Total endovascular repair of an intraoperative stent-graft deployed in the false lumen of Stanford type A aortic dissection:A case report
2020-04-25XuRanLiYuanHaoTongXiaoQiangLiChangJianLiuChenLiuZhaoLiu
Xu-Ran Li,Yuan-Hao Tong,Xiao-Qiang Li,Chang-Jian Liu,Chen Liu,Zhao Liu
Abstract
Key words: Type A dissection; False lumen stent graft implantation; Endovascular repair;3D printing; Thoracoabdominal aortic dissection; Case report
INTRODUCTION
The use of elephant trunk stent can prevent distal residual dilation and anastomotic leakage after total arch replacement and shows survival benefits[1,2].Unfortunately,when the true lumen is too compressed to identify,the stent may enter the false lumen.The prevalence of intraoperative stent-graft deployed in the false lumen is relatively rare.However,malignant stent implantation is also a complication of thoracic endovascular aortic repair.Therefore,every surgeon should pay more attention to its treatment.We report our experience with total endovascular repair of an intraoperative stent-graft deployed in the false lumen.
CASE PRESENTATION
Chief complaints
At 2 years after surgery for aortic dissection,chest tightness lasted for 1 mo.
History of present illness
The patient was admitted to the department of cardiothoracic surgery of our hospital 2 years prior due to repeated chest tightness.He underwent ascending aortic replacement,total arch replacement,and descending aortic stent implantation for Stanford type A aortic dissection on January 2016.The patient recovered well after the operation and the symptom of chest tightness was slightly relieved.However,1 mo ago,the patient felt chest tightness after a little exercise,accompanied by left limb paresthesia,and it was only slightly relieved after rest.The patient had no chest or back lancinate pain or radiating pain,and no nausea,vomiting or other discomfort.
由化脓性链球菌敏感菌株的轻至中度急性扁桃体炎、咽炎,以及由肺炎链球菌敏感菌株或流感嗜血杆菌(仅包括非产β‐内酰胺酶菌株)引起轻至中度急性细菌性上颌窦炎。
History of past illness
The patient underwent surgery for aortic dissection 2 years prior.He had hypothyroidism for 2 years and was treated with Euthyrox.In addition,he had a history of coronary heart disease for 1 mo.
Personal and family history
The patient’s parents were healthy and his personal history was normal.
Physical examination upon admission
On admission,the patient's body temperature was 36.8°C,pulse was 95 times/min,and blood pressure was 159/77 mm/Hg.His breathing was steady,averaging 18 breaths per minute.The patient had an old surgical scar in the middle of chest,no deformity of chest and breath sounds in both lungs were normal.There was no abnormal uplift in his precardiac region,and no obvious expansion of his cardiac dullness boundary.His heart rate was regular at 95 beats/min and there was no pathological murmur.The patient has a weak carotid pulse on the right side.There were no positive signs in abdomen and no swelling in the lower limbs.
Laboratory examinations
There was no significant abnormality in preoperative blood routine and stool routine examination,and the occult blood test was negative.The patient had hypothyroidism,presenting with elevated thyrotrophin(83.41 mIU/L) and multiple positive thyroid antibodies.Biochemical examination showed that the estimated glomerular filtration rate was 77.2 mL/min/1.73 m2,and urine protein was weakly positive in urine analysis,indicating slightly abnormal renal function.
Imaging examinations
Vascular ultrasound revealed dissection in the right carotid artery and the blood was decreased in the right internal carotid artery.The stenosis of the innominate artery was approximately 50%-69%.There was no obvious abnormality in the right subclavian artery.An intraoperative stent-graft was deployed in the false lumen inadvertently in the surgery 2 years prior.This caused severe iatrogenic thoracic and abdominal aortic dissection,and the dissection involved many visceral arteries.The computed tomography angiography (CTA) showed that the blood supply of celiac artery and superior mesenteric artery came from the true lumen and the blood supply of both renal arteries came from the true and false lumen (Figure 1).CTA examination of the neck revealed that the stent of the innominate artery was located in the false lumen,and the right internal carotid artery also formed dissection.The patient survived after the wrong stent implantation,because there were a large number of intimal tears in the distal aorta which communicated between the true and false lumens.A series of endovascular operations were performed to address the intractable situation (Table 1).
