血清疼痛介质及炎症因子在腰椎间盘突出症急性期患者康复治疗前后的变化
2020-06-08林菲菲叶亚云王朋
林菲菲 叶亚云 王朋
[摘要] 目的 探讨血清疼痛介质及炎症因子在腰椎间盘突出症急性期患者康复治疗前后的变化。 方法 选择2017年1月~2018年12月就诊的LDH急性期患者50例作为观察组。观察组患者予以卧床休息、避免腰部剧烈活动、腰椎骨盆牵引、针刺、理疗和推拿等康复措施,连用7 d。观察患者治疗前和治療7 d后血清疼痛介质[多巴胺(DA)、去甲肾上腺素(NE)和5-羟色胺(5-HT)]及炎症因子[白介素-6(IL-6)、IL-8和IL-10]水平变化。另取体检中心健康体检者30例作为对照组。比较两组血清DA、NE、5-HT、IL-6、IL-8和IL-10水平。 结果 观察组患者血清DA、NE和5-HT水平明显高于对照组(P<0.01);治疗7 d后,观察组患者血清DA、NE和5-HT水平较治疗前明显下降(P<0.05)。观察组患者血清IL-6、IL-8水平明显高于对照组,IL-10水平明显低于对照组(P<0.01);治疗7 d后,观察组患者血清IL-6和IL-8水平较治疗前明显下降,IL-10水平较治疗前明显上升(P<0.05)。 结论 LDH急性期存在血清疼痛介质DA、NE和5-HT水平异常升高,其水平的变化可作为LDH急性期治疗疗效随访和预后评估的敏感血清指标;同时LDH急性期存在促炎症/抗炎症因子网络水平紊乱,血清IL-6、IL-8水平的异常升高,血清IL-10水平异常下降,其水平的变化亦可作为LDH急性期疗效随访和预后评估的敏感血清指标。
[关键词] 腰椎间盘突出症;急性期;疼痛介质;炎症因子
[中图分类号] R681.3 [文献标识码] B [文章编号] 1673-9701(2020)10-0152-04
[Abstract] Objective To investigate the changes of serum pain mediators and inflammatory factors before and after rehabilitation treatment in patients with acute lumbar disc herniation. Methods 50 patients with acute LDH from January 2017 to December 2018 were enrolled as observation group. They were given rest in bed, avoiding lumbar violent activities, lumbar pelvic traction, acupuncture, physiotherapy and massage, etc., for 7 days. The changes of serum pain mediators including dopamine(DA), norepinephrine(NE) and serotonin(5-HT), and inflammatory factors including interleukin-6 (IL-6), IL-8 and IL-10 before and at 7 days after treatment in the observation group were observed. Another 30 healthy subjects in the physical examination center were used as the control group. Serum levels of DA, NE, 5-HT, IL-6, IL-8 and IL-10 were compared between two group. Results The levels of serum DA, NE and 5-HT in the observation group were significantly higher than those in the control group(P<0.01). In the observation group, the levels of serum DA, NE and 5-HT after 7 days of treatment were significantly lower than those before treatment(P<0.05). The levels of serum IL-6 and IL-8 in the observation group were significantly higher than those in the control group, and the level of IL-10 in the observation group was significantly lower than that in the control group(P<0.01). After 7 days of treatment, the serum levels of IL-6 and IL-8 in the observation group were higher than those before treatment, and the level of IL-10 decreased significantly compared with that before treatment(P<0.05). Conclusion The levels of serum pain mediators including DA, NE and 5-HT are abnormally elevated in the acute phase of LDH. The changes of serum levels can be used as sensitive serum indicators for the follow-up and prognosis evaluation of acute LDH treatment. Meanwhile, there is pro-inflammatory/anti-inflammatory factor network level disorder, abnormal rise of serum IL-6 and IL-8, and abnormal decrease of serum IL-10 in the acute phase of LDH. The change can also be used as a sensitive serum index for follow-up and prognosis evaluation of acute LDH treatment.
