Monocyte-to-lymphocyte ratio as a prognostic factor in peripheral whole blood samples of colorectal cancer patients
2020-09-23KatarzynaJakubowskaMariuszKodaMagorzataGrudziskaLuizaKaczugaKodaWaldemarFamulski
Katarzyna Jakubowska, Mariusz Koda, Małgorzata Grudzińska, Luiza Kańczuga-Koda, Waldemar Famulski
Abstract
Key words: Monocyte count; Monocyte to lymphocyte ratio; Platelet; Neutrophil-tolymphocyte ratio; Colorectal cancer; Prognosis
INTRODUCTION
According to the latest data, colorectal cancer (CRC) is the third most common malignancy worldwide. It is estimated to be the third leading cause of death due to cancer in both males and females[1]. The appearance of regional lymph-node metastasis in CRC is a relevant risk factor for the development not only of regional recurrences but also distant metastatic lesions[2]. Distant metastases are the main cause of death in CRC patients. It is assessed that roughly one-fifth of CRC patients will have liver metastases. A significant number of patients die within 5 years[3]. Surgery is the most frequent and primary treatment in non-metastatic CRC. In addition, patients with stage II and III undergo chemotherapy based on 5fluorouracil[4]. Early identification of patients with a poor prognosis could optimize treatment. It is currently believed that the characteristics of a tumour mass are insufficient to determine prognosis and treatment.
A systemic inflammatory response is related to tumour progression[5]. In addition, inflammatory cells are key players in the tumour microenvironment[6]. Their count can be measured by simple laboratory tests. The available data on peripheral blood cells in cancer patients show that a rise in monocyte count in the peripheral blood is a predictive factor of a poor prognosis in patients with hepatocarcinoma or stomach cancer[7,8]. In another study, monocyte count was an independent factor correlated with survival in patients with metastasis from CRC[9]. Another important parameter is the monocyte/lymphocyte ratio (MLR). In recent times, the MLR has been investigated in patients with solid tumours. The monocyte level divided by the lymphocyte level may be an efficient prognostic indicator in tumours[10,11]. The neutrophil/lymphocyte ratio (NLR) has been described as a prognostic factor dependent on CRC stage. The NLR ratio was found to be higher in cases with more advanced disease[12]. Another inflammation-based marker is the combination of platelet count (PLT) and NLR (PLT–NLR status). This indicator was examined to predict survival in patients with gastric cancer[13]. Identifying novel prognostic markers of CRC may help identify patients at high risk and choose appropriate treatment in selected cases.
Therefore, the aim of the present study was to investigate the correlation of monocyte count, MLR, neutrophil-to-monocyte ratio (NMR), NLR-PLR status and PLT-NLR status with clinical outcome in CRC patients.
MATERIALS AND METHODS
Baseline characteristics of the study group
We retrospectively reviewed the medical records of 160 patients diagnosed with CRC (96 men and 64 women) who underwent surgery in the Department of Oncological Surgery, Comprehensive Cancer Centre (Bialystok, Poland) between April 2014 and December 2016. The mean age of the patients was 67.5 years, including 40 patients < 60 years old and 120 patients ≥ 60 years old. The majority presented similar symptoms, including abdominal pain, anaemia, rectal bleeding, constipation, diarrhoea, vomiting and anorexia. In most cases, patients additionally received treatment for hypertension, type II diabetes, osteoarthritis and coronary heart disease. However, none of the patients had received anti-inflammatory therapy. All patients underwent routine diagnostic tests, including basic diagnostic laboratory tests (morphological tests and lipid profiles), electrocardiography, spirometry, arterial blood gas analysis, X-ray and chest computed tomography. The clinical stage of CRC was evaluated according to the Tumour-Node-Metastasis (TNM) classification[14]. Prior to surgery, patients with tumours identified in other sites had not received anti-inflammatory or immunosuppressive therapy.
Patients diagnosed with neoplasms in the rectum received preoperative therapy (n= 53). They received radiotherapy (n= 39), chemotherapy (n= 7) and radiochemotherapy (n= 7), and received a dose of 25 Gy in fractions of 5 Gy during one week in the pelvic area. The response to preoperative therapy was estimated according to the Response Evaluation Criteria in Solid Tumours[15]. Stable disease was observed in 26 patients, while 27 patients had a partial response.
The inclusion criteria were as follows: (1) Pathologically confirmed CRC; (2) Treatment with radical resection; and (3) No previous anti-inflammatory therapy. The exclusion criteria were: (1) Incomplete clinicopathological and follow-up data; and (2) Presence of haematological disorders.
Tissues obtained from surgery were fixed in 4% buffered formalin for 24 to 72 h at room temperature. Small sections of tissue were embedded in paraffin. Sections (4 µmthick) were cut from paraffin blocks and stained with haematoxylin and eosin (HE) at room temperature for 4 min (cat. no. 468802128; POCH S.A.; Avantor Performance Materials Poland, Gliwice, Poland) according to the manufacturer's protocol. The slides were deparaffinised in an oven at 60°C for 5 min. The slides were subsequently rehydrated in xylene (three washes, 10 min each) and graded ethanol (100%, 95%, 85% and 75%, 1 min at each concentration). The type of tumour growth, tumour size, histological type, percentage of mucinous component, grade of malignancy and TNM stage were determined by pathologists. Venous, lymphatic and perineural invasions of cancer cells were also analysed. Characteristic features of lymph node invasion were examined, including the number of resected and invaded lymph nodes, the presence of micro- and macro-metastases, invasion of the pouch lymph node, the presence of distant metastases and the size of metastases. The presence, number and size of cancer cell deposits were also assessed[16].
