by using Chi-square test.Univariate and multivariate statistical tests were used to assess the prognostic value of variables and filter out some potential risk indicators of SRC patients.The comparison of discrimination and predictive performance among three lymph node systems,LODDS,LNR and N stage,was evaluated by the Harrell concordance index (C-Index) and Akaike information criterion (AIC).Lymph node staging system with minimization of AIC was the best-fit model.The area under the curve (AUC) of the receiver operating characteristic (ROC) curve was also used to evaluate the prognostic accuracy of three lymph node staging systems.The better lymph node staging scheme was used to construct nomogram. The discrimination of our nomogram model was quantified by C-index and AUC of ROC curve.Then the calibration was evaluated graphically by plotting the relationship between the predicted probabilities and actual probabilities for each outcome.Additionally,using integrated discrimination improvement(IDI) and net reclassification improvement (NRI),we assessed net benefit of our nomogram.And the clinical utility was evaluated by using decision curve analysis(DCA).All statistical analyses were conducted using R statistical software (Version 4.0.0;R Foundation for Statistical Computing,Vienna,Austria).Variables with P<0.05 were taken into consideration as significant.While,variables with P<0.2 in univariate testing were selected as candidate variables and were included in multivariate analysis.
Results
Clinicopathological characteristics of patients
For this research,1,365 patients diagnosed with SRC between 2010 and 2015 were included and randomly partitioned into the training cohort (n=687;50.3%) and the validation cohort (n=678;49.7%).Detailed descriptive statistics are shown inTable 1.No statistical difference was found between the two groups.Most patients were white(n=886;64.9%) and male (n=697;51.1%).Over half of patients (52.4%) were at the old age group.Meanwhile,522 patients (38.2%) were with a tumor size <3.5 cm.The main grade was III (94.3%) and 1,225 patients (89.7%)were in M0 stage.Moreover,610 patients (44.7%) were in the LNR1 group and 471 patients (34.5%) were in the LODDS1 group.The gastric antrum (including pylorus)was the most common site for SRC (33.4%).The median follow-up time for all patients was 28 [interquartile range(IQR),13-53] months.And in training cohort,the median follow-up time was 27 (IQR,13-54) months and in validation cohort it was 29 (IQR,13-53) months.
Prognostic factors of OS and CSS
By using univariate testing,nine parameters,age,race,T stage,M stage,N stage,LODDS,LNR,tumor size and tumor site were associated with OS and CSS (P<0.2,Table 2,3).In comparison with three lymph node systems,AIC of predicted OS rate for N stage,LNR and LODDS were 4,524.74,4,512.35 and 4,498.97.And AIC of predicted CSS for N stage,LNR and LODDS were 4,155.07,4,144.60 and 4,135.16.
For predicting OS rate,C-index of LODDS was 0.745,which was enhanced than LNR and N stage (0.737;0.734,respectively).The AUCs of LODDS was much better than N stage in predicting 3-year OS rate (0.827vs.0.815,P=0.022),but found no marked difference in 1-and 5-year OS rate (0.744vs.0.729,P=0.063;0.844vs.0.839,P=0.445,respectively).Compared LODDS with LNR,AUCs for 1-year OS rate had significant difference (0.744vs.0.728,P=0.007),but no significant difference was found in 3-and 5-year OS rate (0.827vs.0.820,P=0.088;0.844vs.0.835,P=0.100,respectively).The AUCs of LNR and N stage for 1-,3-and 5-year OS rate showed no statistical difference(P=0.891;P=0.378;P=0.479,respectively) (Table 4).
And for predicting CSS,the C-index of LODDS was 0.751,which was also enhanced compared with LNR and N stage (0.745;0.741,respectively).The AUC for 3-year of LODDS was significantly better than N stage (0.832vs.0.820,P=0.035),but no marked difference was found in 1-and 5-year (0.749vs.0.738,P=0.180;0.849vs.0.845,P=0.534).In addition,the AUCs for 1-,3-and 5-year CSS between LODDS and LNR found no statistical difference(P=0.071;P=0.220;P=0.245,respectively).Meanwhile,the AUCs of LNR and N stage for 1-,3-and 5-year had no statistical difference (0.738vs.0.738,P=0.927;0.826vs.0.820,P=0.304;0.842vs.0.845,P=0.694,respectively)(Table 5).To compare the C-index,AIC,and AUC of three methods (Table 4,5),we eventually incorporated LODDS into the next multivariate analysis.
Age is a vital prognostic variable in clinical practice.Although age failed to reach statistical significance (P>0.2)in univariate testing,we decided to incorporate age into the multivariate analysis of CSS.Six parameters,age,race,LODDS,T stage,M stage and tumor size,were defined as independent prognostic factors of OS by multivariate Cox regression analysis (P<0.05,Table 2).While,only five parameters,age,LODDS,T stage,M stage and tumor size,were significantly correlated with CSS in multivariate analysis (P<0.05,Table 3).
