Current understanding of the metabolism of micronutrients in chronic alcoholic liver disease
2020-09-23JingWuQingHuaMeng
Jing Wu, Qing-Hua Meng
Abstract Alcoholic liver disease (ALD) remains an important health problem worldwide. Perturbation of micronutrients has been broadly reported to be a common characteristic in patients with ALD, given the fact that micronutrients often act as composition or coenzymes of many biochemical enzymes responsible for the inflammatory response, oxidative stress, and cell proliferation. Mapping the metabolic pattern and the function of these micronutrients is a prerequisite before targeted intervention can be delivered in clinical practice. Recent years have registered a significant improvement in our understanding of the role of micronutrients on the pathogenesis and progression of ALD. However, how and to what extent these micronutrients are involved in the pathophysiology of ALD remains largely unknown. In the current study, we provide a review of recent studies that investigated the imbalance of micronutrients in patients with ALD with a focus on zinc, iron, copper, magnesium, selenium, vitamin D and vitamin E, and determine how disturbances in micronutrients relates to the pathophysiology of ALD. Overall, zinc, selenium, vitamin D, and vitamin E uniformly exhibited a deficiency, and iron demonstrated an elevated trend. While for copper, both an elevation and deficiency were observed from existing literature. More importantly, we also highlight several challenges in terms of low sample size, study design discrepancies, sample heterogeneity across studies, and the use of machine learning approaches.
Key words: Alcoholic liver disease; Metabolism; Trace elements; Vitamins; Malnutrition; Oxidative stress
INTRODUCTION
Hepatitis B virus infection remains a major cause of chronic liver disease due to its high prevalence and high susceptibility to progress to cirrhosis. With the intensive implementation of hepatitis B vaccination and treatment programs, the epidemiology of liver disease is undergoing major changes in the Asia–Pacific region. Converging evidence has suggested the dramatic benefits of moderate alcohol consumption in cardio-protection, which is the so-called “J” shaped curve in the relationship between alcohol consumption and overall mortality[1]. However, the threshold of consumption is difficult to define. Heavy alcohol consumption may eventually result in a broad spectrum of liver damage ranging from liver steatosis, alcoholic hepatitis, liver cirrhosis, and finally to hepatocellular carcinoma[2]. The incidence of alcoholic liver disease (ALD) is increasing, and requires more attention[3]. Globally, excessive alcohol consumption accounts for nearly half of the burden of liver disease[4]. Notably, the estimated number of deaths from diseases caused by alcoholism was about 3.3 million in 2012 globally, accounting for 7.6% of all deaths among males and 4.0% among females[5]. From the year 2005 to 2015, alcoholism was responsible for 9.8% and 22.1% of the global incidence of liver cirrhosis and liver cancer respectively[6].
For patients with severe liver damage, there are frequent complications including malnutrition, ascites, spontaneous bacterial peritonitis, encephalopathy, and esophageal varices. Specifically, protein-energy malnutrition, which is associated with poor prognosis, is uniformly recognized in almost all patients with alcoholic hepatitis and ALD, which further increases liver vulnerability to alcohol toxicity[7]. For these patients, nutritional support is essential to prevent further progression. Current guidelines from the European Society for Clinical Nutrition and Metabolism and the American Association for the Study of Liver Disease recommend a daily energy intake of 35-40 kcal/kg and protein intake of 1.2-1.5 g/kg through night time snacks and morning feeding for patients with ALD[5]. However, it is really difficult to achieve this objective in practice, since alcohol ingestion usually constitutes half of the daily energy intake in these patients, resulting in a deficiency of energy converted from daily food.
Apart from protein-energy deficiency, metabolic disturbances of micronutrients including vitamins and mineral elements malnutrition are quite common in patients with ALD, as liver dysfunction may affect the metabolism of these elements. ALD patients usually exhibit a clinical spectrum of manifestations including poor-quality diet, polyuria, diarrhea, and vomiting, which to some extent carry an elevated risk of nutrient loss. In addition, portal hypertension in patients with cirrhosis exerts adverse effects on nutrition absorption, another synergistic contributor resulting in fluctuations in the concentration of micronutrients. Accordingly, screening for micronutrientdeficiency and giving adequate supplementation are also recommended by the American Association for the Study of Liver Disease guidelines[8]. However, a definite amount of daily micronutrient intake is not provided. Thus, in contrast to proteinenergy malnutrition, perturbations of micronutrients in ALD patients have attracted less attention. Oxidative stress is one of the most important contributors facilitating pathogenesis and progression of ALD[9]. Trace elements are cofactors or structural constituents of key antioxidant enzymes and other crucial metabolic enzymes for the maintenance of homeostasis. Consequently, a deficiency of these trace elements would lead to disturbances in antioxidant systems, which have long been recognized in ALD[10]. In addition, the abnormal accumulation of elements such as iron in the liver and/or other organs can also trigger malfunction of the corresponding organ.
