健骨方预防椎体成形术后再发骨折的疗效观察
2020-05-06张伟李伟田峰张志强朱先龙
张伟 李伟 田峰 张志强 朱先龙


【摘要】 目的:觀察北京市怀柔区中医医院院内制剂健骨方对骨质疏松性椎体压缩骨折椎体成形术后再发骨折的预防效果。方法:选取2015年1月-2016年1月本院收治的单一椎体压缩骨折患者116例,随机将患者分为观察组和对照组,每组58例。对照组予经皮椎体后凸成形术治疗,观察组予经皮椎体后凸成形术治疗后结合健骨方加减治疗。对两组患者进行为期2年的随访,分别于术后1周、1年、2年对患者进行骨密度(BMD)检测,通过Oswestry功能障碍指数问卷表(ODI)评估功能障碍,WHO疼痛缓解程度标准评估治疗效果,对疼痛复发加重的患者,应用MRI检查确诊是否再发骨折。结果:最终纳入统计的患者111例,其中观察组56例、对照组55例。观察组患者术后1周、1年、2年的治疗总有效率虽均高于对照组,但差异均无统计学意义(P>0.05)。术后1、2年,对照组腰椎、髋部骨密度值均低于观察组,差异均有统计学意义(P<0.05)。术后2年,观察组再发骨折例数少于对照组,差异有统计学意义(P<0.05)。术后1年,观察组的日常生活自理能力、提物、疼痛评分均优于对照组,差异均有统计学意义(P<0.05);术后2年,观察组的日常生活自理能力、提物、睡眠、社会活动、旅行、疼痛评分均优于对照组,差异均有统计学意义(P<0.05)。结论:骨质疏松性椎体压缩骨折椎体成形术手术效果肯定,北京市怀柔区中医医院骨科院内制剂健骨方具有改善骨质疏松,降低椎体再发骨折的作用,可明显改善患者术后的远期功能。
【关键词】 椎体压缩骨折 椎体成形术 健骨方
The Effect of Jiangu Formula on Prevention of Recurrent Fracture after Vertebroplasty/ZHANG Wei, LI Wei, TIAN Feng, ZHANG Zhiqiang, ZHU Xianlong. //Medical Innovation of China, 2020, 17(02): 005-009
[Abstract] Objective: To observe the preventive effect of Jiangu Formula in the Huairou District Hospital of Traditional Chinese Medicine on the recurrent fracture after vertebroplasty for osteoporotic vertebral compression fracture. Method: From January 2015 to January 2016, 116 patients with a single vertebal compression fracture were selected, they were randomly divided into observation group and control group, 58 cases in each group. The control group was treated with percutaneous kyphoplasty, and the observation group was treated with percutaneous kyphoplasty combined with Jiangu Formula. The patients in the two groups were followed up for 2 years. The BMD of the patients were measured at 1 week, 1 year and 2 years after the operation. The dysfunction was assessed by the Oswestry Disability Index questionnaire (ODI), and the treatment effect was assessed by the WHO pain relief standard. For the patients with pain recurrence and aggravation, MRI was used to check whether there was recurrent fracture. Result: 111 patients were included in the final statistics, include 56 patients in the observation group and 55 patients in the control group. Although the total effective rate of the observation group at 1 week, 1 year and 2 years after surgery were higher than those of the control group, but the differences were not statistically significant (P>0.05). 1 year and 2 years after operation, the BMD of lumbar vertebrae and hip in the control group were lower than those in the observation group, the differences were statistically significant (P<0.05). 1 year after the operation, the daily self-care ability, extract and pain of the observation group were all better than those of the control group, with statistically significant differences (P<0.05); 2 years after the operation, daily life self-care ability, extract, sleep, social activities, travel and pain in the observation group were better than those of the control group, with statistically significant differences (P<0.05). Conclusion: The effect of vertebroplasty for osteoporotic vertebral compression fracture is positive, the preparation of Jiangu Formula in the orthopedic department of Huairou District Hospital of Traditional Chinese Medicine in Beijing has the effect of improving osteoporosis and reducing the recurrence fracture of vertebral body, which can significantly improve the long-term function of patients after operation.