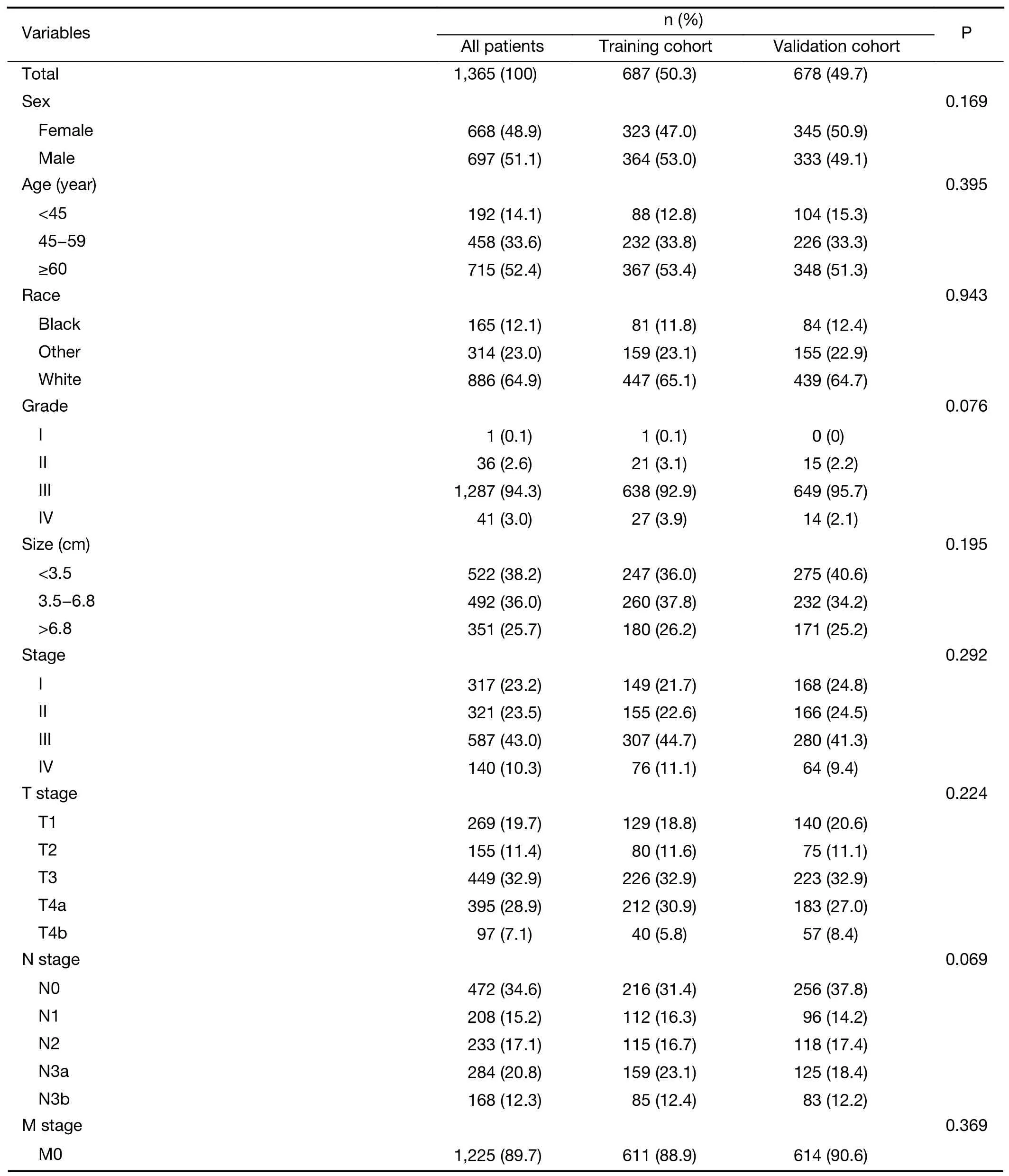
Table 1 Demographic and clinicopathological characteristics of patients
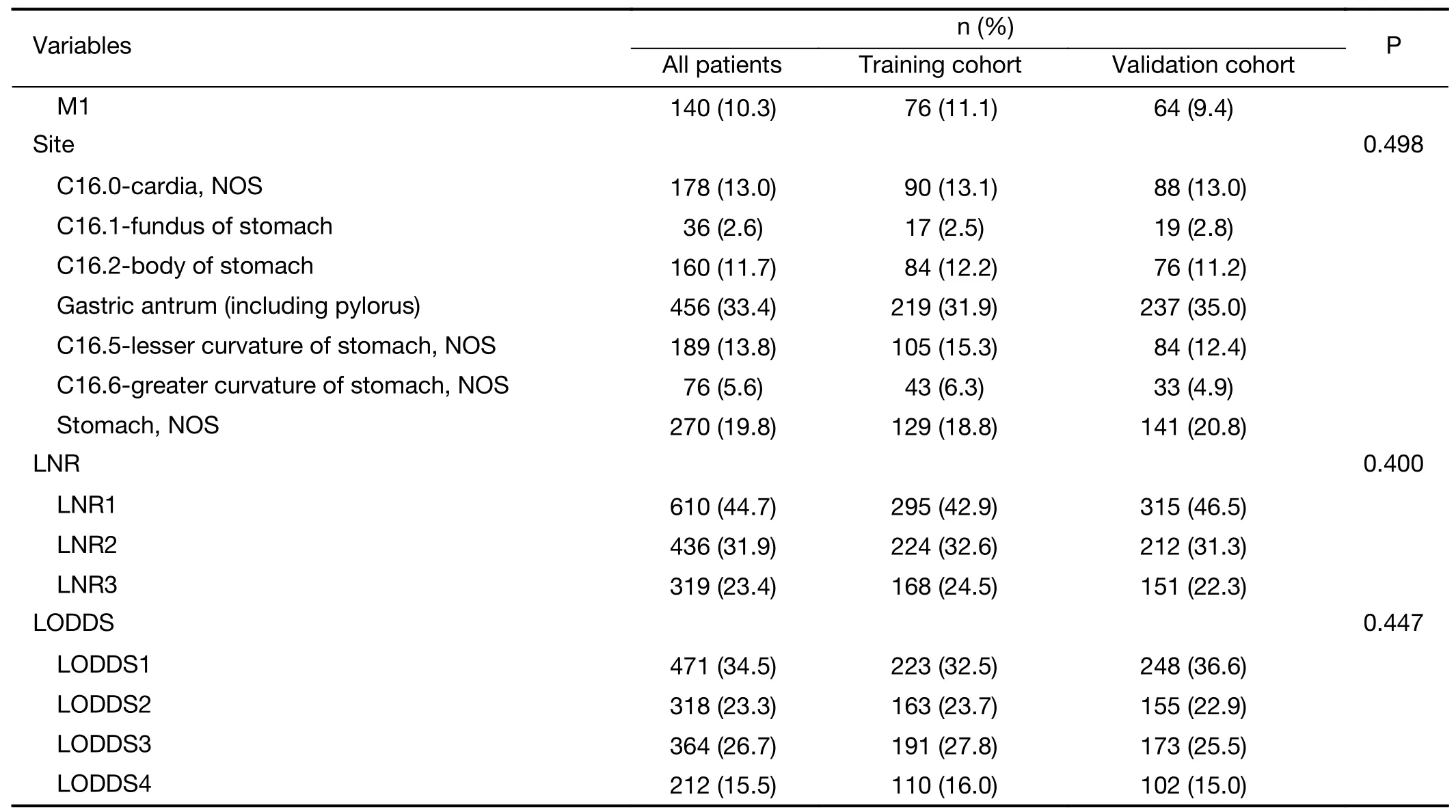
Table 1 (continued)
Construction and validation of prognostic prediction nomogram
Those prognostic variables, which were identified independent with each other in multivariate analysis,were used to construct the prognostic prediction nomogram models.Our OS and CSS nomograms are shown inFigure 3.For predicting OS rate,the C-index of nomogram in the training cohort was 0.760 [95% confidence interval (95%CI),0.735-0.785] and in the validation cohort it was 0.757(95% CI,0.732-0.782),which showed higher statistic power than AJCC TNM staging [0.734 (95% CI,0.709-0.760),P<0.001;0.741 (95% CI,0.716-0.766),P=0.004]. And for CSS prediction, the C-index of nomogram in the training cohort and the validation cohort was 0.763 (95% CI,0.738-0.789) and 0.773 (95% CI,0.748-0.798),which was higher than that of AJCC TNM staging [0.741 (95% CI,0.716-0.767),P<0.001;0.757(95% CI,0.732-0.782),P=0.006,respectively].These results revealed that our nomogram demonstrated a better discrimination and ability of prognostic