Clinical study of warm acupuncture combined with massage in treatment of periathritis of shoulder
2020-04-03HeXingYuBaoLongLiJieZhang
He-Xing Yu, Bao-Long Li, Jie Zhang✉
1. Heilongjiang university of Chinese medicine, Harbin China150040
2. The second affiliated hospital of heilongjiang university of traditional Chinese medicine, Harbin China, 150040
Keywords:
ABSTRACT
1. Introduction
Periarthritis of Shoulder, also known as "Shoulder coagulation wind", is a chronic inflammatory Shoulder joint injury characterized by the patient feeling pain around the Shoulder joint and/or Shoulder joint and impaired Shoulder movement.Modern medical research believes that Periarthritis of Shoulder is mainly caused by chronic non-infectious inflammation of the Shoulder joint and surrounding connective tissue. With the progress of the disease, the inflammation gradually worsens and is accompanied by relatively extensive tissue adhesion, eventually leading to Periarthritis of Shoulder with joint pain and joint movement disorder as the main clinical characteristics[1, 2].In addition, some scholars also believe that PS can also be induced by excessive braking after trauma or irregular rehabilitation exercise after fracture [3-5].
At present, the treatment of Periarthritis of Shoulder in western medicine is very limited [2, 6, 7], In addition to the use of nonsteroidal anti-inflammatory drugs to relieve inflammation and pain,only part of the physical therapy or rehabilitation training and joint cavity closure therapy and other treatment means.The clinical effect of these treatment measures is also very limited. Conventional physical therapy can only temporarily relieve the clinical symptoms of patients, while the long-term joint pain and movement disorder greatly affect the daily life and work of patients.Although nonsteroidal anti-inflammatory drugs can alleviate shoulder pain in patients, their possible adverse reactions, such as gastrointestinal reactions, gastric ulcers, elevated transaminase, skin damage and liver and kidney damage, limit the clinical application of these drugs to a large extent.Therefore, acupuncture, moxibustion, massage manipulation and multiple combinations of drugs have become the preferred treatment for many patients and clinicians with Periarthritis of Shoulder, playing an increasingly important role in the clinical treatment of Periarthritis of Shoulder.
According to the clinical characteristics and pathogenesis of PS patients, most modern doctors attribute PS to the "shoulder syndrome" or "jingjin disease" of traditional Chinese medicine.For most patients with Periarthritis of Shoulder, there are internal and external causes.External causes for excessive strain injury, poor recovery;Periarthritis of Shoulder is formed only when internal and external joint diseases are caused by deficiency of qi and blood,weakness of viscera and blood essence in human body.For the treatment of PS, modern doctors mainly treat with acupuncture,moxibustion and massage, and cooperate with drugs, physical therapy and rehabilitation training[3, 8, 9].
This study analyzes the warm acupuncture, massage and conventional therapy to treat the clinical curative effect of pain stage of Periarthritis of Shoulder, assessment of Shoulder joint pain in patients with various treatments in reducing barriers to Shoulder joint activities differences, analysis of warm acupuncture, massage and warm acupuncture combined massage treatment of PS and the difference between conventional conservative treatment, provide a certain basis for treatment of PS.
2.Materials and Methods
2.1.Materials and Methods
In this study, a total of 120 patients with early Periarthritis of Shoulder who were admitted to the orthopedic clinic and ward of heilongjiang university of traditional Chinese medicine from June 2018 to June 2019 were selected. The patients were divided into warm acupuncture group, massage group, combined treatment group and control group by using a random number table, with 30 patients in each group.The mean age of the warm acupuncture group was 57.03±7.64 years, and the mean course of the disease was 7.80±2.85 months.The mean age of the massage group was 56.77±6.89 years,and the mean course of disease was 7.46±2.06 months.The mean age of the combined treatment group was 58.69±7.34 years, and the mean course of disease was 6.98±2.14 months.There were no significant differences in the mean age, mean course of disease,gender and type of work in each group (P >0.05).
2.2.Diagnostic and inclusion criteria
Diagnostic criteria [7, 8]: ①shoulder pain, tenderness, and with the climate or activities aggravated; ②Limited shoulder joint lift,abduction, adduction, pronation and extension; Atrophy of the shoulder muscles or typical "shouldering" phenomenon;X-ray examination is negative, a small number of patients with long-term disease can see osteoporosis.
Inclusion criteria: ①Periarthritis of Shoulder patients;②Periarthritis of Shoulder between march and December;③Between the ages of 45 and 70.
2.3Exclusion criteria
①Past history of joint injuries; ②have serious osteoporosis, tumor bone metastasis, serious heart, lung, nerve and spirit and liver and kidney diseases; ③refuse acupuncture and moxibustion therapy;④X - ray of shoulder joint appears bone ankylosis or other nonconservative treatment can resolve the serious lesions.