[Key words] Vertebral compression fracture Vertebroplasty Jiangu Formula
First-authors address: Hospital of Traditional Chinese Medicine, Huairou District, Beijing 101400, China
doi:10.3969/j.issn.1674-4985.2020.02.002
随着我国平均寿命增加,目前老年人普遍存在骨质疏松的情况,骨质疏松使椎体脆性增加,胸腰段椎体是力的主要承受部位,故易发生椎体压缩性骨折[1-3]。其临床主要症状为腰背部疼痛,严重影响中老年人的日常生活质量。目前经皮球囊扩张后凸成形术(percutaneous kyphoplasty,PKP)和经皮椎体成形术(percutaneous vertebroplasty,PVP)是治疗骨质疏松性椎体压缩骨折的主要方式,创伤小、可迅速止痛,改善功能障碍,有效提高老年患者生活质量[4-7]。再发骨折是术后常见并发症,中医药制剂对再发骨折的预防成为中医系统研究热点,本院骨科对2015年1月-2016年1月收治的116例椎体成形术后患者进行中药干预并随访研究,以期观察健骨方对单纯骨质疏松性椎体压缩骨折成形术后再发骨折的预防疗效,现将研究结果报道如下。
1 资料与方法
1.1 一般资料 抽选2015年1月-2016年1月本院收治的单一椎体压缩骨折患者116例,纳入标准:符合原发性骨质疏松症诊断标准;明确诊断单一椎体压缩性骨折(MRI提示新鲜压缩骨折);无明显手术禁忌证。排除标准:有明确外伤病史;伴有较严重基础疾病者。其中男10例,女106例,年龄55~89岁,平均(69.4±7.3)岁,病程3~16 d,平均(6.6±2.2)d。随机将患者分为观察组和对照组,各58例。观察组:2例患者无法完成长期服用汤药,56例入组;对照组:2例患者失访,1例患者死亡,55例入组;最终纳入统计111例。此次研究已得到本院伦理委员会批准,患者均签署治疗及随访知情同意书。
1.2 方法 (1)对照组予经皮椎体后凸成形术治疗。患者取俯卧位,C型臂定位患椎,局部麻醉后经椎弓根穿刺,导管针至椎体中前1/3处,调和骨水泥后在C型臂透视下缓慢注入椎体。术毕观察双下肢感觉活动,术后24 h腰围保护下地活动。(2)观察组予经皮椎体后凸成形术治疗后结合健骨方加减治疗。两组患者术后均予健康宣教、协助指导锻炼腰背肌肉,术后第2天下地行走复查X线片,术后第3天出院;出院后均于门诊予骨化三醇、碳酸钙等钙剂药物服用,观察组患者额外服用健骨方,该方由北京市怀柔区中医医院骨科院内制剂,主要组成如下:补骨脂12 g、骨碎补12 g、淫羊藿9 g、怀牛膝15 g、蛇床子6 g、桑葚15 g、黄芪30 g、杜仲15 g等。辨证加减,阴虚者加用乌梅、酒黄精、地骨皮等;血瘀者加用桃仁、红花等。隔天服1剂,早晚分服,间隔3个月复查肝肾功,半年后停服。两组患者均随访24个月。
1.3 观察指标与评价标准 (1)比较两组治疗效果,以WHO疼痛缓解程度为评价标准。完全缓解(CR):治疗后完全无痛;部分缓解(PR):疼痛较治疗前明显减轻,基本不影响睡眠,能正常生活;轻度缓解(MR):疼痛较治疗前有所减轻,但仍明显,睡眠受影响;无效(NR):治疗前后疼痛程度无变化。总有效率=(CR例数+PR例数)/总例数×100%。(2)通过双能X线骨密度仪检测,比较两组术后1周、1年、2年的腰部、双髋部骨密度数值(BMD)。(3)比较两组Oswestry功能障碍指数评分。Oswestry功能障碍指数量表评价内容包括日常生活自理能力、提物、行走、坐、站立、睡眠、社会活动、旅行、疼痛程度等情况,每项内容评分为0~5分,分数越高功能越差。(4)对疼痛复发加重的患者,应用MRI检查确诊是否再发骨折。
1.4 统计学处理 采用SPSS 15.0软件对所得数据进行统计分析,计量资料用(x±s)表示,比较采用t检验;计数资料以率(%)表示,比较采用字2检验。P<0.05为差异有统计学意义。
2 结果
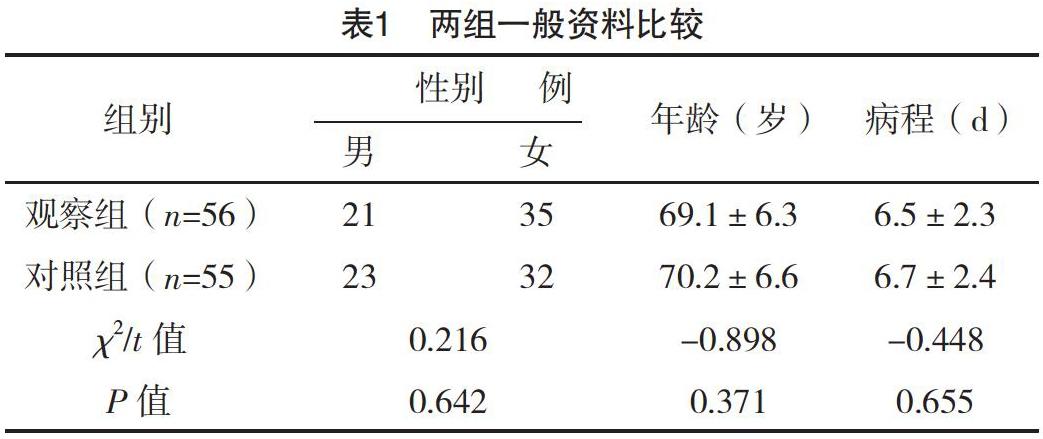
