Comparison of Clinical Value between Right Distal Radial Artery Access and Right Radial Artery Access in Patients Undergoing Coronary Angiography or Percutaneous Coronary Intervention
2020-12-16WenPanHaixiangXuQingjunLiuandJianhuaFan
Wen Pan ,Haixiang Xu ,Qingjun Liu and Jianhua Fan
1 Department of Cardiology,Kunshan Hospital of Traditional Chinese Medicine,Kunshan Aff iliated Hospital of Nanjing University of Chinese Medicine,Suzhou,Jiangsu,China
Abstract
Keywords:distal radial artery access; radial artery access; coronary angiography; percutaneous coronary intervention
Introduction
With the improvement of people’ s living standards,the incidence rate of coronary heart disease is increasing in China.Coronary angiography(CAG) is the main method to diagnose and evaluate the extent of coronary lesions.Campeau [1]f irst described CAG via radial artery access in 1989.With the accumulation of physicians’ experience,radial artery access has become the preferred approach for CAG throughout the world [2].Radial artery puncture has some complications,such as bleeding,hematoma,and radial artery occlusion(RAO).In 2017,for the f irst time,Kiemeneij [3]described radial artery cannulation in the anatomical snuffbox,which may overcome the drawback of traditional radial artery access.
We report our experience to evaluate the feasibility and safety of right distal radical artery access for CAG or percutaneous coronary intervention (PCI)in our hospital.
Methods
Patient Population
We retrospectively analyzed 113 patients who received CAG or PCI through right distal radial artery access or right radial artery access in Kunshan Hospital of Traditional Chinese Medicine between January and October 2018.
The inclusion criteria were as follows:(1) a normal Allen test result,(2) the right distal radial/radial artery can be palpated in the anatomical snuffbox,and (3) suspected coronary heart disease and requirement for CAG or PCI.The exclusion criteria were as follows:(1) absence of radial artery pulsation,(2) history of radial artery use,(3) severe liver or renal failure or abnormal coagulation function,and (4) hemodynamic instability or an emergency.The study was approved by the Ethics Board of our hospital,and informed consent was obtained from all patients before their participation in the study.
Puncture Methods
All patients took aspirin (300 mg) and ticagrelor(180 mg) before the operation.If the patient took 100 mg aspirin daily,only ticagrelor (180 mg) was taken before the operation.The patient lay supine on a platform in the catheterization laboratory and the right arm was positioned on a side board.The operators randomly determined the primary puncture access.The operators reconf irmed the pulse in the artery and determined which points were suitable for puncture.After subcutaneous injection of lidocaine,a modif ied Seldinger puncture was performed in the right radial artery or the anatomical snuffbox.A 6 F radial artery sheath was inserted carefully after successful puncture (Figure1).Then 200 μ g of nitroglycerin and weight-based heparin were administrated via the artery after successful insertion of the sheath.Angiography was performed through 5 F Judkins diagnostic catheters.If the operator failed to penetrate the radial artery three times or the catheters could not pass through the tortuous or cramped arteries,the operator switched to another arterial puncture access.
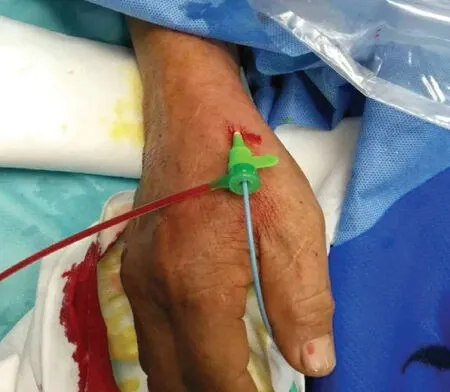
Figure1 A 6 F Sheath Inserted into the Right Distal Radial Artery.
Bandaging and Hemostasis
In both groups,the catheter sheaths were removed immediately after CAG or PCI.In the right distal radial artery group,a small pile of gauze and a semielastic bandage were used for hemostasis for several hours.In the right radial artery group,a TR band (Terumo Medical) was used for hemostasis.Nurses checked the puncture site every hour and adjusted the tightness if necessary.The puncture site was checked for the presence of a radial pulse before discharge.Patients who were suspected of having RAO caused by radial artery thrombosis (weak or no pulse) underwent Doppler ultrasonography.After the operation,the antiplatelet drug regimen was adjusted according to the patient ’ s CAG results.