2.4.Therapeutic Method
Routine treatment: the patient is advised to keep the shoulder warm at ordinary times, not to be invaded by wind, cold and dampness and other external evils, and to carry out appropriate shoulder joint rehabilitation exercise independently.Patients with osteoporosis should take 2 tablets of calcium carbonate D3 chewable tablets every day/times/day, and those with unbearable pain can take fenbide temporarily (Chinese medicine approval: H10900089).Ultrashort wave treatment: ldt-cd-31 ultrashort wave was selected, and two medium electrode plates were placed symmetrically on the affected side of the patient's shoulder.The wavelength is set to 6.26m and the operating frequency is 39.57mhz.Power select micro heat.Each ultrashort wave treatment is set at 10-20 minutes.At the same time during the non-ultra-short wave treatment, huoxue and pain reliever ointment (anhui anke yuliangqing pharmaceutical co., LTD.
Wen acupuncture: choose one side shoulder Yu, shoulder liao, chien cheng and li 11, acupuncture point positioning reference fan-rong liang, wang hua editor "acupuncture" teaching material [10]. Specific operational process [10-12]: During the treatment, the patient was instructed to take the healthy side lying position, with the affected shoulder on top, and the affected shoulder fully exposed.Enter the needle vertically, twist to get air, then place a moxa bar about 2cm long at the needle handle and light the moxa bar.Each warm acupuncture treatment continued for 30 minutes.Massage therapy:told the patient to sitting, with , point, shake, according to the push,pull out, a finger zen, and, pull, shake, rub back and forth several times in the front of one side shoulder and upper arm inside, with limb passive outreach, outside activities.Each massage treatment was controlled at 15-20min.Referring to the study of massage edited by fang min and song bolin[13, 14].
Patients in the warm acupuncture group were given warm acupuncture treatment on the basis of general treatment.The massage group was given massage therapy on the basis of general treatment.The combined treatment group was given warm acupuncture combined with massage manipulation on the basis of conventional treatment.Patients in the control group were treated with ultrashort wave combined with topical drug application on the basis of conventional treatment.All patients were treated continuously for 4 weeks.
2.5.Evaluation Criterion
Assess changes in Shoulder motion and symptoms in patients with Periarthritis of Shoulder before and after treatment.VAS score and ibuprofen were used to evaluate the severity of shoulder pain [8, 12].Ibuprofen use: the overall dosage of ibuprofen sustained-release capsules during the 4-week treatment period was recorded, and the analgesic effect of each treatment regimen was evaluated.VAS score:0 to 10 was used to gradually indicate the pain level of the patient.The Melle functional score was used to assess activity limitations [8].Flexible movement of the joint was 0, mild impairment of movement was 1, moderate was 2, and severe was 3. The ability to abduct,rotate, touch the neck, touch the spine, and touch the lips was evaluated by this standard.The TCM syndrome score scale was used to evaluate the improvement of clinical symptoms in each group before and after treatment.According to the improvement degree of shoulder joint pain and shoulder movement, the therapeutic effect of different treatment schemes on PS patients was evaluated.Meanwhile, venous blood was collected to detect changes in serum inflammatory cytokines (il-2, TNF- TNF, il-1β) before and after treatment.
2.6.Serum inflammatory factors were detected by ELISA
The kit should be balanced to room temperature (20-25℃) and the required reaction plate removed.50ul of diluted standard was added into the standard hole on the plate.40ul of sample diluent was added in the sample hole to be tested on the plate and incubated at 37℃for 30 minutes.Add 50ul of enzyme-labeled reagent to each hole,except blank holes.Gently shake the mixture and incubate at 37℃for 30 minutes.Discard the liquid and shake to dry. Fill each hole with diluted washing liquid, shake for 30 seconds and then shake off the washing liquid.Add A50ul of color developer and B50ul of color developer into each hole, shake gently and mix well, and then produce color at 37℃ for 10 minutes without light.The enzyme marker plate was taken out, and 50ul of termination solution was added into each hole to stop the reaction.The absorbance value (OD value) of each hole was measured at 450nm wavelength by adjusting the blank hole to zero.The regression equation of the standard curve was calculated based on the concentration of the standard product and the corresponding OD value, and the corresponding sample concentration was calculated based on the linear regression equation based on the OD value of the sample.
2.7.Statistical methods
In this study, IBM-SPSS 26.0 was used for data processing.Measurement data with mean ±SD. One-way ANOVA was used for comparison between groups, and Tukey method was used for pretest.The rank sum test of paired samples was used for self - before- after comparison. Chi-square consistency test was used for the classified data.Non - parametric test was used for grade data and non - normal distribution. P < 0.05 was considered statistically significant.
3.Result
3.1.Patients' use of ibuprofen
According to table 1, the use of ibuprofen sustained release capsules in the warm acupuncture group, the massage group and the combined treatment group was significantly lower than that in the patients receiving ultrashort wave combined plaster (P < 0.05).We also found that ibuprofen was used least in the combination group (P< 0.05).