Recent years have witnessed a significant improvement in our understanding of the role of micronutrients in the pathogenesis and progression of ALD. However, the highly complex nature of ALD poses an immense challenge for understanding the precise biological mechanisms. The goal of this review is to summarize the findings on the imbalance of micronutrients in patients with ALD with a focus on zinc, iron, copper, magnesium, selenium, vitamin D, and vitamin E, and determine their potential mechanisms (Table 1). Moreover, we also highlight some challenges emerging from existing studies that aim to assess how disturbances in micronutrients relate to the pathophysiology of ALD, as well as present some promising future directions.
MINERAL MALNUTRITION IN ALD
Zinc deficiency
The investigation of mineral malnutrition in ALD has been most active in Zinc (Zn). As an essential metallic element, Zn plays a pivotal role in multiple biological processes including the regulation of neurotransmitter functions, intracellular signaling transduction, inflammatory response, reactive oxygen species (ROS) production, immunoregulation, wound healing, as well as gene expression[11-15]. Independent lines of research suggest that approximately 10% of the human proteome, which includes a total of 2800 proteins, may bind with Zn and cellular Zn fluctuations may dramatically disturb the biological functions of these Zn-binding proteins[16]. Convergent findings suggested that there was a significant Zn deficiency in patients with ALD[17]. Dietary Zn supplementation could provide protection against metabolic dysfunction and alcoholic liver injury[18-21]. Apart from the common factors (e.g., poorquality diet, polyuria, diarrhea), that can result in Zn deficiency, the Zn deficiencyinduced anorexia or acrodermatitis enteropathica might, in turn, exacerbate the deficiency[22,23]. Zn may protect against ethanol-induced liver injury by participating in multiple pathways. A mouse model suggested that Zn could decrease tight-junction proteins and further increase the risk of intestinal barrier dysfunction, thereby resulting in endotoxemia and liver injury[15]. Another study observed that a reduction in the Zn level was linked with mitochondrial dysfunction and oxidative liver injury through ROS generation and depletion of glutathione. Glutathione is the most important member of the antioxidants in cellular antioxidant defense[10]. Consequently, the hepatoprotective effect of Zn in alcoholic liver injury may be ascribed to its inhibition of oxidative stress[10]. Moreover, some studies found that Zn may be involved in hepatocyte apoptosis. Zinc depletion contributed to the overexpression of Fas ligand and elevation of cytosolic cytochrome, which may further activate caspase-3, a hallmark of cell apoptosis[24]. In terms of immunomodulation, Zn can interfere with the NF-kB pathway, which can influence the production of lipopolysaccharide (LPS)-induced hepatic TNF-α and disturb dendritic cells’ ability to respond to LPS. Growingin vivoexperiments suggest that oral Zn supplementation has therapeutic potential in the prevention and/or treatment of ALD[10,25].
Iron overload
Iron is critical in many fundamental biological processes as it participates in hemoglobin and myoglobin formation, which control the transportation of oxygen, as well as deoxyribonucleic acid biosynthesis and ATP synthesis[26]. In addition, iron is a cofactor of multiple enzymes that regulate the tricarboxylic acid cycle and the electron transport chain[27,28]. Iron metabolic disorder may induce irreversible damage to cellular homeostasis. There is a growing consensus that patients with ALD are frequently characterized by serum iron elevation and hepatic iron overload and it was estimated that significant pathological iron deposition could be detected in approximately 50% of ALD patients[29]. Excessive alcohol exposure promotes iron absorption and a subsequent increase in ferritin. Actually, ethanol by itself can directly induce ferritin synthesis and suppress IL-6-mediated hepcidin production[30,31]. The increased iron content and ferritin expression subsequently contribute to disease progression[32,33]. Specifically, it has been widely reported that ferritin could interfere with hepatic stellate cells (HSC) and disturb the balance between extracellular matrix deposition and degradation, which can significantly increase the risk of liver fibrosis[34,35]. On the other hand, there are also studies implying that iron itself could activate HSC and promote the gene expression of type I collagen, which is a clinical indicator of liver fibrosis, providing solid evidence that iron overload could promote the development of liver fibrosis[36].