predictive over the 8th edition AJCC TNM staging.The similarities between the actual observation and predicted survival rates of nomogram were validated by plotting a calibration curve of training cohort and validation cohort of OS and CSS(Figure 4).Furthermore,the predictive performance of novel nomogram models was calculated by AUC of ROC curve (Figure 5).In the training cohort,the AUC values were 0.768,0.841 and 0.861 for 1-,3-and 5-year OS rates,which revealed higher statistic power than AJCC TNM staging (0.729,P<0.001;0.815,P=0.002;0.839,P=0.024,respectively).And AUC values for 1-,3-and 5-year CSS rates were 0.771,0.845 and 0.863 (Figure 5A,B),which were higher than AJCC TNM staging (0.738,P=0.003;0.820,P=0.001;0.845,P=0.056,respectively).In the validation cohort,the AUC values were 0.780,0.844 and 0.870 for 1-,3-and 5-year OS rates,which observed no significant difference with AJCC TNM staging (0.762,P=0.058;0.831,P=0.078;0.856,P=0.111,respectively).For the CSS prediction,the AUC values were 0.788,0.860 and0.890,which showed a slight preponderance over AJCC TNM staging (0.776,P=0.193;0.846,P=0.039;0.877,P=0.095,respectively) (Figure 5C,D).