Data Collection
We collected general characteristics,the rate of successful radial artery puncture,the rate of successful catheter placement,the number of puncture attempts,the access time,and postoperative compression time and complications (bleeding,hematoma,and RAO) for the two groups.
Statistical Analysis
SPSS Statistics 17.0 was used for the statistical analysis.Continuous variables were expressed as the mean ± standard deviation,and categorical variables were expressed as the number and percentage.Thettest was used for comparisons between the two groups,and categorical variables were analyzed by aχ2test.P < 0.05 was considered a statistical difference.
Results
General Characteristics of the Patients
Fifty-two patients were enrolled in the right distal radial artery group and 61 patients were enrolled in the right radial artery group.The differences in sex,age,body mass index,hypertension,diabetes,stroke,atrial f ibrillation,and smoking rates,and left ventricular ejection fraction between the two groups were not statistically signif icant (Table1).
Procedural Characteristics for the Two Groups
Fifteen patients underwent PCI in the right distal radial artery group and 20 patients underwent PCI in the right radial artery group (28.85%vs.32.79%,P = 0.652).The number of puncture attempts (2.19 ± 0.53 vs.1.26 ± 0.44,P = 0.048) was greater and the access time (4.77 ± 1.49 min vs.3.23 ± 0.86 min,P < 0.05) was longer but the compression time (3.44 ± 0.92 h vs.7.16 ± 1.2 h,P < 0.05)was shorter in the right distal radial artery group.The rate of successful artery puncture (94.23% vs.100%,P = 0.057) and the rate of successful catheter placement (88.46% vs.91.80%,P = 0.367) in the two groups were not statistically different (Table2).