Blood sample examination
Blood samples were obtained within 3 d before and after surgical treatment. Venous blood samples were also obtained from 42 healthy controls (female: 21, male: 21; mean age: 45 years old; min-max: 25-65 years old). The differential white blood cell count was determined using an XN-1000 automated haematology analyser (Sysmex Co., Kobe, Japan).
We analysed monocyte count and the MLR in whole blood before and after surgery of patients with CRC. The MLR was defined as the absolute monocyte count divided by the absolute lymphocyte count. Receiver operating characteristic (ROC) curve analysis was used to investigate cut-off values of the pre- and postoperative monocyte count (preMONO/postMONO) and MLR (preMLR/postMLR). The cut-off of pre- and postoperative monocyte count were 0.39 and 0.68 with sensitivity (preMONO-75.8%; postMONO-27.89%) and specificity (preMONO-16.67%; postMONO-85.71%) The area under the ROC curve for pre and post monocyte count had weak prognostic value in CRC patients (0.505 and 0.532). Moreover, the cut-off of pre- and postoperative MLR was 1.46 in both cases. The sensitivity and specificity of analysis in preoperative blood samples were 94.27% and 73.81% and were similar to those in postoperative samples (90.41% and 73.81%). The area under the ROC curve for pre and postNMR showed that the parameter exhibits strong diagnostic power (1.000). Pre and post MLR had moderate diagnostic power of 0.751 and 0.746. Patients were divided into the high and low groups according to the cut-off values in pre- and postoperative blood samples.
The NLR-PLR was calculated according to Hiraharaet al[17]. The NLR-PLR status consists of two parameters: NLR (the absolute neutrophil count divided by the absolute lymphocyte count) and PLR (the platelet count divided by the absolute lymphocyte count). The cut-off values were 2.5 and 267.3, respectively. Patients with low values of both parameters (NLR < 2.5, PLR < 267.3) were scored as group 0. Score 1 consisted of one high parameter: NLR (> 2.5) or PLR (> 267.3). Score 2 was generated by combining both high parameters (NLR > 2.5, PLR > 267.3). The PLT-NLR status was generated by PLT with the NLR score. The cut-off values were 300 and 2.5 based on the ROC curve. Score 0 was calculated as PLT (< 300) and NLR (< 2.5). Patients with either elevated NLR or PLR were allocated to score 1. Patients with both increased NLR (> 2.5) and PLR (> 300) were in group 2. For disease-free survival (DFS) analysis, we divided the study group into two subgroups with score 0 and score 1 + 2.
Follow-up data
Patients were followed up for 2-5.0 years. They were monitored by the measurement of carcinoembryonic antigen and CA19-9 levels, physical examination, colonoscopy or/and radiological imaging including computed tomography of the chest, abdomen and pelvis, bone scan, and positron emission tomography scans. Local and distant recurrences were defined as pathologic evidence of the spread of tumours in the region of anastomosis (local recurrence) or/and present outside the primary tumour at other sites such as liver, lungs, bones, brain (distant recurrence) and confirmed by the techniques mentioned above.
Statistical analysis
Statistical analysis was performed using the STATISTICA 13.0 program. Comparisons between groups were analysed using the independent-samplest-test, and comparisons within groups were analysed using the pairedt-test. Enumeration data were analysed using theχ2test. Comparisons among multiple groups were analysed using one-way ANOVA. DFS time was calculated as the duration between the date of diagnosis and the date of disease progression, including local or distant relapse. The DFS rate was estimated using the Kaplan Meier estimator method and the survival curves were compared using log-rank tests. Prognostic factors were assessed using univariate and multivariate analyses (Cox proportional hazard regression model). APvalue < 0.05 was considered statistically significant.
RESULTS
The clinicopathological characteristics of patients with colorectal cancer
The study group was heterogeneous in terms of sex (40% female, 60% male) and age (25% < 60 years old, 75% > 60 years old). Tumour locations were the right-side of the colon in 20 patients (12.5%), transverse colon in 14 patients (8.75%), left-side in 15 patients (9.37%), sigmoid colon in 29 patients (18.12%) and rectum in 82 patients (51.25%). There were 42 (26.25%) patients with TNM stage I, 31 (19.37%) with stage II, 69 (43.12%) with stage III and 18 (11.25%) with stage IV. In more than 92% of patients the grade of malignancy was determined as 2. Tumour size was between 2.5 and 5.0 cm in 106 patients (66.25%). Among 160 evaluable patients, only 17 had distant metastasis. Lymph-node metastasis was found in almost half of patients in the study group (49.37%). The presence of venous invasion and lymphatic invasion was determined in 46 and 38 patients, respectively. The complete characteristics of the study group are shown in Table 1.
