Hepatic abscess resulted from a toothpick piercing the gastric wall into the liver
2020-10-23CuiFeiLuoJiXuYunQingLu
Cui-Fei Luo , b , c , Ji Xu , b , c , Yun-Qing Lu , b , c , ∗
a Department of Emergency Medicine, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou 310 0 03, China
b Department of Geriatric Medicine, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou 310 0 03, China
c Zhejiang Provincial Key Laboratory for Diagnosis and Treatment of Aging and Physic-chemical Injury Diseases, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou 310 0 03, China
TotheEditor:
Foreign bodies’ ingestion is a common phenomenon, and most of the ingested foreign bodies pass through the gut uneventfully.In clinical practice, less than 1% of these patients develop complications such as gut wall penetration or perforation [1-3].We present a rare complication of hepatic abscess secondary to the toothpick piercing the gastric wall into the liver.The abscess was successfully treated by endoscopic retrieval of the foreign body and empirical antibiotic therapy, without drainage or laparotomy.
A 65-year-old woman was admitted with a two-week intermittent epigastric pain and a 2-day exacerbation associated with fever.Upon admission, she weighed 62kg and had a temperature of 38.9 °C, heart rate of 112 beats/min, respiratory rate of 24 times/min, and blood pressure of 105/62 mmHg(1 mmHg = 0.133 kPa).Physical examination revealed unremarkable, except for upper abdominal tenderness, and the electrocardiogram was also normal.
Laboratory tests showed a white blood cell count of 15.1 ×109cells/L with 83.9% neutrophils and 7.4% lymphocytes, hemoglobin concentration 13.0 g/dL, and platelet count 319 ×109cells/L.The C-reactive protein level was 22.2 mg/L (reference range 0-8.0 mg/L), procalcitonin level was 38.5 μg/L (reference range 0-0.5 μg/L) and interleukin-6 (IL-6) level was 94.7 pg/mL (reference range 0.1-2.9 pg/mL).The cardiac, liver and renal function tests and blood clotting index were all normal.In general, laboratory results indicated that she was in a state of severe bacteria-induced inflammation.
The emergency physician performed abdominal computed tomography (CT) scan.The abdominal CT and three-dimensional reconstruction showed a hyperdense linear foreign body in the stomach body piercing into the liver directly, thickened gastric wall edema, and hypodense foci in the lateral segment of left lobe of the liver, considering hepatic abscess caused by the foreign body( Fig.1 ).Emergency gastroscopy revealed a long foreign body piercing the posterior wall of the stomach ( Fig.2 A).Endoscopic retrieval was performed to remove the foreign body which turned out to be a 6.0-cm-long wooden toothpick ( Fig.2 B).Positive treatments, such as broad-spectrum antibiotics and nutrition support,were applied afterwards, and the patient recovered well and was discharged 2 weeks later.Following up on her medical history, the patient had the habit of using toothpicks, but she could not accurately recall when the toothpick was swallowed.Thus, the patient was diagnosed as hepatic abscess caused by the toothpick piercing the gastric wall into the liver which formed sinus tract for bacteria.Follow-up ultrasonography (USG) confirmed that hepatic abscess was completely resolved two months after discharge.
Gastrointestinal tract perforation occurs in less than 1% of patients who ingested foreign bodies.The most common sites are stomach, duodenum and colon [1,4].Though the types of ingested gastrointestinal foreign bodies were diverse according to the personal dietary habit and community sociocultural features,fish bones and toothpicks were the most commonly implicated foreign bodies [ 1 , 3 , 5 ].Metallic foreign bodies were also been reported, including needle, clothespin, pen, and wire [5].The size of the foreign body was wide-ranging from 1 cm (fish bone) to 19 cm(toothbrush) [ 1 , 5 ].The migrated foreign body-induced hepatic abscess is rare, and usually represents 1% −5% of hepatic abscesses.Since the first case was reported by Lambert in 1898, less than 100 cases have been reported until now [6].Hepatic abscess caused by the toothpick penetration of gastrointestinal tract is even more rare, and most patients were treated surgically [ 1 , 6 ].The left lobe was the most frequently affected area in the location of hepatic abscess, followed by the right lobe, and bilobar involvement [1].There are several reasons for a predominance of left lobe in hepatic abscess secondary to foreign body migration: the close anatomic proximity to the gastroduodenal region which is the most common site when gastrointestinal tract perforation occurs, and the physical stenosis of pyloric sphincter that traps the foreign body [7].However, the mechanism in right lobe abscess is more complicated and variable.
The clinical symptoms of hepatic abscess due to the ingestion of foreign bodies are non-specific and elusive, and it is important to recognize such case timely and accurately.According to the Euro-pean Society of Gastrointestinal Endoscopy Guideline, conventional radiography (e.g.X-ray) is recommended to evaluate the presence,location, size, and configuration of foreign bodies if the radiopaque objects (e.g.metal, graphite, and stone) are suspected, while a CT scan is recommended in all patients with suspected symptoms or similar complications [ 3 , 8 ].Clinically, USG may be the most convenient tool for detecting radiolucent foreign bodies and hepatic abscess in emergency situation because of its widely available and accessible, as well as of high resolution (150μm), specificity and sensitivity in detecting radiolucent objects [9].However, the success of USG requires a pretest suspicion of foreign body and its general anatomic location.Therefore, USG is better applied for assessing detailed location and configuration of foreign body after the diagnosis [7].In fact, CT is a preferred imaging examination for diagnosis due to its high resolution and accuracy in identifying foreign bodies and evaluating the complications of gut wall penetration [9].The most commonly used diagnostic modality was CT, followed by USG, plain radiography, and laparotomy; even the combination of USG and CT, plain radiography and CT, and even the triple combination of plain radiography, USG and CT were also applied when necessary [1].