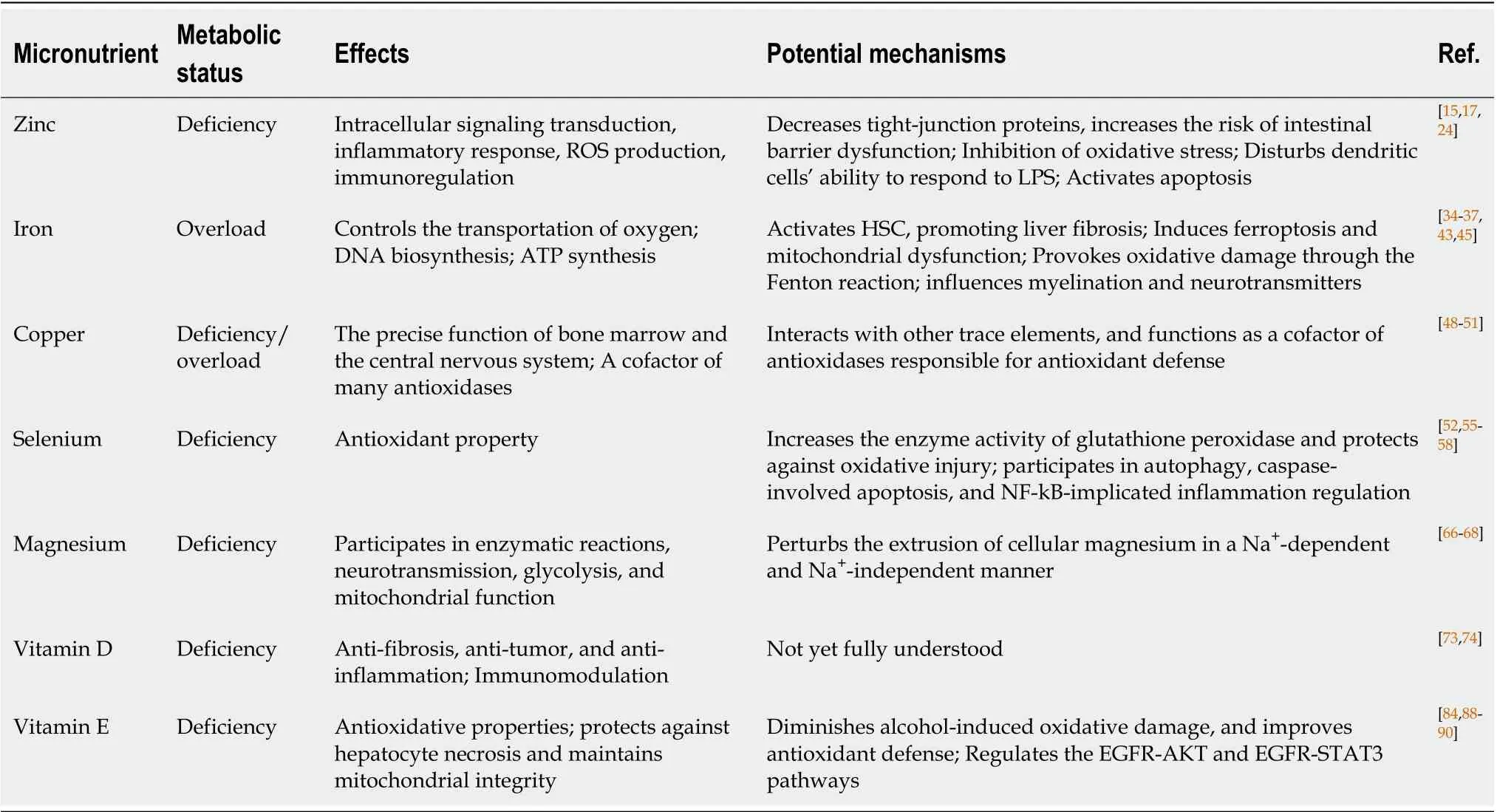
Table 1 Micronutrients imbalance in patients with alcoholic liver disease
Additionally, studies have demonstrated that iron overload could result in ferroptosisviaROS production and lipid peroxidation. Ferroptosis is a form of irondependent oxidative cell death that is morphologically, biochemically, and genetically different from autophagy and apoptosis. In addition, an excessive iron-induced ROS burst could lead to mitochondrial dysfunction, which is a typical characteristic of ferroptosis[37]. Inhibition of ferroptosis can relieve ethanol-induced liver injury[38-40]. Therefore, preventing the abnormal accumulation of iron and even ferroptosis would be a potential candidate for the design of novel therapeutic strategies for patients with ALD.