FINAL DIAGNOSIS
Thoracic aortic dissection (after stent implantation),coronary heart disease,hypothyroidism,and cholecystolithiasis.
TREATMENT
Stage 1
In July 2018,left subclavian artery-right carotid artery artificial vascular bypass surgery was performed to repair the right common carotid artery dissection (Figure 2A).After 1 mo,thoracic endovascular aortic repair was performed.Under general anesthesia,an occluder (28 mm,WBFDQ-I 16,Shanghai memory alloy) was used to occlude the true lumen (Figure 2B).A covered stent (32 mm × 200 mm,Ankura,Ankuracompany,China) was deployed through the intimal tear to overlap with the original stent in the false lumen for approximately 3 cm.The proximal end of the covered stent was in the false lumen and the distal end was in the true lumen.It drew the blood flow back to the true lumen successfully (Figure 2C).A CTA examination 3 mo after surgery showed that the descending aortic dissection was completely repaired (Figure 2D-F).
Stage 2
The patient underwent the second stage of surgery in December 2018.Before surgery,the positions of the visceral arteries were located by the three-dimensional (3D)printing technique.The 3D printing guide plate was designed by Geomagic Design Direct 2014 software.During the operation,the covered stent (28 mm × 24 mm × 160 mm,Ankura,Ankura Company,China) was fenestrated at the positions of the celiac trunk artery,superior mesenteric artery,and bilateral renal arteries according to the custom 3D printing model.A very short-branched stent was sutured at the position of left renal artery to avoid endoleak (Figure 3A,B).The customized stent was deployed in the true lumen of abdominal aorta from the right femoral approach.Then two branched stents were deployed in the superior mesenteric artery,and the right renal artery and balloons were used to expand these branched stents.Another two covered stents were deployed at the distal end of the fenestrated stent to deal with endoleak(Figure 3C,D).The thoracic and abdominal aortic dissection was successfully repaired,with all the visceral arteries preserved.The operation lasted approximately 7.5 h and the radiation dose was 1529 mGy.The volume of intraoperative hemorrhage was approximately 500 mL and the blood transfusion volume was approximately 600 mL.
Patients were given oral antihypertensive drugs to control their blood pressure every day after discharge.The patient received long-term antiplatelet managementwith rivaroxaban (5 mg/d) and aspirin (100 mg/d) to prevent in-stent restenosis.In addition,regular examinations of aortic CTA were necessary.
住宅工程质量,直接关系到千家万户的切身利益。随着百姓维权意识的逐渐提高,住宅工程质量投诉不断增加,甚至群诉群访时有发生。2009年住房城乡建设部印发了《关于做好住宅工程质量分户验收工作的通知》(建质〔2009〕291号),要求各省市建立住宅工程逐套验收制度,督促建设、施工、监理等参建单位认真履行法定义务,提高住宅工程质量水平,维护业主的合法权益,减少投诉。2009年分户验收工作的实施,在一定程度上促进了我国建筑工程质量水平的整体提高,但仍需要做好以下工作:

Table 1 Timeline
OUTCOME AND FOLLOW-UP
The patient suffered from acute renal failure after the thoracic aortic stent implantation and interventional occlusion operation.However,he did not develop renal failure or spinal cord injury after the second EVAR.A computed tomography scan was performed at 3 mo after the operation.The results showed that all of the stents were in the right positions and all of the branch arteries were patent (Figure 3E).
DISCUSSION
Inappropriate deployment of the stent-graft into the false lumen may lead to hypoperfusion of important viscera and lethal aortic rupture during or after surgery.This patient survived after previous catastrophic stent implantation because there were a large number of intimal tears,which communicated between the true and false lumens but eventually led to severe aortic disease.There are many ways to rescue incorrect stent implantation.Conventional open surgery can be adopted to replace the relevant aortic segments.However,this kind of surgery is very dangerous in high-risk patients and requires extracorporeal circulation[3,4].EVAR was proved to be minimally invasive and had lower perioperative morbidity and mortality than open surgery[5-7].However,this less invasive approach still has several complications such as spinal cord injury,renal failure,and neurological complications[8,9].Thus,operations need to be well designed to reduce these complications (Figure 4).