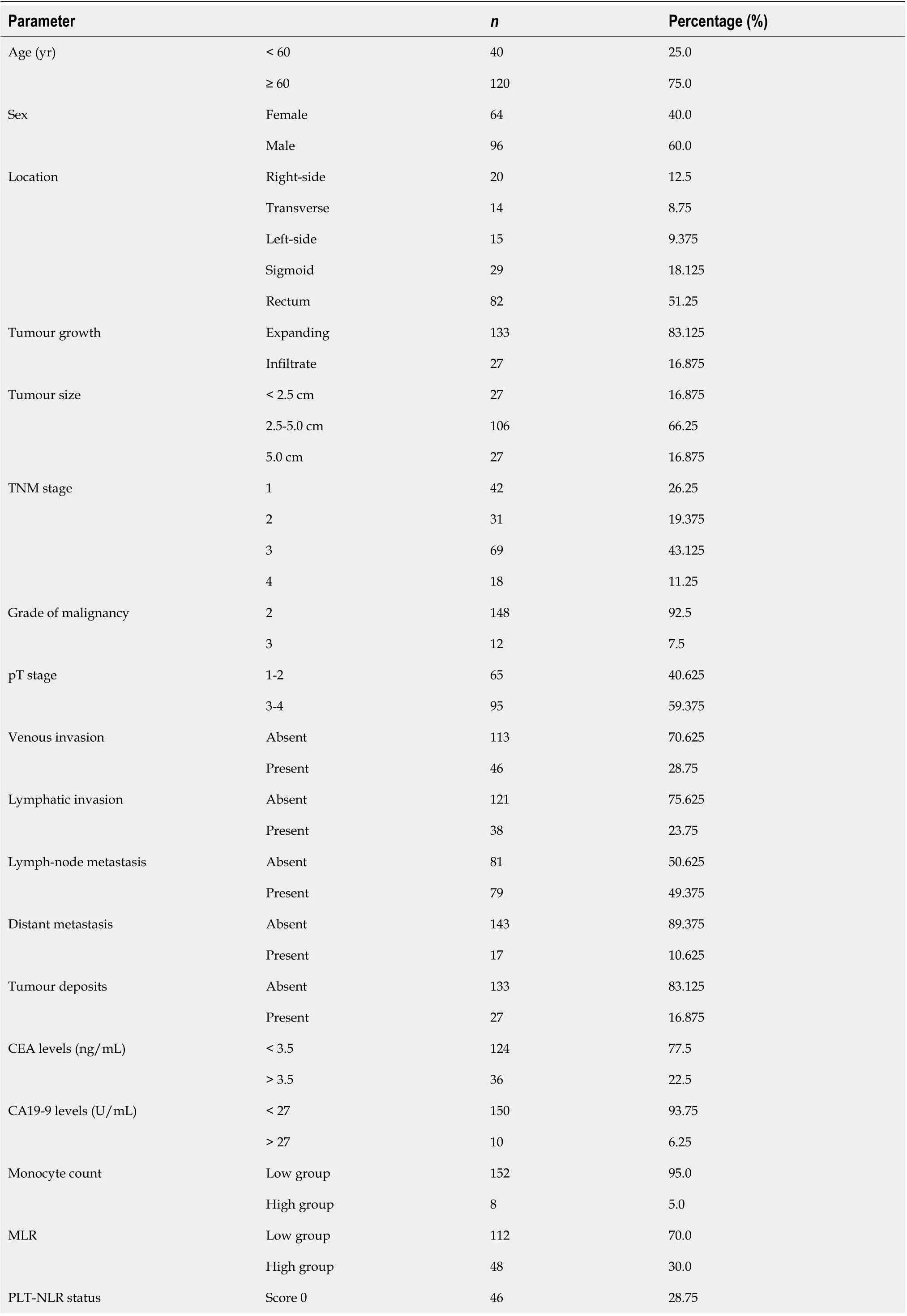
Table 1 Characteristics of the study group (n = 160)

TNM stage: Tumour-Node-Metastasis; CEA: Carcinoembryonic antigen; CA19-9: Carbohydrate antigen 19-9; MLR: Monocyte-to-lymphocyte ratio; PLTNLR status: Platelet and neutrophil-to-lymphocyte ratio; NLR-PLR status: Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio.
Correlation between monocyte count, monocyte to lymphocyte ratio, neutrophil-tolymphocyte ratio and platelet-to-lymphocyte ratio status, platelet and neutrophil-tolymphocyte ratio status and clinicopathological variables in colorectal cancer patients
The correlations between monocyte count and MLR and anatomoclinical variables were published previously. The PLT-NLR status calculated based on the preoperative blood samples was correlated with tumour size and the presence of perineural invasion (P= 0.015;P= 0.037). Moreover, high values of NLR-PLR and PLT-NLR in the blood samples obtained after surgery were positively associated with histological type of the cancer and the percentage of mucinous component (NLR-PLR:P= 0.002;P= 0.009; PLT-NLR status:P= 0.002;P= 0.007). We found no correlation between NLRPLR and PLT-NLR and any other variables such as age, sex, TNM stage, lymph node status, the presence of distant metastasis and cancer cell deposits. These results are shown in Table 2.
Prognostic values of monocyte count, monocyte to lymphocyte ratio, neutrophil-tolymphocyte ratio and platelet-to-lymphocyte ratio status and platelet and neutrophilto-lymphocyte ratio status in colorectal cancer patients
The median 3- and 5-year DFS time was 11.6 and 27.6 mo, respectively. Patients with a low monocyte count in preoperative blood samples lived approximately 12.3 mo (3-year DFS survival) and 28.3 mo (5-year DFS survival) compared to 8.25 mo (3-year DFS time) and 20.3 mo (5-year DFS time) in those with a high monocyte count. These values for monocyte count differed from each other but they were not statistically significant(P= 0.145;P= 0.138) (Figure 1A and B). In the whole blood samples obtained after surgery, the monocyte count tended to differ significantly for the 5-year DFS time which was 0.084. The mean 3-year and 5-year DFS were 15.7 mo and 27.6 mo in the high group and 11.6 mo and 37.1 mo in the low group (Figure 1C and D). Patients with a higher preMLR value tended to have shorter 3- and 5-year DFS time(P= 0.248,P= 0.122) (Figure 1E and F). Patients with low postMLR had longer 3- and 5-year DFS time(P= 0.031,P= 0.049) (Figure 1G and H). Analysis of the NLR-PLR status measured after surgery showed only a tendency for shorter 5-year DFS in the low group(P= 0.054) (Figure 2A-D). Moreover, the results of the PLT-NLR status obtained after surgery showed a tendency for shorter 3- and 5-year DFS in the low group as compared to the high group(P= 0.071;P= 0.072) (Figure 2E-H).