Accumulating research has unfolded the association between iron and immune function. Excessive iron is associated with the likelihood of activating the transcription factor NF-kB and upregulating the expression of pro-inflammatory cytokines. In addition, considering the close relationship between iron and bacterial multiplication as well as virulence, iron overload could behave as a deleterious factor of infections[41,42]. Apart from the above-mentioned mechanisms, iron-induced oxidative stress is another extensively investigated biological process. During oxidative stress, iron can produce oxygen free radicalsviathe Fenton reaction. Then, oxygen free radicals receive electrons transferred from lipids, resulting in decomposition of the cytoplasmic membrane, and damage to intracellular organelles, a process known as lipid peroxidation. Moreover, as demonstrated in some investigations, oxidative stress could also trigger collagen expression in HSC, and further contribute to the development of liver fibrosis[43].
Some recent studies have also established the relationship between iron overload and cognitive or behavioral deficits in patients with ALD. Generally, these patients demonstrated greatly overlapped behavioral, cognitive, physiological, and social problems[44]. Putatively, studies suggested that iron brought about these phenotypic dysfunctions by exerting influences on the brain systems. Specifically, iron can influence myelination as well as the synthesis and metabolism of neurotransmitters[45]. Moreover, chronic excessive alcohol induced-abnormal iron deposition in brain areas including the basal ganglia and dentate nucleus may act as a contributor to this phenomenon[46].
Copper imbalance
Copper is an extracellular element responsible for the precise function of bone marrow and the central nervous system, and it also functions as a cofactor of many antioxidases[47]. Consequently, copper metabolic disorder may induce dysfunction in the corresponding organ. Compared with the two trace elements (i.e., iron and Zn) mentioned above, investigations focusing on revealing the relationship between copper metabolism and the potential pathophysiology of ALD are relatively limited. Findings derived from these studies were also far from conclusive and sometimes even inconsistent. For example, results from the study by Shibazakiet al[48]showed that people with excessive alcohol consumption tended to exhibit a significant copper deficiency, which concurs with prior evidence showing copper metabolism perturbations in patients with ALD[48]. In contrast, another study found that copper levels in patients with ALD were elevated or unchanged as compared with healthy controls[49]. Unfortunately, most of these available studies only reported the differences in copper levels between patients and healthy controls from the perspective of statistical analysis, with the mechanistic insights into the involvement of copper imbalance in the pathogenesis of ALD significantly unexplored. This may be partially ascribed to the fact that copper has a complex interaction with other trace elements, especially iron and Zn. Specifically, hyperzincemia can suppress copper absorption, and copper deficiency usually has a synergistic effect with Zn reduction in impairing normal functioning of the central nervous system in patients addicted to alcohol[50]. In addition, copper deficiency can dampen iron transport by suppressing the activity of hephaestin, a copper-containing ferroxidase necessary for iron efflux from enterocytes[51]. These three metals function as cofactors of antioxidases that are responsible for antioxidant defense, which is critical in preventing oxidative damage in patients with ALD. Taken together, further investigations to elucidate the specific metabolic pattern of copper in patients with ALD are warranted.
Serum selenium deficiency
Selenium is an important component of antioxidant-glutathione peroxidase and thus it has been broadly used in the clinic due to its antioxidant property. Abnormal metabolism of selenium has been reported in a growing body of research, which suggested that low selenium level is a common feature of patients with ALD[52]. Selenium metabolic disorder may lead to liver dysfunction[52,53]. However, the involvement of selenium depletion in the pathogenesis of ALD has not been fully defined. Substantial efforts have hitherto been devoted to revealing the potential mechanisms. For example, a study suggested that selenium was capable of alleviating liver histopathological features including hepatocyte injury, abnormal accumulation of liver fat and liver neutrophils infiltration, and can reduce elevated ALT levels after selenium supplementation inin vivoexperiments[54]. Putatively, the protective effects of selenium predominantly may lie in its ability to increase the level or the enzyme activity of glutathione peroxidase and thus affords marked protection against oxidative injury. Other studies have implied that the participation of selenium in autophagy, caspase-involved apoptosis, and NF-kB-implicated inflammation regulation may be another protective mechanism[55-57]. Despite the above findings, some investigations derived inconsistent results suggesting that chronic excessive alcohol intake might have no significant effect on serum selenium levels[58], even though it may not be that common. Therefore, further investigation is still urgently required to determine the metabolism of selenium in patients with ALD.