Complications Related to Puncture
A small hematoma (< 5 cm) in f ive patients and localized bruising in one patient in the right radial artery group were managed conservatively.There were two cases of bleeding after TR band removal in the right radial artery group.Doppler ultrasonography conf irmed RAO in one patient in the right radial artery group.There was no statistical difference in the incidence of hematoma (1.93%vs.6.56%,P = 0.232),bleeding (0% vs.3.28%,P = 0.188),or RAO (0% vs.1.64%,P = 0.354) in the two groups of patients.But the rate of total complications (1.93% vs.11.48%,P = 0.048) in the right distal radial artery group was considerably lower than in the right radial artery group (Table3).
Discussion
The anatomical snuffbox is a depression in the wrist’ s radial part,limited by the tendons of theabductor longus muscle,extensor pollicis brevis muscle,and extensor pollicis longus muscle[4] (Figure2).The study by Valsecchi et al.[5]suggests that the diameter of the snuffbox artery is 2.22 ± 0.14 mm and that of the proximal radial artery is 2.64 ± 0.13 mm.So a 6 F sheath can be inserted into the distal radial artery in normal circumstances.
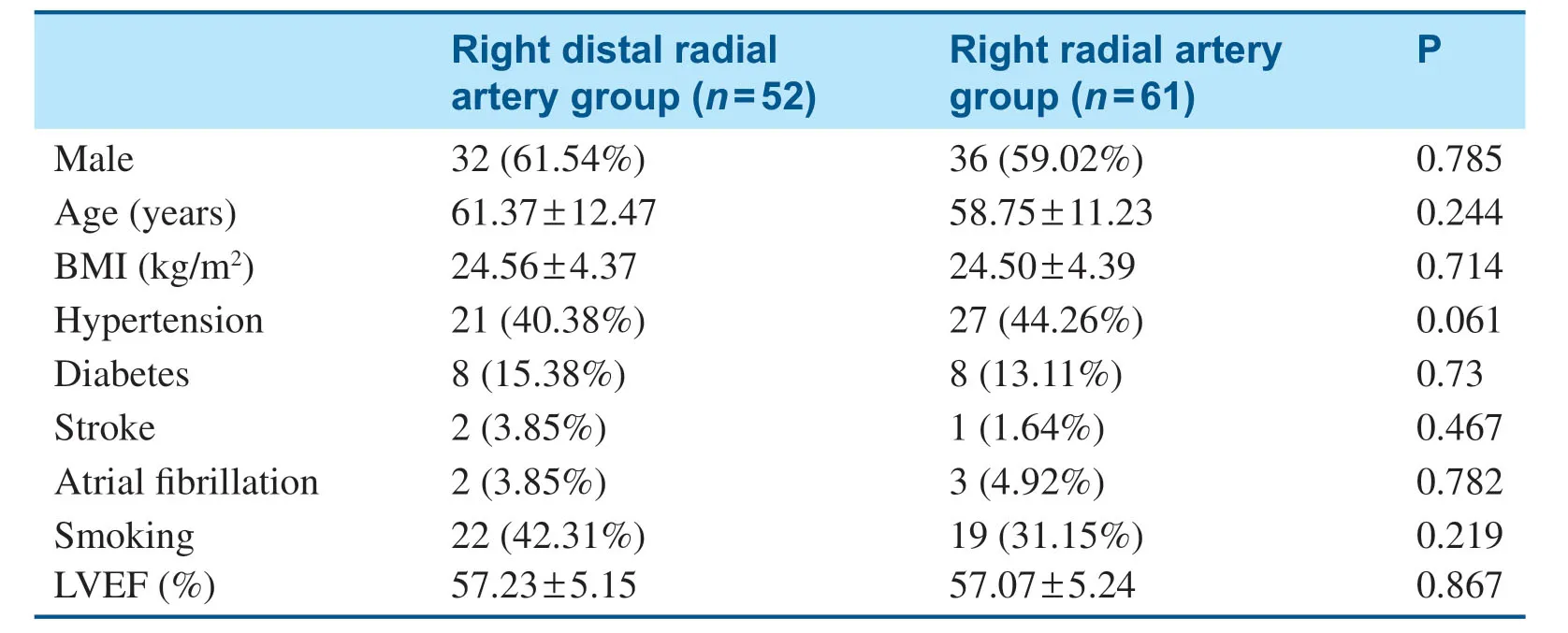
Table1 General Characteristics of the Patients in the Two Groups.
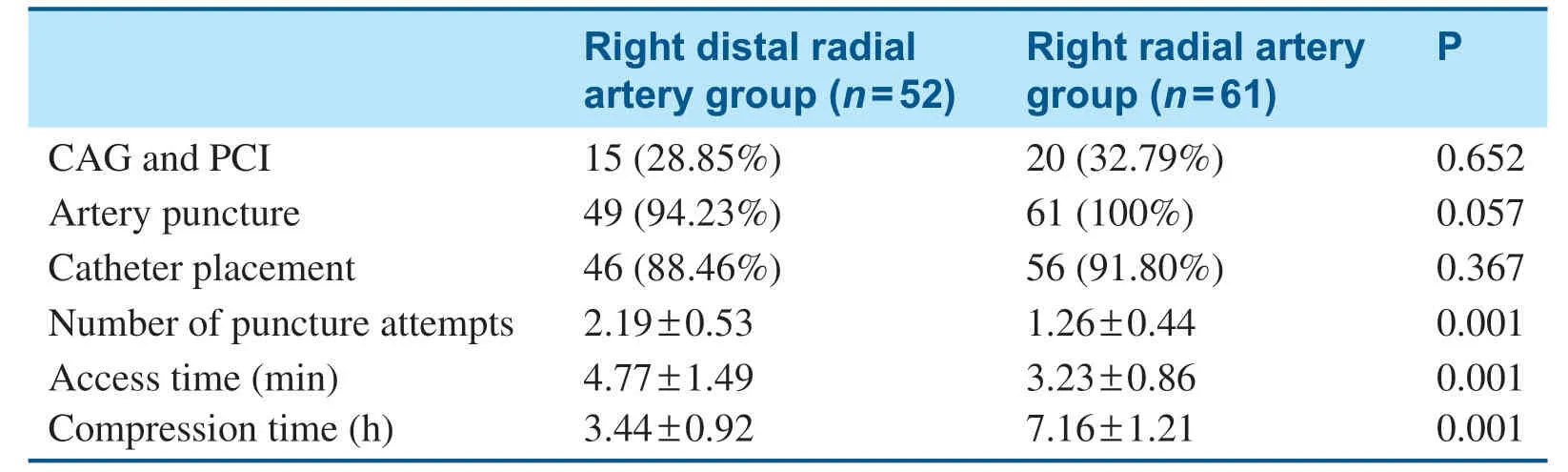
Table2 Procedural Characteristics for the Two Groups.