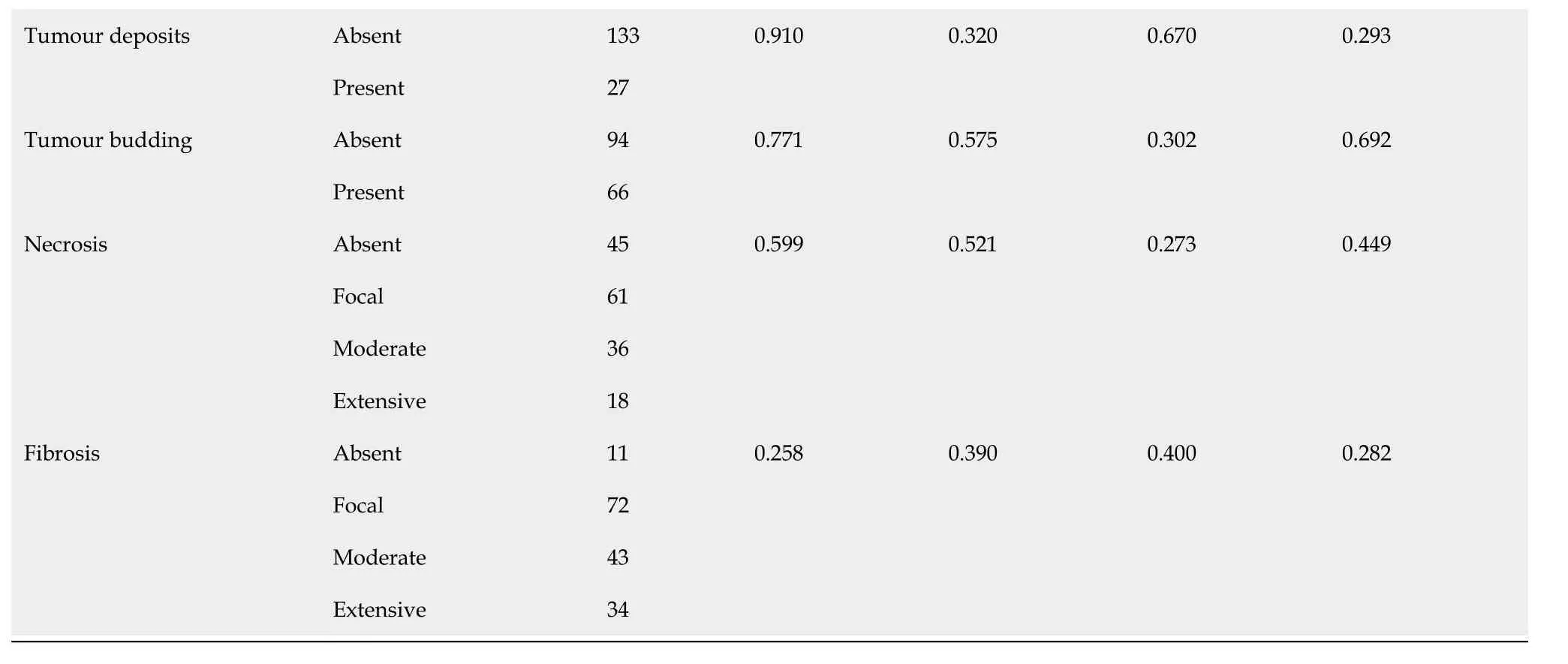
Factors found to be predictive of 3-year DFS in univariate Cox regression analysis included: The number of lymph nodes removed (HR = 0.415, 95%CI: 0.193-0.890,P= 0.023), invasion of the lymph node pouch (HR = 14.191, 95%CI: 1.458-138.08,P= 0.022), inflammatory cell infiltration in the invasive front (HR = 1.590, 95%CI: 1.011-2.525,P= 0.044) and MLR obtained before surgery (HR = 2.000, 95%CI: 0.814-5.063,P= 0.015). According to the multivariate Cox proportional model, the number of lymph nodes removed(P= 0.020) and inflammatory cell infiltration in the invasive front(P= 0.015) were independent factors of 3-year DFS in CRC. Moreover, the analysis of 5-year DFS showed that the MLR in whole blood obtained after surgery (HR = 2.903, 95%CI: 1.368-6.158,P= 0.005) and the status of lymph node metastasis (HR = 0.813, 95%CI: 0.653-1.013,P= 0.050) were prognostic factors in patients diagnosed with CRC. Using the multivariate Cox proportional model, we demonstrated that only the MLR calculated from whole blood after surgical treatment was an independent factor of 5-year DFS in CRC patients. These results are shown in Tables 3 and 4.