[Key words] Lumbar disc herniation; Acute phase; Pain mediators; Inflammatory factor
腰椎间盘突出症(lumbar disc herniation,LDH)是门诊常见病与多发病,其发病率占椎管疾病的第1位,多见于中老年患者,主要是由于各种原因导致的髓核、纤维环及软骨板发生退行性变,使髓核等椎间盘组织从破裂处脱出或突出刺激或压迫神经根而引起腰腿痛或活动受限[1,2]。LDH的发病机制较复杂,近年来研究发现疼痛介质及炎症因子在其发病中起着极其重要作用[3,4]。卧床休息、腰椎骨盆牵引、针刺或推拿是目前治疗LDH急性期常用的康复锻炼措施,疗效较好,但疼痛介质及炎症因子的在康复治疗前后的变化国内外报道较少[5,6]。本研究观察了血清疼痛介质及炎症因子在腰椎间盘突出症急性期患者康复治疗前后的变化,现报道如下。
1 资料与方法
1.1 一般资料
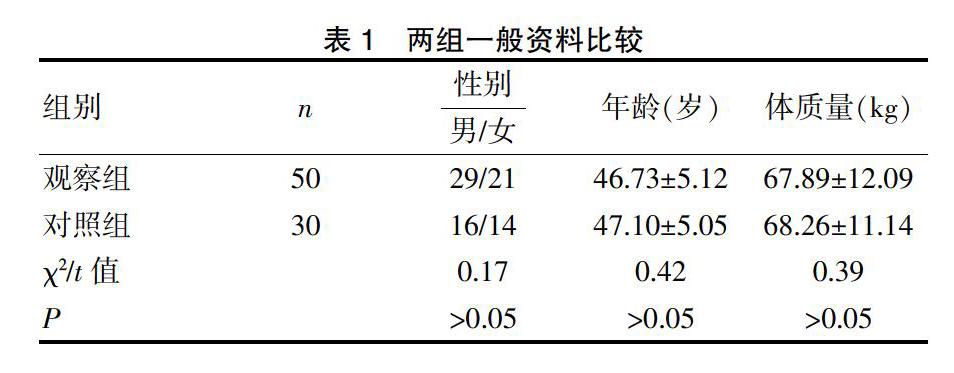
选择2017年1月~2018年12月在我院门诊就诊的LDH急性期患者50例作为观察组。纳入标准[7]:(1)诊断符合《腰椎间盘突出症》中的相关标准[8],并经CT或磁共振检查确诊;(2)1周内急性发作或首次发作未超过1周。排除标准[9]:(1)腰椎狭窄、结核、转移瘤及腰椎失稳症等原因引起腰腿痛者;(2)内分泌、血液或代谢性疾病或严重感染性疾病者。另取我院体检中心健康体检者30例作为对照组。两组性别、年龄及体质量等情况均衡可比(P>0.05)。见表1。
1.2 方法
观察组患者予以卧硬板床休息、避免腰部剧烈活动、腰椎骨盆牵引、针刺或理疗推拿等康复干预措施,连用7 d。观察患者治疗前和治疗7 d后血清疼痛介质[多巴胺(Dopamine,DA)、去甲肾上腺素(Noradrenaline,NE)和5-羟色胺(5 -hydroxytryptamine,5-HT)]及炎症因子[白介素-6(interleukin-6,IL-6)、IL-8和IL-10]水平变化。而对照组仅在入组前测定上述指标1次。
1.3 观察指标
1.3.1 标本采集 采集静脉血3~5 mL置入肝素钠抗凝离心管中,2500 r/mim,4°C离心10 min分离出血清分装,置于-70°C冰箱待检。
1.3.2 血清DA、NE、5-HT、IL-6、IL-8和IL-10水平测定 采用荧光分光光度法测定血清DA、NE和5-HT水平;采用酶联免疫吸附法测定IL-6、IL-8和IL-10水平。
1.4 统计学处理
应用SPSS20.0软件,计量资料用均数±标准差(x±s)表示,采用t检验,计数资料用[n(%)]表示,采用χ2检验,P<0.05为差异有统计学意义。
2 结果
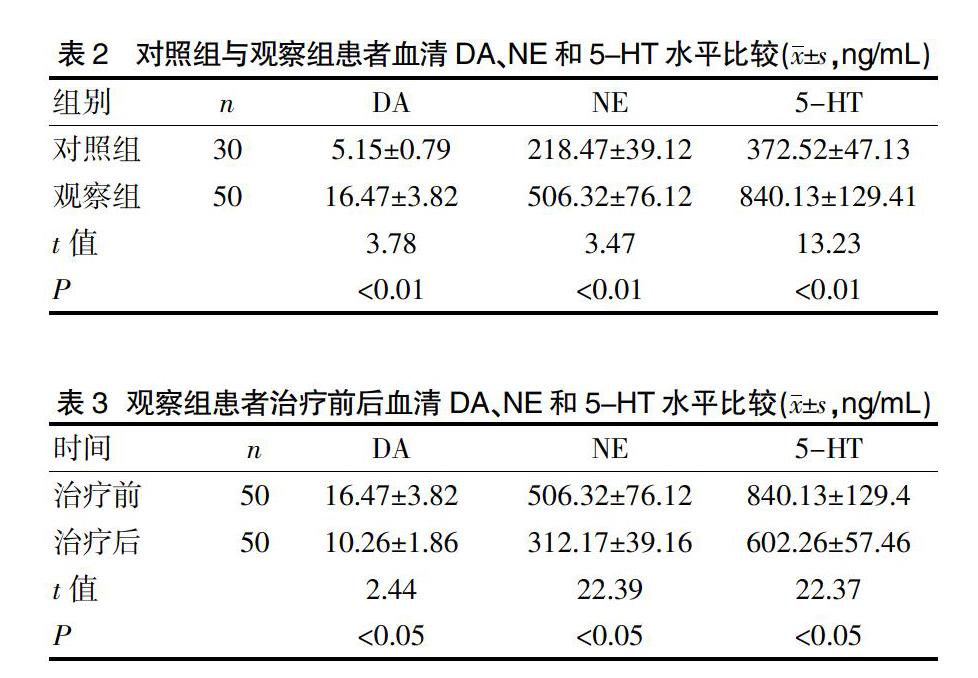