This operation had several technical challenges.First,we need to divert blood to the true lumen.Maet al[10]adopted fenestration technique to puncture the septum between lumens,artificially creating a break to connect the true and false lumens.Then,a covered stent was deployed through the break to connect the true and false lumens.In this way,the blood was drawn back into the true lumen.In our case,fenestration was not necessary because there was already a break at the distal end of the aorta.A balloon was used to expand the break,and a covered stent was used to connect the elephant trunk stent in the original false lumen with the true lumen.An occluder was deployed at the proximal end of the true lumen to repair the anastomotic leakage to avoid high-risk fenestration of the aortic arch.Second,personalized stent was the key to retain visceral blood supply.After the first stage of surgery,we repaired the abdominal aortic dissection with a custom stent graft,which was fenestrated with 3D printing guidance.Before the implantation,the stent was released in the 3D-printed vascular model and the positions of fenestration were accurately determined by the model.
With the development of endovascular techniques,there have been many reports about successful rescue after false lumen stent-graft implantation.However,there are serious complications because of incorrect stent implantation including death from intraoperative or postoperative aortic rupture.A large amount of blood flow into the false lumen and less blood is in the true lumen which may eventually lead to multiple organ failure and even death.The pressure in the false lumen was too great which lead to the formation of a dissecting aneurysm at the distal end.Eventually the aneurysm ruptures and patients die.Thus,preventing stents from being deployed in the false lumen is the most crucial step.Some cardiac surgery departments have grasped the concept of modern hybrid aortic surgery.The guide wires can be used to locate the positions of stents and perform angiography at any time.In addition,another stent can be implanted at the distal end of elephant trunk stent to avoid possible complications.Furthermore,the hemodynamic changes in complicated dissections and position of the septum can be assessed using intravascular ultrasound[11,12].Most importantly,the true and false lumens should be carefully identified by preoperative computed tomography.Usually the true lumen is smaller and the false lumen is larger.The beak sign and a large cross-sectional area indicate a false lumen.Intimal calcification is common in the true lumen and mural thrombus is more common in the false lumen.