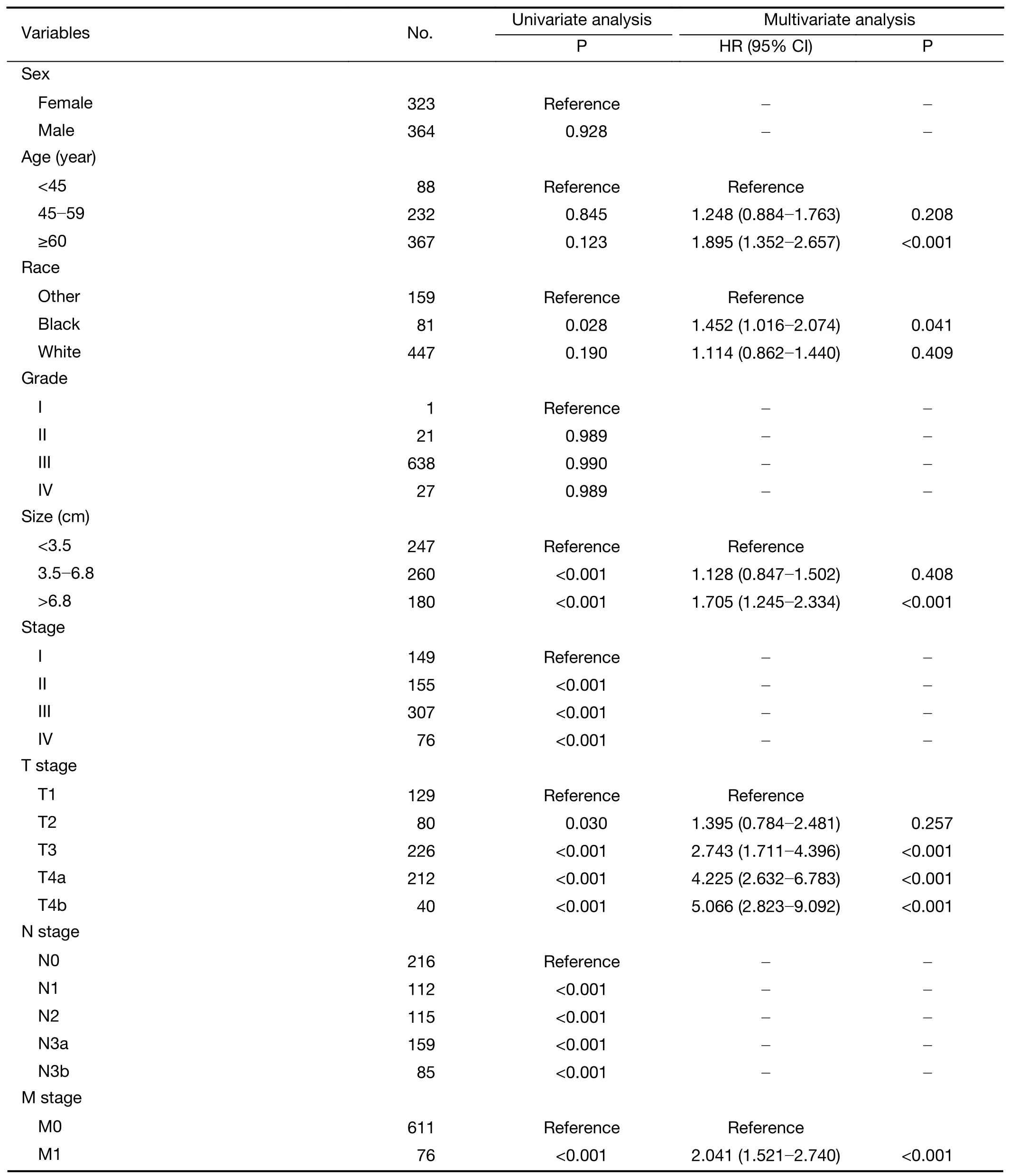
Table 2 Univariate and multivariate analysis of OS in training cohort (N=687)
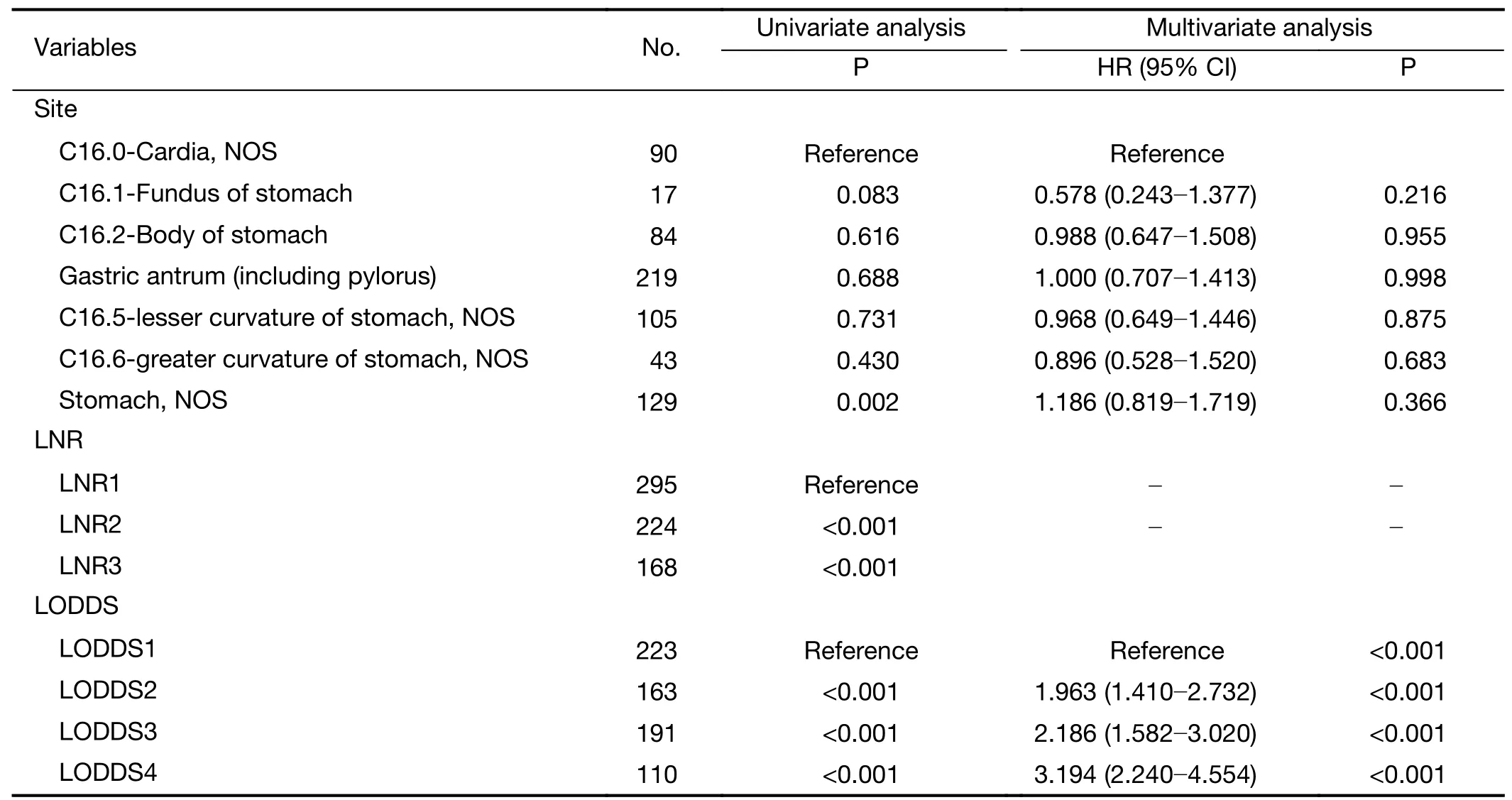
Table 2 (continued)
Clinical value of nomogram
In the decision curve analysis,the novel nomograms showed more net benefit across the range of decision threshold probabilities than the AJCC 8th edition TNM stage (Figure 6).Above all,patients can benefit more from the nomograms in predicting individual survival outcomes.In the IDI analyses,our new nomograms based on LODDS have a superior performance than TNM staging system.IDI of OS nomogram at one year,three years,and five years was as follow:0.061 (P<0.001),0.052 (P<0.001) and 0.033 (P=0.012),respectively.While,for CSS nomogram,IDI at one year,three years,and five years was as follow:0.051 (P<0.001),0.049 (P=0.002) and 0.026 (P=0.042),respectively.The NRI values for 1-,3-,and 5-year OS were 0.127 (95% CI,0.033-0.290),0.123 (95% CI,0.010-0.185), and -0.005 (95% CI,-0.068-0.287),respectively.And for CSS,the NRI values were 0.111 (95%CI,-0.021-0.215),0.076 (95% CI,-0.017-0.190) and 0.023 (95% CI,-0.077-0.219),respectively.
Discussion
In this study,we extracted data of SRC patients from the public SEER database to construct and validate prognostic nomogram model including LODDS for predicting OS rate and CSS.Six prognostic variables,age,race,LODDS,T stage,M stage and tumor size were included in OS nomogram.While CSS nomogram included age,LODDS,T stage,M stage and tumor size.The discrimination of our nomogram was superior to over the AJCC 8th edition TNM staging system alone both in OS and CSS.The calibrations of nomogram showed considerable performance,which were verified both internally and externally.Our nomograms based on LODDS have a more accurate and convenient prognostic evaluation.IDI and NRI values revealed positive improvements in predicting 1-year and 3-year survival probability,although there was no strong improvement in predicting 5-year survival probability between the two models.Furthermore,DCA proved that our novel nomogram models obtained more clinical net benefit than the AJCC staging system across a range of threshold probability.These results showed our nomograms would be helpful to develop appropriate therapeutic strategies for more efficient treatment of SRCpatients.