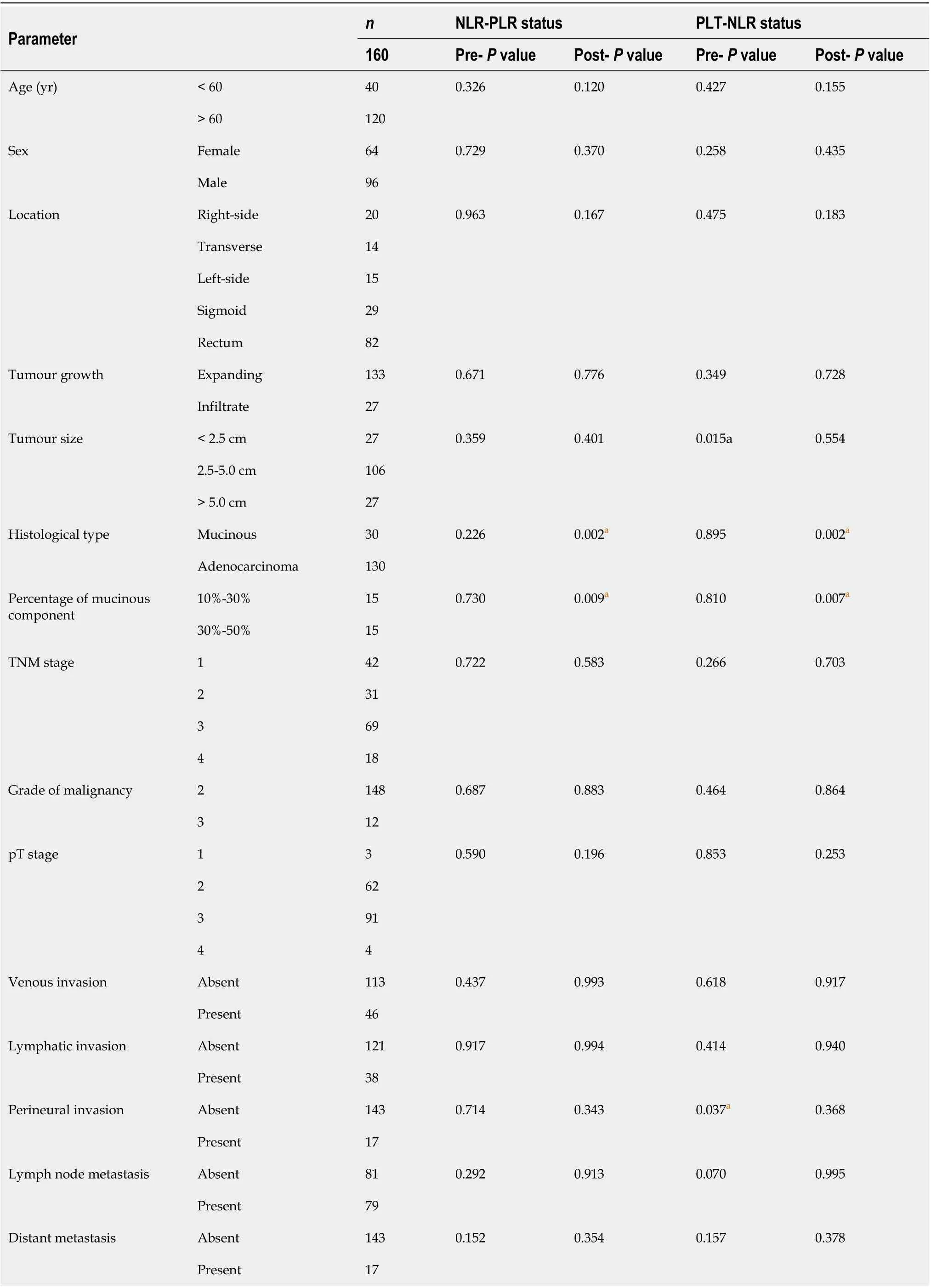
Table 2 Correlations between neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio status and platelet and neutrophil-tolymphocyte ratio status in pre and postoperative whole blood samples and clinicopathological features of patients with colorectal cancer
aP < 0.05. TNM stage: Tumour-Node-Metastasis; PLT-NLR status: Platelet and neutrophil-to-lymphocyte ratio; NLR-PLR status: Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio; Pre: Preoperative blood samples; Post: Postoperative blood samples.
DISCUSSION
Systemic inflammation is closely associated with carcinogenesis. The tumour microenvironment consists of tumour cells and inflammatory cells which release various cytokines and chemokines. Literature data have shown that monocytes appear to be recruited as inflammatory cells with cellular machinery to directly kill malignant cells. They are involved in TRAIL-mediated apoptosisviathe production of interferon alfa[18]. Monocytes are also able to stimulate cancer cell death through Ab-dependent cytolysis and phagocytosis[19]. However, cancer cells appear to protect themselves from phagocytosis in the circulationviachemokine CD47 overexpression. Despite high expression of the ligand for CD47 on the surface of circulating monocytes, they are unable to stop cancer cell invasion through phagocytosis[20]. Multiple reports have documented that monocytes can be responsible for tumour progression, including the early stages of tumour growth and the formation of distant metastases[21]. Both human and mouse models of colorectal and breast cancer have shown that monocytes can be recruited to primary tumours and pulmonary metastases in a CCL2 Monocyte chemoattractant protein-1 (MCP-1/CCL2)-dependent manner[22,23]. In our study we showed that patients with CRC and a low preoperative absolute monocyte count had a tendency for longer 3-year and 5-year DFS. Our results are in contrast with those of Liet al[24]who demonstrated shorter one, three-, five-year overall survival rates in CRC patients with a low absolute monocyte count. Also, Huet al[25]proved that preoperative monocyte counts in peripheral blood samples were associated with 5-year overall survival and appear to be an independent risk factor for liver metastasis of CRC. Sasakiet al[9]and Harukiet al[26]observed that an increase in preoperative peripheral blood monocyte count can be an independent risk factor for overall and cancer-related survival of patients with CRC metastasis after hepatic resection. Our results suggest that preoperative circulating monocytes in the blood of patients with CRC take part in tumour progression and can be responsible for reduced patient survival. Moreover, we also showed that the peripheral absolute monocyte count in postoperative blood samples had a reverse tendency for survival time. Additional work on the evaluation of monocyte count in postoperative blood samples in a larger group is needed to better understand the observed correlation.