Hypomagnesemia
Magnesium is the second most abundant intracellular cation after potassium, and mitochondria, endoplasmic reticulum, and cytosol constitute the top three cellular pools that are rich in Mg2+[59]. Consequently, serum magnesium levels may not reflect the real storage. Magnesium participates in diverse biological processes, including enzymatic reactions, neurotransmission, glycolysis, and mitochondrial function[60,61]. Growing evidence suggests that magnesium metabolic disorder is common in patients with severe malnutrition, diabetes, hypertension, and ALD[62,63]. Importantly, hypomagnesemia is also a significant electrolyte abnormality in critically ill patients, and these patients have higher mortality than patients with normomagnesemia[64]. With regard to excessive alcohol exposed populations, convergent findings suggest that magnesium deficiency is a common feature[65]. It was reported that alcohol could decrease whole tissue magnesium by approximately 14%, of which liver magnesium accounted for 5%-10%. In addition, hepatocytes from ethanol-treated rats exhibited a 25% reduction in cellular magnesium compared with the control group[66]. Alcohol may induce magnesium disturbance by perturbing the extrusion of cellular magnesium in a Na+-dependent and Na+-independent manner. In addition, there was also a distinct decline in ATP content. All these pieces of evidence indicate that chronic alcohol consumption could considerably impair Mg2+homeostasis and transport of liver cells after prolonged exposure to alcohol. The inability of liver cells to reserve Mg2+might, at least in part, explain the reduction in tissue Mg2+content after prolonged exposure to alcohol. In particular, alcohol treated-cells became insensitive to catecholamine-induced magnesium accumulation, which to some extent prevented hepatocytes from restoring cellular magnesium[66,67].
VITAMIN METABOLISM IN ALD
Vitamin D deficiency
Existing work in liver diseases concerning vitamin metabolism has mostly focused on vitamin D. In past years, vitamin D has been well documented due to its classical effects on bones and calcium metabolic homeostasis. Results from recent functional and mechanical studies demonstrate that vitamin D could also behave as a regulatory factor modulating many other biological functions such as cell proliferation, apoptosis, cell cycle, differentiation, and immunomodulation. Additionally, the effects of vitamin D in anti-fibrosis, anti-tumor, and anti-inflammation have also been systematically investigated.
It was estimated that approximately one billion people worldwide are vitamin D insufficient[68]. Accumulating research has indicated that people with a lower concentration of vitamin D always have a higher body mass index and are predisposed to being diagnosed with hypertension and many cancer types[69,70]. Decreased vitamin D concentration is one of the most consistent observations in patients with chronic disease, especially those with severe liver disease. An enormous number of studies have indicated that vitamin D could modulate the biological function of HSC, which can effectively attenuate liver fibrosis. Specifically, Potteret al[71]observed that the vitamin D receptor could combine with a proximal Sp1.1 site and a newly identified distal site on the collagen promoter, through which vitamin D could suppress TGFβ1-induced type I collagen formation in HSC[71].
It was estimated that 96% of alcoholic patients have repressed levels of serum vitamin D, and 86.1% were deficient and 60.4% were severely deficient. In addition, among alcoholic patients, a severe deficiency of vitamin D was quite common in those with alcoholic steatohepatitis[72]. This concurs with prior evidence that decreased serum vitamin D was associated with increased susceptibility to ethanol-induced liver damage, which was manifested by abnormal serum AST, steatosis, and liver cirrhosis. Typically, Trépoet al[73]reported that severe vitamin D deficiency was significantly associated with a poor prognosis and complications of portal hypertension[73]. This study also found that vitamin D treatment or supplementation could suppress the expression of the pro-inflammatory cytokine TNFα, which further confirmed the role of vitamin D in immunomodulation. Moreover, the results of a prospective study among patients with alcoholic liver cirrhosis found that oral vitamin D supplementation decreased the Child-Pugh score and ameliorated liver damage[74]. Collectively, these data highlight the possibility that vitamin D may serve as a diagnostic biomarker and a potent agent in the management of ALD. However, the specific role of vitamin D in the pathogenesis, disease progression, and other complications during the course of ALD is not yet fully understood. Therefore, there is a pressing need for further studies to elucidate the precise mechanisms underlying vitamin D and alcohol-induced hepatotoxicity, which can facilitate clinical applications and improve the diagnosis, prevention, and treatment of ALD.