2.1 对照组与观察组以及观察组治疗前后血清DA、NE和5-HT水平比较
观察组患者血清DA、NE和5-HT水平明显高于对照组(P<0.01);治疗7 d后,观察组患者血清DA、NE和5-HT水平较治疗前明显下降(P<0.05)。见表2、3。
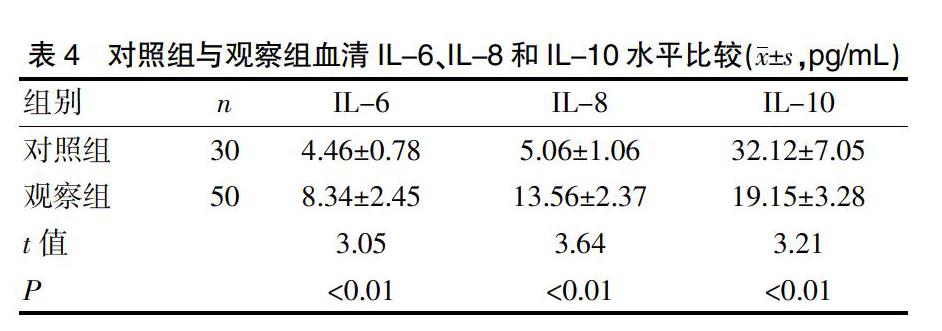
2.2 对照组与观察组以及观察组治疗前后血清IL-6、IL-8和IL-10水平比较
观察组患者血清IL-6、IL-8水平明显高于对照组,IL-10水平明显低于对照组(P<0.01);治疗7 d后,观察组患者血清IL-6和IL-8水平较治疗前明显下降,血清IL-10水平较治疗前明显上升(P<0.05)。见表4、5。
3 讨论
近年来,研究认为疼痛介质DA、NE和5-HT在LDH发病机制中的作用越来越受到重视。疼痛是LDH患者最主要最明显的症状,主要由神经根压迫及其导致的神经代谢紊乱所致,LDH患者局部或全身疼痛时疼痛介质大量分泌,促使疼痛感受放大,测定疼痛介质水平可判断患者的疼痛测定[10-12]。DA、NE和5-HT是目前已知与疼痛发生及加剧密切相关的疼痛介质,DA、NE和5-HT三者均具有明显的直接致痛作用,主要通过第二信使作用于局部,刺激感觉神经末梢而产生疼痛[13-15]。本研究发现观察组患者血清DA、NE和5-HT水平明显高于对照组。提示LDH急性期存在血清疼痛介质DA、NE和5-HT水平异常升高;同时研究還发现治疗7 d后,观察组患者血清DA、NE和5-HT水平较治疗前明显下降。提示血清疼痛介质DA、NE和5-HT水平的变化可作为LDH急性期治疗疗效随访和预后评估的敏感血清指标。
近年来研究认为,炎症因子IL-6、IL-8和IL-10在LDH发病机制中的作用越来越受到重视。研究认为LDH患者的神经根性疼痛与局部炎症关系密切,一方面LDH患者髓核本身对硬膜囊及神经根均有致炎作用;另一方面巨噬细胞浸润及血管新生可以形成椎间盘边缘区域肉芽组织,进一步加剧局部炎症反应[16-18]。当LDH患者疼痛加重时,刺激大量炎症介质释放,促炎症因子IL-6、IL-8等分泌释放量明显增加,抗炎症因子IL-10释放量明显减少,加重组织细胞发生炎症损伤,炎症损伤进一步扩大疼痛感受,两者形成恶性循环[19-21]。IL-6、IL-8是体内主要的促炎症因子,可促进炎症细胞在病灶部位的聚集、活化,加重炎症反应,参与LDH发病过程[22]。IL-10主要是由T淋巴细胞和单核巨噬细胞分泌的一种抗炎症因子,主要通过间接抑制促炎症因子的分泌释放,下调体内炎症反应,参与LDH发病过程[23]。有研究发现,随着LDH伴疼痛患者血清TNF-α和IL-6水平升高,其腰腿痛症状越明显,TNF-α和IL-6在突出的椎间盘组织及周围有较高的表达活性,可通过影响椎间盘基质降解酶的抑制酶而发挥作用[24-26]。