Monocytes are able to interact with adaptive immunity by directing the recruitment and function of lymphocytes within the tumour microenvironment. Circulating monocytes take part in paracrine signalling and produce higher levels of many inflammatory cytokines and chemokines, including tumour necrosis factor alfa, interleukin 1 (IL-1η), interleukin 6 (IL-6), and chemokine ligand 3[27]. They can be recruited into tumours and determine the reduction of cytotoxic CD8+T cell infiltration. Literature data have shown that the inhibition of CCR2-dependent monocyte-derived cells leads to intensive infiltration of CD8+T cells and a reduction in tumour growth in various tumours, including malignant melanoma, pancreatic and liver tumours[28,29]. Monocyte-derived cells can also secrete chemokine ligand 5 (CCL5) that recruits immune suppressive regulatory T cells into the tumour micro-environment[30]. In addition, nonclassical monocytes are important for the recruitment of natural killer (NK) cells to metastatic sites of malignant tumours[31]. Monocytes can overexpress chemoattractants for NK cells, including chemokine ligand 3, CCL4, and CCL5, and may be able to attract NK cells to lung metastases[32]. The close relation between monocytes and lymphocytes prompted us to determine a simple, haematologic MLR. Literature data have demonstrated that the MLR is an independent prognostic factor for patients with advanced gastric cancer and hepatocellular carcinoma undergoing neoadjuvant treatment[33,34]. Most of the research was focused on the preoperative MLR. The significant role of the MLR as a prognostic factor has been confirmed in various malignant neoplasms, including lung cancer, urothelial carcinoma, ovarian carcinoma and gastrointestinal stromal tumours[35-37]. In the present study, CRC patients with a low MLR in peripheral blood obtained after surgery had longer 5-year DFS. Moreover, the multivariate Cox regression model showed that the MLR in peripheral blood obtained after surgery is an independent prognostic factor for 5-year DFS. Our results are in accordance with those of Huanget al[38]who found that CRC patients with a high MLR had a poor prognosis. More studies are required to determine the significance of the MLR in CRC patients.
Table 3 Prognostic factors of 3-yr disease-free survival in patients with colorectal cancer
Moreover, we also examined the neutrophil to lymphocyte and platelet to lymphocyte ratios in pre- and postoperative blood samples from CRC patients. In the current study, the NLR-PLR status in postoperative peripheral blood was found to correlate with histological type and percentage of the mucinous component. The preoperative NLR-PLR status has been reported to be a useful prognostic factor in patients with various gastrointestinal malignancies[39-41]. Recio-Boileset al[39]showed that NLR-PLR status in perioperative blood samples from patients with resectablepancreatic ductal adenocarcinoma was associated with invasion of the resected margins and lymph nodes. The NLR-PLR score was higher in patients with progressive advanced gastric cancer[40]. Moreover, Kabiret al[41]confirmed that the elevated NLR-PLR value in preoperative blood samples from hepatocellular carcinoma patients predicts both overall survival and recurrence-free survival. In multivariate analysis, we failed to confirm these relationships in patients with CRC. We only found a tendency for shorter 3- and 5-year DFS in postoperative samples. Our observation was in contrast to Liet al[42]who demonstrated an inverse correlation between NLR-PLR status and survival time.

Table 4 Prognostic factors of 5-yr disease-free survival in patients with colorectal cancer
Patients with CRC may suffer from thrombocythemia and have a poor prognosis[43]. It is well known that platelets are closely related to cancer cells. Cancer cells can modify platelet behaviour which includes tumour-platelet aggregates, triggering platelet granules and extracellular vesicle release and altering platelet phenotype. Platelets can secrete angiogenic factors and enhance tumour growth by promoting proliferation and antiapoptotic signals. Moreover, they promote tumour invasion and sustain metastasis. Furthermore, platelets assist tumours in evading immune destruction[44]. Therefore, they appear to be important in the immune response against cancer in correlation with neutrophils and lymphocytes. We analysed the platelet count and NLR in pre- and postoperative peripheral blood samples from CRC patients. The present study showed that high PLT-NLR status was found to positively correlate with tumour size in preoperative samples and with histological type and the percentage of mucinous component in samples obtained after surgery. Moreover, the analysis showed that patients with high PLT-NLR status had a longer 3-year and 5-year DFS. Our observations suggest that the PLT-NLR status may be a useful haematologic marker of CRC. To our knowledge, this is the first research on PLT-NLR status in CRC and should be expanded in a larger group of CRC patients in the near future.

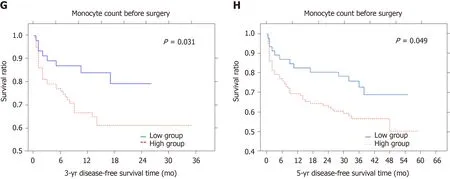
Figure 1 Three- and five-year disease-free survival rates according to monocyte count and monocyte to lymphocyte ratio in colorectal cancer patients, before and after surgery, respectively. Kaplan-Meier curves were used to identify factors for colorectal cancer survival. A and B: Monocyte count before surgery [3- and 5-yr disease-free survival (DFS)]; C and D: Monocyte count after surgery (3- and 5-yr DFS); E and F: Monocyte to lymphocyte ratio before surgery (3- and 5-yr DFS); G and H: Monocyte to lymphocyte ratio after surgery (3- and 5-yr DFS).
In conclusion, the postoperative MLR in whole blood samples can be used as an independent prognostic factor in patients diagnosed with CRC undergoing surgery. In addition, invasion of the lymph node pouch, the number of lymph nodes removed and inflammatory cell infiltration in the invasive front can be considered directly related to DFS in patients with CRC.