Vitamin E inadequacy
As a nonenzymatic antioxidant, vitamin E has been intensively investigated due to its antioxidative properties. Dietary sources of vitamin E predominately include vegetables, nuts, olive oil, and lean meats. The endogenous metabolites of vitamin E consist of multiple isomers, among which α-tocopherol is the most important biological active form[75]. Through suppression of oxidative and inflammatory reactions, vitamin E alleviated the progression of atherosclerosis in low-density lipoprotein receptor-deficient mice fed with a high-fat diet[76]. Moreover, vitamin E has beneficial effects on the prevention of cancers and diabetes due to its antioxidative effects[77]. Chronic vitamin E deficiency could increase the risk of damage in response to oxidative stress. A recent study observed that a moderate intake of vitamin E changed the composition of gut microbiota and altered intestinal microbiota involved in the pathogenesis of ALD[78]. In a clinical trial of patients with nonalcoholic steatohepatitis and advanced fibrosis, Vilar-Gomezet al[79]found that vitamin E supplementation improved patients’ clinical outcomes including reducing the risk of death or liver transplant and the probability of hepatic decompensation[79]. Moreover, for other chronic liver diseases such as steatocholestasis and drug-induced liver injury, vitamin E also protected against hepatocyte necrosis and maintained mitochondrial integrity[80,81]. Notably, apart from the effects of anti-inflammation and antioxidative properties, some studies have also highlighted that vitamin E is involved in signal transduction and gene expression. Specifically, it is postulated that vitamin E achieves its anti-inflammation, anti-tumor, and anti-apoptosis effects partly by regulating the expression of related genes (e.g., P53, NF-kB, cyclin D1)[82].
It is widely accepted that vitamin E deficiency is common in patients with ALD[83]. Malnutrition, along with impaired transport by lipoproteins may be the primary causes of vitamin E deficiency[84]. Clinical administration of vitamin E increased the plasma α-tocopherol but did not improve the parameters of liver function and clinical outcomes such as motility and one-year survival. However, vitamin E decreased the expression of hyaluronic acid, an indicator correlated with hepatic fibrosis[85,86]. Studies in an animal model showed that vitamin E could diminish alcohol-induced oxidative damage by removing ROS, reducing lipid peroxidation, and improving antioxidant defense[87], which is in harmony with findings from the study by Yaoet al[88]. Treatment with vitamin E, especially together with tannic acid, relieved histologic damage, reduced collagen, and glycogen deposition in addition to its hepatoprotective role in decreasing the levels of serum hepatic damage markers (e.g., ALT, AST). The hepatoprotective effects may be the result of vitamin E’s antioxidative property and its suppression of the inflammatory response as well as cell apoptosis through regulation of the EGFR-AKT and EGFR-STAT3 pathways[89].
CHALLENGES AND FUTURE DIRECTIONS
The studies surveyed above open interesting cues to systematically explore the benefits of micronutrients-based therapeutic interventions in the cure of alcoholinduced liver injury. However, some important issues should be discussed. Here, we elaborate on some representative challenges that have emerged from the reviewed studies, and present some promising future directions as follows:
Sample size
Most of the studies discussed in this review included a limited number of subjects. Although small studies have multiple practical advantages, such as being timesaving in the enrollment of subjects, and high flexibility in data analyses[90], results from these small samples are usually attached to low statistical power[78], and are more likely to generate false-positive results. In this regard, these biomedical findings may only demonstrate statistically significant effects but have no clinical utility. Consequently, future investigators should perform analyses following larger studies involving more subjects.