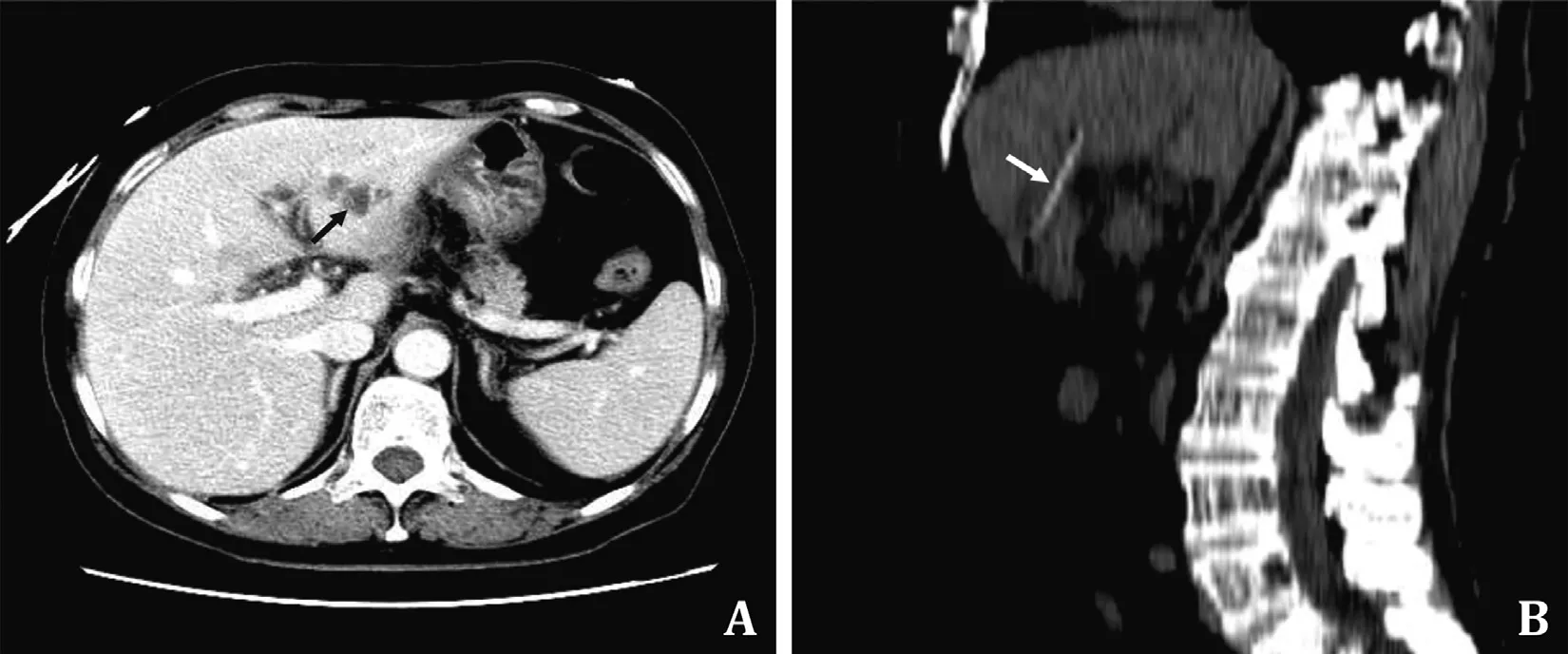
Fig.1.Imaging studies with abdominal contrast-enhanced computed tomography and three-dimensional reconstruction.A: contrast-enhanced computed tomography showing a hypodense mass representing hepatic abscess (arrow) in the left lobe of the liver; B: abdominal multiplanar reconstruction showing a hyperdense linear foreign body(arrow) directly piercing into the liver.

Fig.2.Images of removing foreign body from the stomach.A: endoscopic retrieval of the toothpick piercing the posterior wall of stomach body; B: a 6-cm long wooden toothpick retrieved.
In this case, an initial noncontrast CT scan followed by a contrast-enhanced CT indicated the foreign body piercing the gastric wall into the liver directly, without evidence of notable pancreatic or vascular injury.We implemented the successful conservative management by combining endoscopic removal of the toothpick and empirical antibiotic therapy, without drainage or laparotomy.Emergency physicians should be alerted to these rare diseases with early detection and treatment for a good prognosis.
Acknowledgments
None.
CRediT authorship contribution statement
Cui-Fei Luo:Data curation, Formal analysis, Writing - original draft.Jia Xu:Writing - original draft, Writing - review & editing.Yuan-Qiang Lu:Conceptualization, Funding acquisition, Supervision, Writing - review & editing.
Funding
This study was supported by a grant from the Foundation of Key Discipline Construction of Zhejiang Province for Traditional Chinese Medicine ( 2017-XK-A36 ).
Ethical approval
Informed consent was obtained from the patient for the publication of her information and imaging data.
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
杂志排行
Hepatobiliary & Pancreatic Diseases International的其它文章
- Fecal microbiota transplantation has therapeutic effects on chronic hepatits B patients via altering composition of gut microbiota
- The Janus of mIS in hepatobiliary surgery: Importance of maximally invasive surgery in an era of minimally invasive surgery
- Liver injury in COVID-19: What do we know now?
- Is the Bismuth-Corlette IIIb stage really an unfavorable situation for resectability of Klatskin tumors? A critical appraisal
- Pancreatoblastoma: A rare indication for liver transplantation in children
- Optimized liver resection range and perioperative safety in patients with high levels of indocyanine green R15