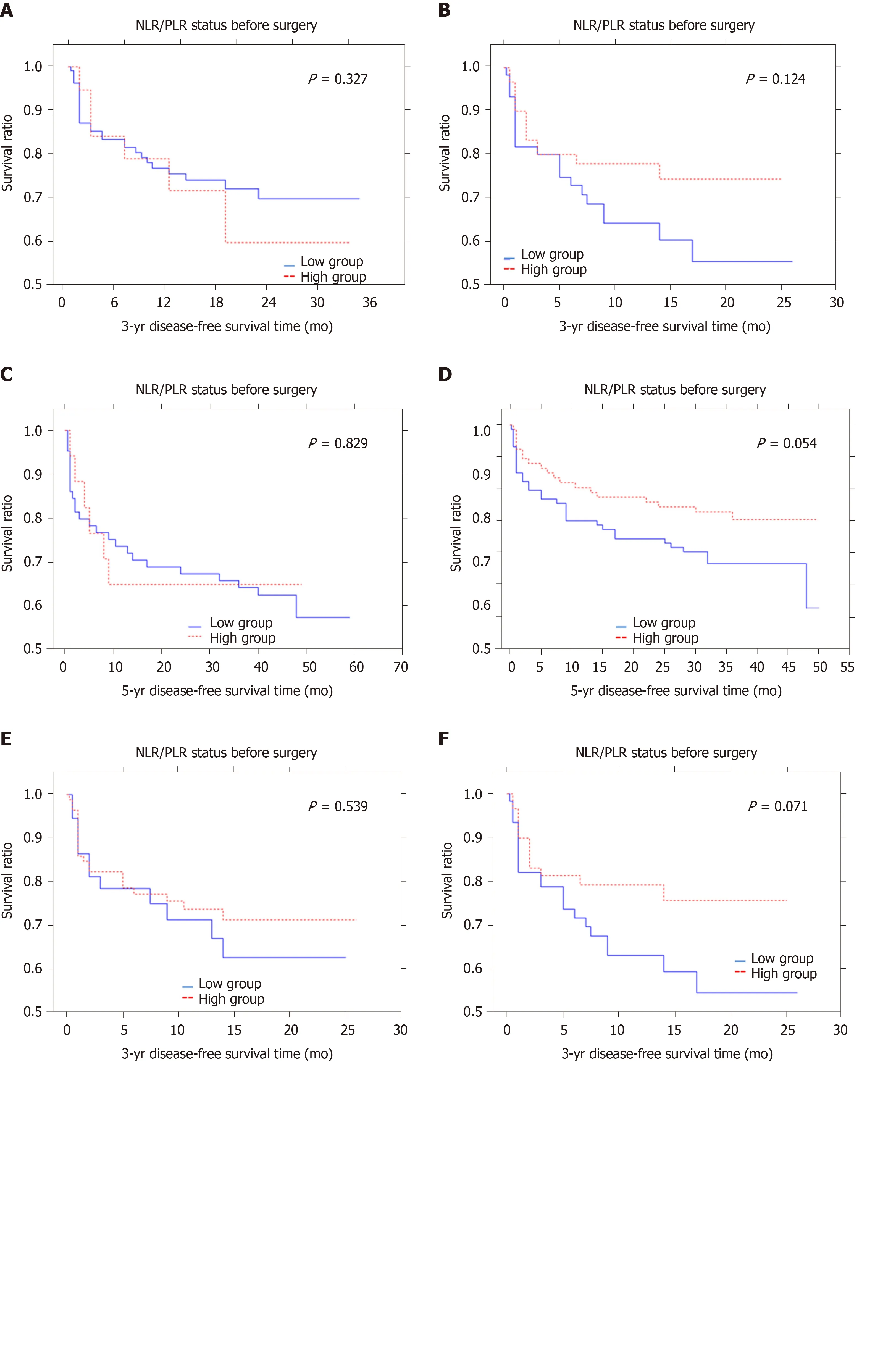
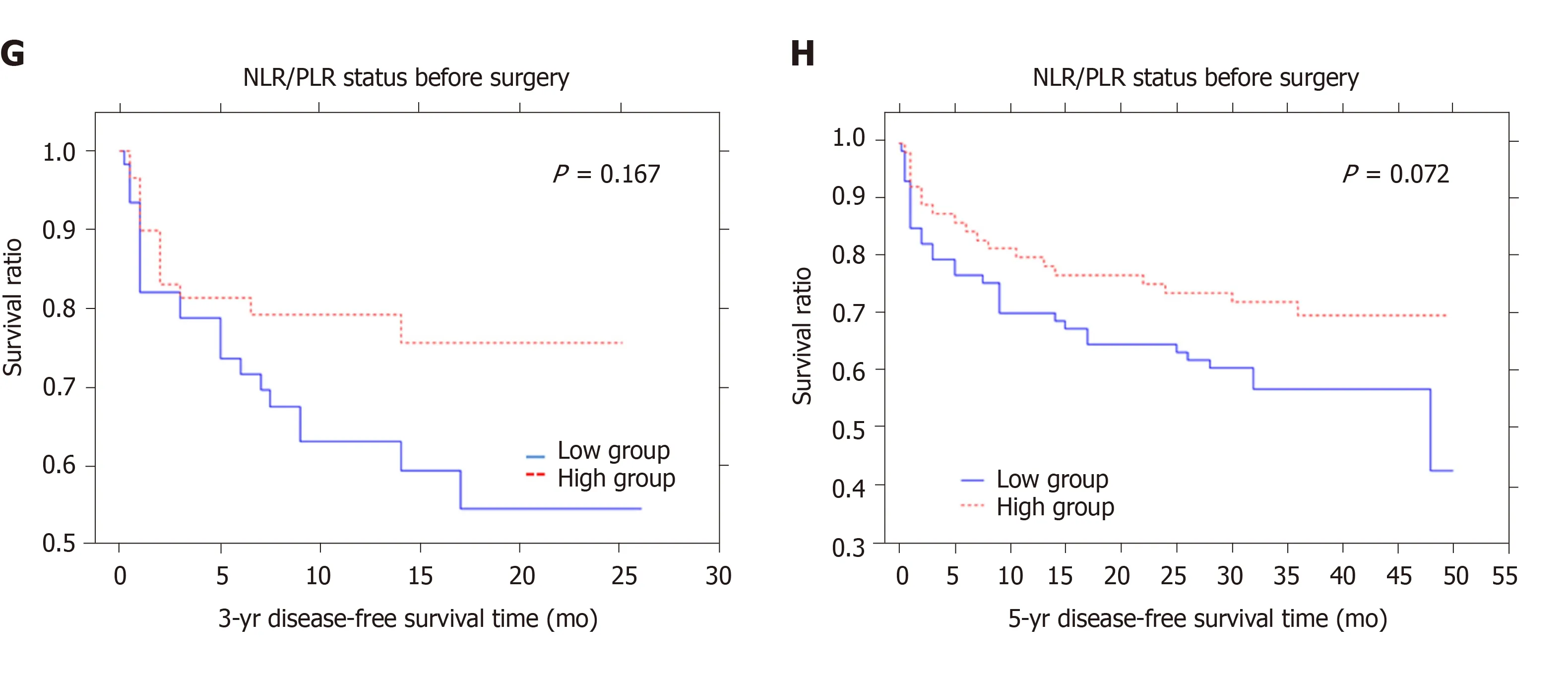
Figure 2 Three- and five-year disease-free survival rates according to neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio status and platelet and neutrophil-to-lymphocyte ratio status in colorectal cancer patients, before and after surgery, respectively. Kaplan-Meier curves were used to identify factors for colorectal cancer survival. A and B: Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio status before surgery [3- and 5-yr disease-free survival (DFS)]; C and D: Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio status after surgery (3- and 5-yr DFS); E and F: Platelet and neutrophil-to-lymphocyte ratio status before surgery (3- and 5-yr DFS); G and H: Platelet and neutrophil-to-lymphocyte ratio status after surgery (3- and 5-year DFS).
ARTICLE HIGHLIGHTS
Research background
Colorectal cancer (CRC) is the third most common malignancy worldwide. Therefore, it is critically important to identify new useful markers that can be easily obtained in routine practice. Recent studies showed that inflammation is a crucial issue in the pathogenesis and development of cancer, especially in tumour progression. However, little is known about the prognostic value of the absolute monocyte count, monocyte to lymphocyte ratio (MLR), the combination of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio (NLR-PLR), and combined platelet and neutrophil-tolymphocyte ratio (PLT-NLR) in patients diagnosed with CRC.
Research motivation
Effective research on haematologic markers that can improve the diagnosis of colorectal cancer and establish patient prognosis.
Research objectives
The aim of the study was to evaluate the prognostic value of absolute monocyte count, MLR, the combination of NLR-PLR, and PLT-NLR in peripheral blood samples of patients with colorectal cancer undergoing surgery.
Research methods