Study design
There is a pyramid of evidence, which represents a general hierarchy of multiple clinical study designs. The top of the pyramid is the double-blind, randomized, controlled studies, and such investigations without the use of surrogate endpoints are always most rigorous and reliable to evaluate the effects of a specific intervention[91]. However, many of the clinical studies discussed in the current review enrolled patients with liver diseases from a single clinic and were carried out in a nonrandomized manner. In contrast to the randomized controlled trials, the nonrandomized controlled investigations cannot invariably eliminate bias in the studies efficiently, which may silently affect the results and fool the investigators[92]. As such, the results may be confusing and misleading. Additionally, some of the important studies were conducted in mice that are innately different from humans. Animal research is at the base of the pyramid with the lowest forms of evidence, thereby limiting its wider application in clinical settings. For example, although various independent animal studies reported that vitamin E administration alleviated liver damage, supplementation of vitamin E to ALD patients had no significant influence on clinical status[86]. Therefore, we encourage future studies assessing the impact of micronutrients on ALD to be designed as randomized controlled trials.
Sample heterogeneity across studies
To minimize the imbalance of sample properties between two groups being compared, it is necessary to ensure that the two populations are propensity matched on the irrelevant variables (e.g., age, gender, body mass index) except the one of interest. However, we cannot guard against the possibility that there are some unrecognized confounders that may contribute to the imbalance between groups, and further affect the results[79]. This may also be one of the reasons that inconsistent results were sometimes derived from existing studies, especially when group comparisons were conducted in small samples.
On the other hand, there is also heterogeneity in the variable of interest per se between studies. To explore the effect of a specific micronutrient, various treatment doses for various durations were administered across reported studies, as there is no definite “golden standard” for them, especially for exploratory studies at an earlystage. Despite the fact that the confounding variables have been largely balanced, the findings might also be inconsistent across different trials. A case in point was whether vitamin E replacement benefits ALD patients. A clinical study by de la Mazaet al[86]observed that supplementation with 500 IU vitamin E for one year had no significant effect on hepatic laboratory parameters and mortality[86]. However, Mezeyet al[85]found that vitamin E could decrease serum hyaluronic acid, a biomarker of liver fibrosis, when ALD patients were given 1000 IU vitamin E for three months[85]. These findings, to some extent, might fail to help investigators to reach a firm decision in clinical practice. Of note, excessive drug (which was intended to serve as a therapy) exposure has a detrimental effect, which might also mislead researchers. For example, a metaanalysis by Milleret al[93]discovered that high-dosage vitamin E (≥ 400 IU/d) showed an increased risk of all-cause mortality[93]. Therefore, many efforts are required to extensively control potential confounders.
Machine learning methods
Among the reviewed studies, univariate analytical techniques were the most widely applied methods in the investigation of micronutrient imbalance in alcoholic-induced liver diseases. Such investigations maintain a focus on group-level comparison to examine whether significant group differences exist in a specific micronutrient between patients with liver disease and healthy controls. Although these studies have advanced our understanding of the mechanisms underlying ALD, the biggest disadvantage of them is that they do not have the ability to provide individualized guidelines. In recent years, machine learning-based methods have attracted substantial attention from multiple research fields, which can build a multivariate predictive model by employing cross-validation strategies to ensure generalization[94]. However, the application of machine learning models in the investigation of micronutrients in ALD is relatively limited. Futures studies can capitalize on the strengths of machine learning to better reveal the role of micronutrients in the pathology of ALD.
CONCLUSION
In this review, we summarized studies investigating micronutrients imbalance in patients with ALD, with a focus on zinc, iron, copper, selenium, magnesium, vitamin D and vitamin E. Overall, zinc, selenium, vitamin D and vitamin E uniformly exhibited a deficiency, and iron demonstrated an elevated trend. While, for copper, both an elevation and deficiency were observed from existing studies, which requires further investigation. In conclusion, this review helps delineate the imbalance of micronutrients in ALD, thus shedding light on the underlying mechanism, and offering possibilities for clinical intervention.
杂志排行

World Journal of Gastroenterology的其它文章
- Establishment of a pattern recognition metabolomics model for the diagnosis of hepatocellular carcinoma
- Monocyte-to-lymphocyte ratio as a prognostic factor in peripheral whole blood samples of colorectal cancer patients
- Clinical and prognostic significance of CC chemokine receptor type 8 protein expression in gastrointestinal stromal tumors
- Initial experience of single-incision plus one port left-side approach totally laparoscopic distal gastrectomy with uncut Roux-en-Y reconstruction
- Feasibility and efficacy evaluation of metallic biliary stents eluting gemcitabine and cisplatin for extrahepatic cholangiocarcinoma
- Impact of interval between neoadjuvant chemoradiotherapy and surgery in rectal cancer patients