2.1 两组一般资料比较 两组患者的一般资料比較,差异均无统计学意义(P>0.05),具有可比性,见表1。
2.2 两组术后疼痛缓解效果比较 观察组患者术后
1周、1年、2年的治疗总有效率虽均高于对照组,但差异均无统计学意义(字2=0.000、1.392、1.582,P=0.985、0.238、0.209),见表2。
2.3 两组术后腰椎、髋部骨密度比较 两组术后1周腰椎、髋部骨密度值比较,差异均无统计学意义(P>0.05);术后1、2年,对照组腰椎、髋部骨密度值均低于观察组,差异均有统计学意义(P<0.05)。见表3。
2.4 两组术后再发骨折情况比较 术后1年,两组再发骨折情况比较,差异无统计学意义(P>0.05);术后2年,观察组再发骨折例数少于对照组,差异有统计学意义(P<0.05)。见表4。
2.5 两组术后Oswestry功能障碍指数评分比较 术后1周,两组患者在Oswestry功能障碍指数中9个方面比较,差异均无统计学意义(P>0.05);术后1年,观察组的日常生活自理能力、提物、疼痛评分均优于对照组,差异均有统计学意义(P<0.05);术后2年,观察组的日常生活自理能力、提物、睡眠、社会活动、旅行、疼痛评分均优于对照组,差异均有统计学意义(P<0.05)。见表5。
3 讨论
PKP和PVP是治疗骨质疏松性胸腰椎体压缩性骨折的主要方式之一,疗效已经得到文献[8-11]研究证实,但随着患者年龄增加,骨质疏松加重,使患者再次出现腰背部疼痛甚至骨折,进而影响术后患者的远期效果,所以系统全程的抗骨质疏松治疗才是治疗疾病的根本,符合中医理论“标本兼治”。
经脉受损、气机失调、血不循经溢于脉外、离经之血瘀滞于肌肤腠理为产生疼痛的主要原因[12]。经过椎体成形术后,主要病机由血瘀气滞转变为肾虚、脾虚有关;中医学认为“肾为先天之本,主生长发育”“肾藏精,主骨生髓”,如肾精亏损则不能滋养全身之骨,则骨枯髓减,导致骨痿。结合中医基础理论及现代药理研究,笔者提出了治疗椎体压缩骨折术后骨质疏松症的主要原则为补肾壮骨、健脾益氣、活血通络,据此原则组方,研制出防治骨质疏松症的健骨方。该方以补骨脂补肾助阳壮骨为君药;辅之骨碎补、淫羊藿加强其补肾壮阳之功为臣药;同时配以黄芪补中益气;杜仲、桑葚补益肝肾,此乃“善补阳者,必于阴中求阳”和“壮水之主,以制阳光”之意。现代药物实验研究表明,较高浓度补骨脂对分离破骨细胞性骨吸收有抑制作用,它抑制了骨吸收陷窝的增加和扩大[13]。补骨脂中的有效成分异补骨脂素能显著促进骨髓间充质干细胞的成骨性分化,从而起到抗骨质疏松的作用[14]。淫羊藿可通过保护性腺、抑制骨吸收和促进骨形成等途径,使机体骨代谢处于骨形成大于骨吸收的正平衡状态,抑制骨量丢失,防止骨质疏松的发生[15]。
本研究结果显示,术后1、2年,对照组腰椎、髋部骨密度值均低于观察组,差异均有统计学意义(P<0.05);且术后2年,对照组发生再骨折的例数明显多于观察组(P<0.05),这说明健骨方在治疗过程中可以维持平稳骨密度,从而降低椎体再骨折的风险。两组患者在症状改善及治疗总有效率方面,差异均无统计学意义(P>0.05),充分肯定了PKP和PVP的手术效果。术后1年,观察组的日常生活自理能力、提物、疼痛评分均优于对照组,差异均有统计学意义(P<0.05);术后2年,观察组的日常生活自理能力、提物、睡眠、社会活动、旅行、疼痛评分均优于对照组,差异均有统计学意义(P<0.05);充分说明了中药补肾健骨治疗对骨质疏松性胸腰椎体压缩性骨折的具有较好的远期疗效。
综上所述,椎体成形术是目前临床治疗骨质疏松性椎体压缩骨折的主要方法,健骨方能提高骨密度,降低椎体再骨折的风险,明显改善患者术后的功能和症状。
参考文献
[1] Bae J S,Park J H,Kim K J,et al.In Reply to the letter to the editor regarding “analysis of risk factors for secondary new vertebral compression fracture following percutaneous vertebroplasty in patients with osteoporosis”[J].World Neurosurg,2017,99:387-394.