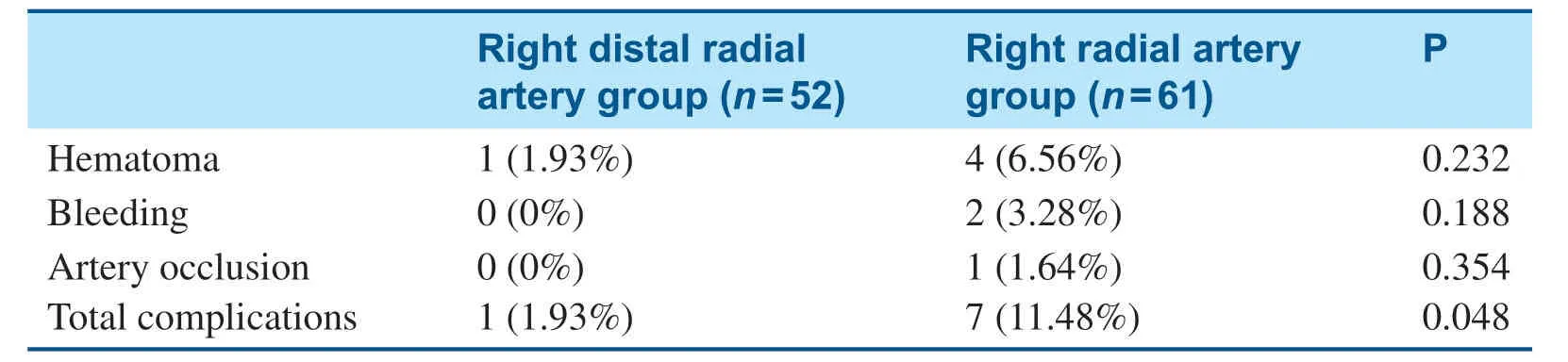
Table3 Complications Related to Puncture in the Two Groups.

Figure2 The Anatomical Relationship of the Distal Radial Artery in the Anatomical Snuffbox and Surrounding Tendons.
Our study showed that patients in the right distal radial artery group had more puncture attempts,a lower rate of successful catheter placement,a longer access time,a shorter compression time,and a similar PCI ratio.The incidence of RAO after transradial artery access was 2%- 18% in some reports [6].Our research found that the incidence of RAO in the right radial artery group was 1.64%,but no patient had RAO in the right distal radial artery group.We also found that the incidence of hematoma and the incidence of bleeding in the right radial artery group were higher than in the right distal radial artery group.The results of our research are similar to those of previous studies [7,8].
The right distal radial artery group had early hemostasis and a low risk of hematoma and RAO.But the diameter of the distal radial artery is relatively smaller than that of the radial artery so the rate of sheath implantation success is lower and sheath implantation is time-consuming.To shorten the puncture time and implant the sheath successfully,we should select patients carefully as stated by Kar [9].So distal radial artery access is another option for CAG or PCI in suitable patients and saves the radial artery for possible future coronary artery bypass graft.
Limitations
This is a retrospective study with a small number of patients.Large prospective randomized controlled studies are needed to evaluate the clinical value of right distal radial artery access.
Conclusions
Right distal radial artery access isassociated with lower incidence of bleeding and postoperative complications but at the cost of increased time and number of punctures.If the patient is selected appropriately,distal radial artery access is an option.
Acknowledgments
The authors thank their many colleagues who worked together on this project.
Conf ilcts of Interest
The authors declare that they have no conf licts of interest.
Author Contributions
Jianhua Fan collected and analyzed related data.Haixiang Xu and Wen Pan performed operations and wrote the f irst draft.Qingjun Liu and Jianhua Fan edited and corrected the article.
杂志排行

Cardiovascular Innovations and Applications的其它文章
- Epicardial Adipose Tissue in Patients with Obstructive Sleep Apnea:A Systematic Review and Meta-analysis
- Comparison of Segmentation Algorithms for Detecting Myocardial Infarction Using Late Gadolinium Enhancement Magnetic Resonance Imaging
- Current Management Strategies in Patients with Heart Failure and Atrial Fibrillation:A Review of the Literature
- In-Stent Thrombosis after Antiplatelet Therapy Conversion while Awaiting Coronary Bypass
- lmpact of MitraClip Program on the Volume and Outcomes of Mitral Valve Surgery:A Single-Center Retrospective Study
- Clinical Analysis of Transcatheter Embolotherapy for Congenital Pulmonary Arteriovenous Fistulas in Children