因此,通过干预或调节炎症因子水平,使得促炎/抗炎平衡得到优化,消除神经根部位的炎症水肿,抑制炎症反应是目前治疗LDH的新方向。观察组患者血清IL-6、IL-8水平明显高于对照组,IL-10水平明显低于对照组,提示LDH急性期存在促炎症/抗炎症因子网络水平紊乱,血清IL-6、IL-8水平的异常升高,血清IL-10水平异常下降。治疗7 d后,观察组患者血清IL-6和IL-8水平较治疗前明显下降,血清IL-10水平较治疗前明显上升。提示血清炎症因子IL-6、IL-8和IL-10水平的变化可作为LDH急性期治疗疗效随访和预后评估的敏感血清指标。
总之,LDH急性期存在血清疼痛介质DA、NE和5-HT水平异常升高,其水平的变化可作为LDH急性期疗效随访和预后评估的敏感血清指标;同时LDH急性期存在促炎症/抗炎症因子网络水平紊乱,血清IL-6、IL-8水平的异常升高,血清IL-10水平异常下降,其水平的变化亦可作为LDH急性期治疗疗效随访和预后评估的敏感血清指标。因此,如何通过有效的干预措施去调控这些疼痛介质与炎症因子,从而可以预防和治疗LDH对人们带来的痛楚,以及如何进一步研究上述疼痛介质与炎症因子对于LDH的损害机制还有待于进一步研究。
[参考文献]
[1] Masuda K,Oegema TR Jr,An HS. Growth factors and treatment of intervertebral disc degeneration[J]. Spine,2004,29(23):2757-2769.
[2] Atlas SJ,Keller RB, Wu YA,et al. Long-term outcomes of surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation:10 year results from the maine lumbar spine study[J].Spine,2005,30(8):927-935
[3] 晁满香,李建军,许昌泰,等. 腰椎间盘突出症伴疼痛患者血清细胞因子的改变[J]. 现代检验医学杂志,2018, 33(2):19-22.
[4] Han YX,Liang D,Han XR,et al. Comparative analysis of the influence of fructus ligustri lucidi on a rat lumbar disc herniation model[J].Mol Med Rep,2015,12(1):1225-1232.
[5] 朴起范,郭长青,付伟涛,等.针刀疗法对腰椎间盘突出症根性神经痛大鼠血清IL-1和IL-6的影响[J].安徽中医药大学学报,2014,33(6):42-45.