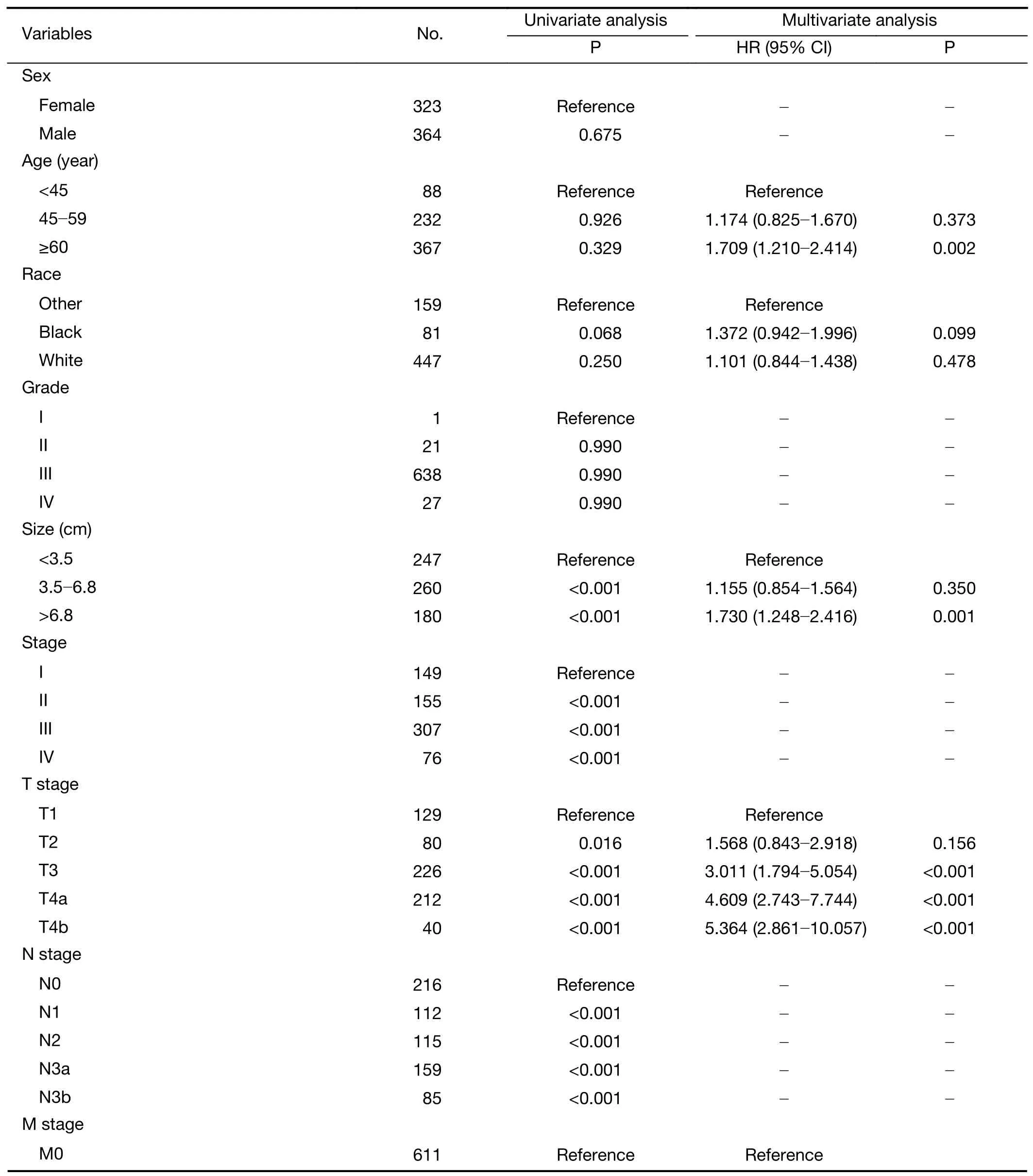
Table 3 Univariate and multivariate analysis of CSS in training cohort (N=687)
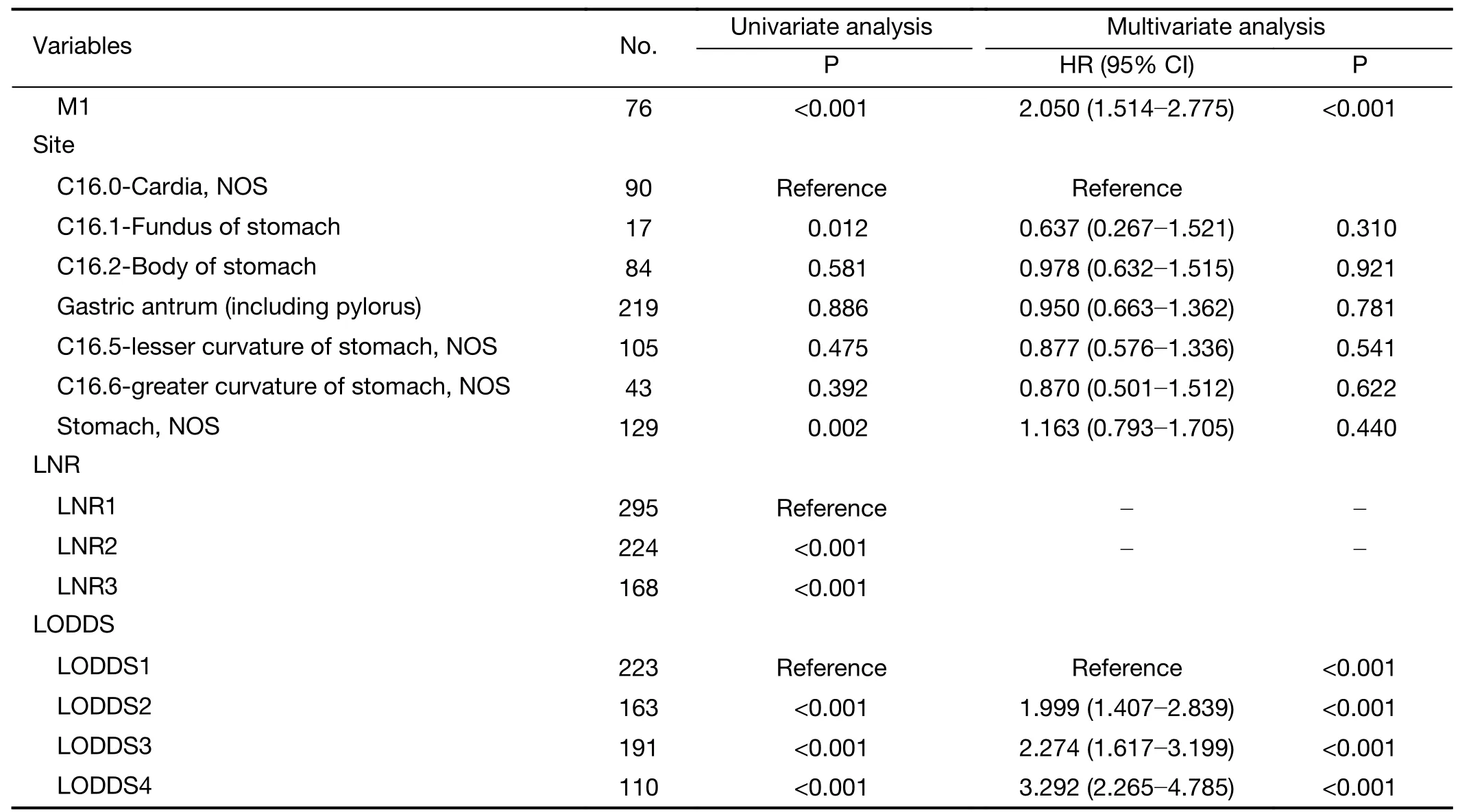
Table 3 (continued)

Table 4 Prognostic efficiency of different lymph node staging systems of OS in training cohort

Table 5 Prognostic efficiency of different lymph node staging systems of CSS in training cohort
The reason why this study focused on SRC nomagram is that the prognosis of SRC remains controversial.The survival of SRC patients was relatively better than other histological types in early stage,which was mainly reported in Asian countries (4,9,20,21).Probably because the tumor of SRC is more frequently observed with superficial spreading and depressed lesions and shows a lower rate of lymph node metastasis (10,22).However,a French study did not demonstrate drastic difference (23).With regard to advanced gastric cancer,many researches from Asia reported that SRC was associated with poor OS rate(9,10,24).Meanwhile,Jianget al.observed no significant difference of prognosis between SRC patients and other histological types in advanced gastric cancer (25).According to a large cohort research from the United States,SRC was not a prognostic indicator after the adjustment for the tumor stage (26).Overall,developing a unique nomogram that directly targets SRC patients,rather than general gastric cancer patients,could have a greater clinical value.The novel nomogram models have a high potential in individualized treatments and disease management.
For better applicability by other institutions or regions,it is crucial to reduce the influence of difference in pathological examination and surgical methods on prognosis.Thus,we only selected those patients diagnosed with SRC after 2010.Previous studies have revealed that examining more than fifteen lymph nodes could improve the accuracy of predicting prognosis in gastric cancer (27).And a large multicenter study from China demonstrated retrieval of more than 30 lymph nodes could be helpful for clinicians to more accurately evaluate the prognosis (28).Also,due to the effect of stage migration,the increased survival rate was shown in many studies as the quantity of examined lymph nodes increased (29,30).The AJCC staging system recommended that at least sixteen lymph nodes were assessed for more accurate staging,with low risk for stage migration and better survival (31).In this study,nearly 40% of patients failed to reach sixteen or more lymph nodes examination,the median amount of lymph node dissections was 18 (IQR,12-27).This result represented that part of patients failed to receive adequate lymph node dissection.Inadequate lymph node dissection will inevitably affect evaluation of actual amount of lymph node metastases,and then affect the reliability of N stage,which also means that AJCC 8th version was still insufficient in clinical practice.