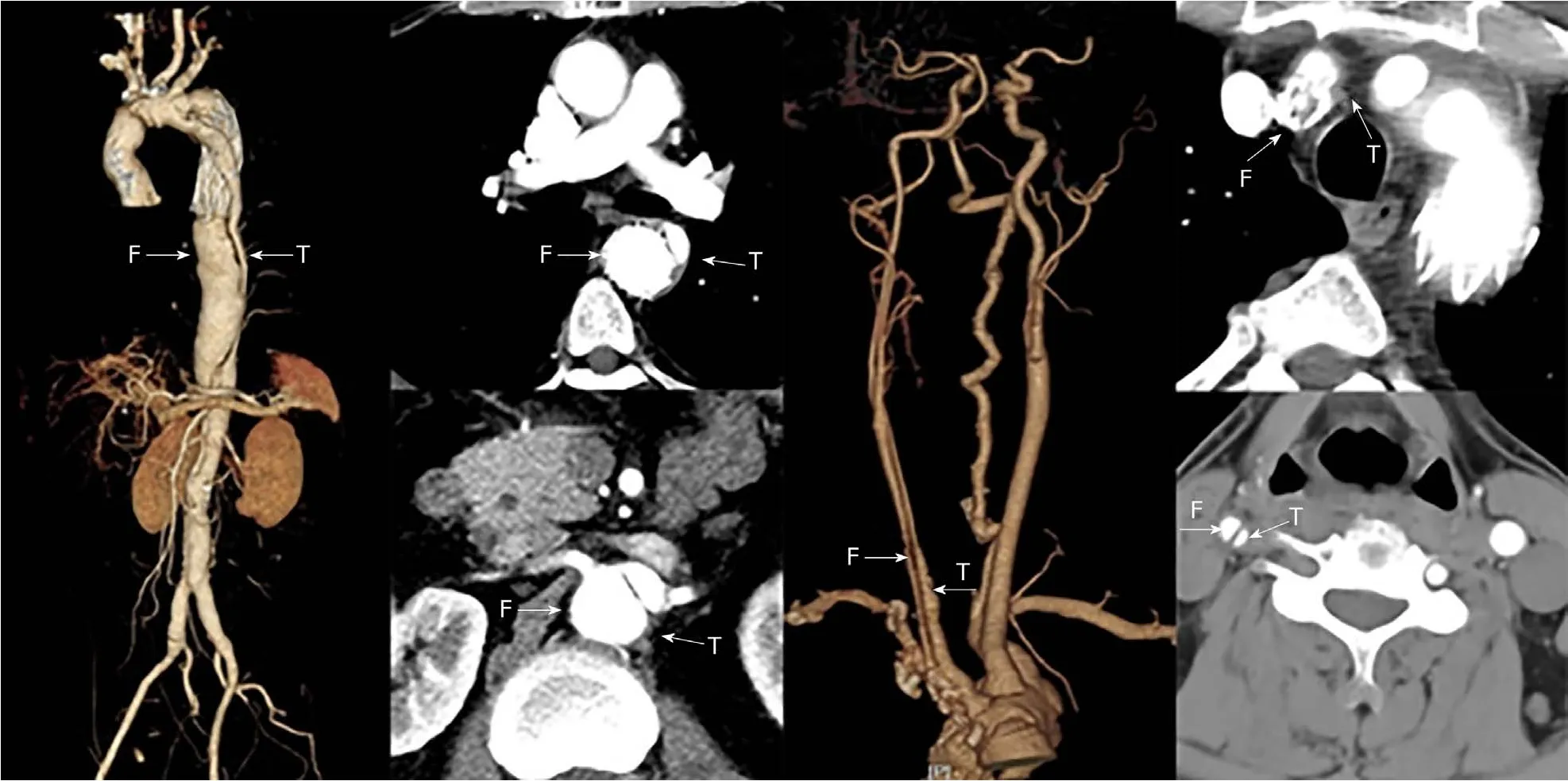
Figure 1 Preoperative computed tomography:The stents of innominate artery and thoracic aorta were located in the false lumen.
To reduce the risk of stent rupture into the false lumen,the length and size of the stents should be carefully selected according to the aortic diameter and the position of the tears before surgery[13].In addition,it is very important to ensure that the guide wire is in the true lumen.Angiography should be performed before the guide wire and catheter reach the target position and before the stents are released.We should avoid the guide wire passing between the true and false lumens and confirm both ends of the stent are in the true lumen before release.
CONCLUSION
This case shows that total endovascular repair for incorrect stent-graft implantation is feasible and minimally invasive and personalized operation planning is very important to success.Further research is still needed to evaluate its clinical effect.

Figure 2 Treatment stage 1 computed tomography.

Figure 3 3D printing model,angiography,and computed tomography scan.
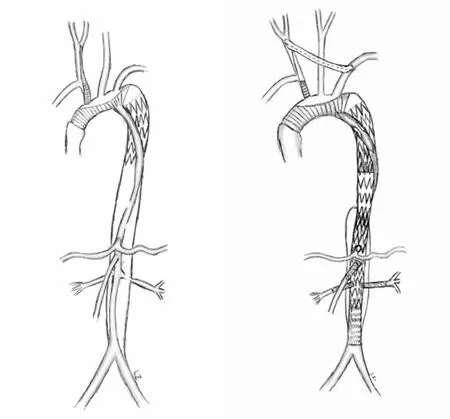
Figure 4 Operation diagram.
猜你喜欢
杂志排行

World Journal of Clinical Cases的其它文章
- Repair mechanism of astrocytes and non-astrocytes in spinal cord injury
- Study on the correlation and predictive value of serum pregnancy-associated plasma protein A,triglyceride and serum 25-hydroxyvitamin D levels with gestational diabetes mellitus
- Significance of 125I radioactive seed implantation on growth differentiation factor and programmed death receptor-1 during treatment of oral cancer
- Computed tomography-based score model/nomogram for predicting technical and midterm outcomes in transjugular intrahepatic portosystemic shunt treatment for symptomatic portal cavernoma
- Efficacy of totally laparoscopic compared with laparoscopic-assisted total gastrectomy for gastric cancer:A meta-analysis
- Allograft artery mycotic aneurysm after kidney transplantation:A case report and review of literature