We respectively enrolled CRC patients who undergone surgery between April 2014 and December 2016 in the Department of Oncological Surgery, Comprehensive Cancer Centre (Bialystok, Poland). The status of absolute monocyte count, MLR, NLR-PLR and PLT-NLR was calculated on the basis of blood samples obtained before and after surgery and were examined in correlation with various pathomorphological and clinical factors. Receiver operating characteristic curve analysis was used to investigate cut-off values for the pre- and postoperative haematologic factors examined. The Kaplan-Meier method and the long-rank test were used to compare survival curves. To determine independent prognostic factors, univariate and multivariate Cox proportional hazards regression models were applied.
Research results
The analysis showed that PLT-NLR status was correlated with tumour size and the presence of perineural invasion (P= 0.015;P= -0.174,P= 0.037). Moreover, high NLRPLR and PLR-NLR in the blood samples obtained after surgery were positively
associated with the histological type of cancer and percentage of the mucinous component (NLR-PLR:P= 0.002;P= 0.009; PLR-NLR status:P= 0.002;P= 0.007). The analysis of 5-year disease-free survival showed that the MLR in whole blood obtained after surgery (HR = 2.903, 95%CI: 1.368-6.158,P= 0.005) and the status of lymph node metastasis (HR = 0.813, 95%CI: 0.653-1.013,P= 0.050) were independent prognostic factors in colorectal cancer patients.
Research conclusions
The present study demonstrated that the postoperative MLR in whole blood samples can be used as an independent prognostic factor in patients diagnosed with colorectal cancer.
杂志排行

World Journal of Gastroenterology的其它文章
- Current understanding of the metabolism of micronutrients in chronic alcoholic liver disease
- Establishment of a pattern recognition metabolomics model for the diagnosis of hepatocellular carcinoma
- Clinical and prognostic significance of CC chemokine receptor type 8 protein expression in gastrointestinal stromal tumors
- Initial experience of single-incision plus one port left-side approach totally laparoscopic distal gastrectomy with uncut Roux-en-Y reconstruction
- Feasibility and efficacy evaluation of metallic biliary stents eluting gemcitabine and cisplatin for extrahepatic cholangiocarcinoma
- Impact of interval between neoadjuvant chemoradiotherapy and surgery in rectal cancer patients