To reduce the effect of stage migration,we adopted LNR and LODDS which were proposed to predict the prognosis more effectively and improve the description of lymph node status.The number of studies had revealed that the LODDS staging system may better stratify patient survival than the AJCC lymph node staging system (13-16,32),which was validated in this research.Additionally,we compared the predictive power of LNR,LODDS and N stage in 8th edition of the AJCC.The results showed that LODDS was found as a more satisfying prognostic indicator for predicting OS and CSS by comparing Cindex,AUC and AIC of three lymph nodes staging systems(Table 4,5).By using the multivariate analysis,our research identified LODDS was an independent prognostic determinant of affecting prognosis of SRC patients.In addition,LODDS was a superior node staging scheme than AJCC N stage and LNR in theory.Furthermore,not only the absolute quantity of positive lymph nodes but also the amount of negative lymph nodes was taken into consideration on LODDS.So it has a better discriminatory power especially in patients with no lymph node involvement or with all lymph node involvement (13-15).All above,LODDS has a broad application prospect in clinical practice.
Some other independent prognostic indicators from routine clinical practice were consisted in our nomograms.Age has been confirmed as a vital prognostic variable in previous studies (33).In this research,our results confirmed that age was a significantly independent poor prognostic factors through multivariate analysis.The middle age group was at greater risk over the young age group in OS rate.Moreover,the old age group had the highest risk both in OS and CSS.As is shown in our research,the old age group had a significantly different prognosis with the young age group.Thus,the influence of age should not however be underestimated and it plays an important role in clinical treatment decision making.
Our findings indicate that tumor size is also of great value in predicting prognosis.On the basis of our results,patients in group of tumor size of 3.5-6.8 cm was at a higher risk than those in group of tumor size <3.5 cm both in OS rate and CSS.Moreover,group of tumor size >6.8 cm indicated a significantly worse prognosis.Previously,Zhouet al.reported that SRC patients with tumor size ≥4.9 cm usually had a poor prognosis (34).Large-size group was more prone to invasive growth,metastasis of lymph node,and distant metastasis characterized by peritoneal dissemination compared with small-size group,all of which were associated with a worse prognosis (34-36).Notably,our research observed patients with tumor size >6.8 cm were significantly associated with poor prognosis,which was identified as an independent prognostic factor.The effects of tumor size on SRC and its intrinsic features largely remain unexplored.It could be insufficient to clarify its clinical value and prognosis by using simple cut-off points of tumor size=5 cm.
Thus,on the basis of the SEER database,we established nomograms based on the LODDS system to predict OS rate and CSS of SRC patients.Our nomograms displayed higher accuracy and comparatively better prognostic discrimination than the AJCC 8th edition TNM staging.The validation cohort demonstrated a satisfying ability of prognosis of the nomograms.
Although our nomograms have good accuracy and discrimination,several limitations also deserve to be mentioned.Though SEER is a huge population-based database,vascular infiltration,perineural invasion and surgical details (the extent of lymphadenectomy,D1,D2 or D2+) are not available.Meanwhile validation of our nomogram was only performed in SEER database.Verification of other large sample size and multi-center studies was required to assess the accuracy of this model.Future well-designed studies could improve the nomogram by incorporating these factors based on their predictive power.
Conclusions
Our results identified LODDS was an independent prognostic indicator for SRC patients.A large populationbased study from SEER was used to build a novel prognostic nomogram predicting OS rate and CSS of SRC patients after surgical resection.Our nomograms based on LODDS have a more accurate and convenient prognostic evaluation than the AJCC 8th edition staging system alone.And it can help clinicians formulate suitable individual treatments and conduct personalized prognostic evaluation.
Acknowledgements
None.
Footnote
Conflicts of Interest:The authors have no conflicts of interest to declare.
杂志排行
Chinese Journal of Cancer Research的其它文章
- Separate lateral parametrial lymph node dissection improves detection rate of parametrial lymph node metastasis in early-stage cervical cancer:10-year clinical evaluation in a single center in China
- Hyperthermic intraperitoneal chemotherapy for gastric cancer with peritoneal metastasis:A multicenter propensity scorematched cohort study
- Prognostic factors affecting long-term outcomes in patients with brain metastasis from esophageal carcinoma
- Signatures within esophageal microbiota with progression of esophageal squamous cell carcinoma
- Oral microbiome and risk of malignant esophageal lesions in a high-risk area of China:A nested case-control study
- Current epidemiology of pancreatic cancer:Challenges and opportunities