[6] 曹越,章薇.针药结合对寒湿证腰椎间盘突出症患者血清IL-6和TNF-α的影响[J].针灸临床杂志,2016,32(1):8-9.
[7] Han KT,Lee HJ,Park EC,et al.Length of stay and read-mission in lumbar intervertebral discdisorder inpatients by hospital characteristics and volumes[J].Health Policy,2016,120(9):1008-1016.
[8] 胡有谷.腰椎间盘突出症[M].等4版.北京:人民卫生出版社,2011:370.
[9] Elseberq CL,Salziq D,Czermak P. Bioreactor expansion of human mesenchymal stem cells according to GMP requirements[J].Methods Mol Biol,2015,1283(10):199-218.
[10] 于志坚,吕凯,艾启利.选择性神经根阻滞治疗腰椎间盘突出症疼痛的疗效及对血清疼痛及炎症介质的影响[J].中国医药导刊,2017,19(3):223-224.
[11] 宋志刚,牛小育.腰椎间盘突出症患者血清指标与疼痛程度的关系研究[J].河北医学,2015,21(12):1947-1949.
[12] 李育刚.腰椎间盘突出患者血清疼痛物质及炎性应激指标的变化研究[J].中国骨与关节外科,2014,7(6):472-474.
[13] Khizhniak MV,Makeeva TI,Priǐmak IV.Correlation of clinico-neurological peculiarities and morphological signs of small hernias (protrusion) of the lumbar intervertebral discs in formation of discogenic pain syndromes in patients of different age[J].Klin Khir,2014,16(1):41-43.
[14] Tulloch I,Papadopoulos MC. Giant central lumbar disc herniaions:A case for the transdural approach[J].Ann R Coll Surq Enql,2018,100(3):e53-e56.
[15] 劉世伟.针刺联合椎间孔镜治疗对腰椎间盘突出症患者疼痛介质、神经功能及应激反应的影响[J].海南医学院学报,2017,23(18):2524-2527.
[16] Shiri R,Karppinen J,Leino-Arjas P,et al. Cardiovascular and lifestyle risk factors in lumbar radicular pain or clinically defined sciatica:A systematic review[J].Eur Spine J,2007,16(12):2043-2054.
[17] 徐志国,侯勇,张沿洲.老年腰椎间盘突出症患者椎间盘细胞因子水平改变及临床意义[J].中国老年学杂志,2016,36(18):4530-4531.
[18] Wahlstrom J,Burstrom L,Nilsson T,et al. Risk factors for hospitalization due to lumbar disc disease[J].Spine,2012,37(15):1334-1339.
[19] 孙中仪,田纪伟.白细胞介素与椎间盘退变的研究进展[J].中国矫形外科杂志,2014,22 (30):249-252.
[20] Kalliolias GD,Ivashkiv LB. TNF biology,pathogenic mechanisms and emerging therapeutic strategies[J]. Nat Rev Rheumatol,2016,12(1):49-62.
[21] 陈杰.外周血IL-1β和IL-6水平与腰椎间盘突出症腰腿痛疼痛程度的临床研究[J].实用预防医学,2012,19(12):1877-1878.
[22] 朱换平,赵继荣,邓强.杜仲腰痛丸对腰椎间盘突出症患者血清TNF-α、IL-1β的影响[J].西部中医药,2015, 28(4):103-106.
[23] 侯桂红,李倩,谢燕.椎间盘组织中炎症因子水、MMPsTIMPs表达与腰椎间盘突出症的关系研究[J].中国实验诊断学,2018,22(5):791-794.
[24] Smith LJ,Chiaro JA,Nerurkar NL,et al. Nucleus pulposus cells synthesize a functional extracellular matrix and respond to inflamma-tory cytokine challenge following long-term agarose culture[J]. Eur Cell Mater,2011,22(4):291-301.
[25] 舒劍臣,唐小穗.P物质、白介素6与腰椎间盘突出症所致腰腿痛的相关性研究[J].中国骨与关节损伤杂志,2013,28(9):825-827.
[26] Khizhniak MV,Priǐmak EV. Epidural pharmacotherapy in the treatment of the pain syndrome in osteochondrosis complicated by intervertebral discs protrusion of lumbar part of the vertebral column[J]. Klin Khir,2013,15(3):44-46.
(收稿日期:2019-03-22)