[2] Wang Y,Zhong H,Zhou Z,et al.Letter to the editor regarding “analysis of risk factors for secondary new vertebral compression fracture following percutaneous vertebroplasty in patients with osteoporosis”[J].World Neurosurg,2017,103:924-925.
[3] Lee D G,Park C K,Park C J,et al.Analysis of Risk Factors Causing New Symptomatic Vertebral Compression Fractures After Percutaneous Vertebroplasty for Painful Osteoporotic Vertebral Compression Fractures[J].Journal of Spinal Disorders & Techniques,2015,28(10):E578.
[4] Yan L,He B,Guo H,et al.The prospective self-controlled study of unilateral transverse process-pedicle and bilateral puncture techniques in percutaneous kyphoplasty[J].Osteoporos Int,2016,27(5):1849-1855.
[5] Gu Y T,Zhu D H,Liu H F,et al.Minimally invasive pedicle screw fixation combined with percutaneous vertebroplasty for preventing secondary fracture after vertebroplasty[J].J Orthop Surg Res,2015,10:31.
[6] Firanescu C E,De Vries J,Lodder P,et al.Percutaneous Vertebroplasty is no Risk Factor for New Vertebral Fractures and Protects Against Further Height Loss (VERTOS IV)[J].CardioVascular and Interventional Radiology,2019,42(7):991-1000.
[7] Xie L L,Chen X D,Yang C Y,et al.Efficacy and complications of 125I seeds combined with percutaneous vertebroplasty for metastatic spinal tumors: a literature review[J].Asian Journal of Surgery,2019,36(8):1020-1024.
[8] Yan L,He B,Guo H,et al.The prospective self-controlled study of unilateral transverse process-pedicle and bilateral puncture techniques in percutaneous kyphoplasty[J].Osteoporos Int,2016,27(5):1849-1855.
[9] Gu Y T,Zhu D H,Liu H F,et al.Minimally invasive pedicle screw fixation combined with percutaneous vertebroplasty for preventing secondary fracture after vertebroplasty[J].J Orthop Surg Res,2015,10:31.
[10] Shiva S J J,Roah M,Stefanos F,et al.Imaging Improves Efficacy of Vertebroplasty-A Systematic Review and Meta-Analysis[J].The Canadian Journal of Neurological Sciences.Le Journal Canadien Des Sciences Neurologiques,2019,46(5):1-33.
[11] Ge Z,Ma R,Chen Z,et al.Uniextrapedicular kyphoplasty for the treatment of thoracic osteoporotic vertebral fractures[J].Orthopedics,2015,36(8):e1020-1024.
[12]孫月钊,郭宁国,强晓军,等.骨质疏松性骨折术后再发骨折的危险因素分析[J].深圳中西医结合杂志,2019,29(7):79-81.
[13]王丹丹,王琛,郭奥林.椎体成形术后再发骨折的临床研究进展[J].世界最新医学信息文摘,2018,18(A2):130,133.
[14]丁小力,王燕,闫海珠,等.椎体成形术后邻椎新发骨折特征与相关因素分析[J].宁夏医学杂志,2018,40(12):1193-1195.
[15]梅治,李青,赵成毅,等.经皮椎体成形术后非手术椎体再发骨折的危险因素分析[J].中国医刊,2018,53(4):397-400.
(收稿日期:2019-06-26) (本文编辑:张爽)
①北京市怀柔区中医医院 北京 101400
通信作者:张伟