Table1 .Ibuprofen use in patients(grain,±s)
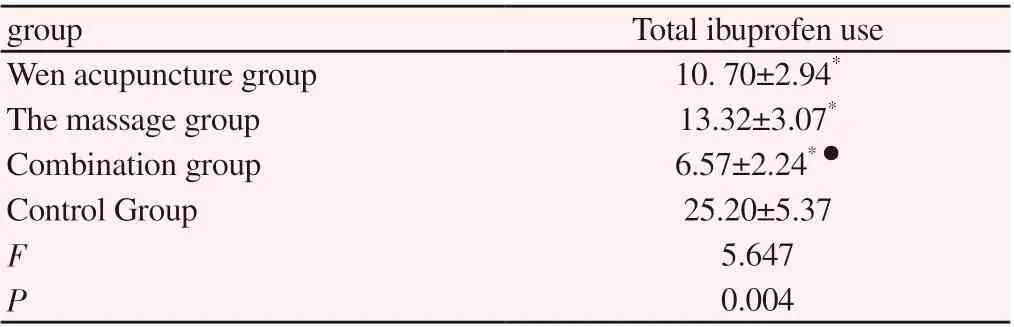
Table1 .Ibuprofen use in patients(grain,±s)
Note: * compared with Control Group, P < 0.05;Compared with Wen I group,P < 0.05;● compared with The massage group, P < 0.05
group Total ibuprofen use Wen acupuncture group 10. 70±2.94*The massage group 13.32±3.07*Combination group 6.57±2.24*▲●Control Group 25.20±5.37 F 5.647 P 0.004
3.2.Comparison of shoulder joint pain
According to table 2, symptoms of patients in all groups were improved compared with those before treatment (P < 0.05).VAS scores in all treatment groups were significantly lower than those in the control group (P < 0.05).In addition, the VAS score of patients receiving warm acupuncture combined with tuina manipulation decreased significantly more than that of patients receiving warm acupuncture or tuina manipulation alone (P < 0.05).
Table2 .VAS score of shoulder joint pain(±s)

Table2 .VAS score of shoulder joint pain(±s)
Note: * compared with Control Group, P < 0.05;Compared with Wen I group, P < 0.05;● compared with The massage group, P < 0.05
prior treatment posttreatment degree of improvement Z P Wen acupuncture group 6.47±0.94 3.17±1.21* 2.30±0.75* -4.873 <0.05 The massage group 6.20±0.87 3.32±1.11* 2.08±0.73* -4.452 <0.05 Combination group 7.01±0.74 2.09±1.31*▲● 3.68±0.68*▲● -4.754 <0.05 Control Group 6.59±0.89 5.17±1.57 1.48±0.58 -3.502 0.042 Z-0.927 -5.105 -6.266 P 0.354 <0.05 <0.05
Table3 .Melle score of shoulder joint mobility(±s)

Table3 .Melle score of shoulder joint mobility(±s)
Note: * compared with Control Group, P < 0.05;Compared with Wen I group, P < 0.05;● compared with The massage group, P < 0.05
prior treatment posttreatment degree of improvement Z P Wen acupuncture group 8.80±2.58 3.77±1.79* 5.03±1.71* -4.806 <0.05 The massage group 8.56±2.47 4.08±1.65* 4.77±1.87* -4.325 <0.05 Combination group 8.89±2.85 2.45±1.06*▲● 6.35±1.37*▲● -4.925 <0.05 Control Group 7.92±2.63 5.96±2.47 1.96±0.45 -4.663 0.021 Z-1.389 -3.369 -6.421 P 0.165 0.001 <0.05
Table4 .Improvement of TCM syndrome score of patients(±s)

Table4 .Improvement of TCM syndrome score of patients(±s)
Note: * compared with Control Group, P < 0.05;Compared with Wen I group, P < 0.05;● compared with The massage group, P < 0.05
prior treatment posttreatment degree of improvement Z P Wen acupuncture group 32.56±2.46 16.54±2.04* 16.64±1.38* -5.064 <0.05 The massage group 33.74±2.69 20.44±2.17*▲ 13.58±2.07*▲ -4.879 <0.05 Combination group 31.27±1.89 11.74±1.68*▲● 20.17±1.78*▲● -5.721 <0.05 Control Group 31.89±2.09 25.67±1.34 8.07±1.17 -4.027 0.039 Z-1.077 -4.057 -8.339 P 0.246 <0.05 <0.05
Table5 .Changes of serum inflammatory factors in patients(±s)

Table5 .Changes of serum inflammatory factors in patients(±s)
Note: * compared with Control Group, P < 0.05;Compared with Wen I group, P < 0.05;● compared with The massage group, P < 0.05
Group TNF-α(ng/L) IL-1β(ng/mL) IL-2(ng/L)prior treatment posttreatment prior treatment posttreatment prior treatment posttreatment Wen acupuncture group 11.35±6.27 6.37±1.31#* 124.38±12.39 65.87±9.34#* 10.34±3.21 6.57±1.06#*The massage group 11.57±5.37 7.24±1.37#* 130.75±13.77 83.49±10.03#*▲ 12.07±2.59 7.49±1.67#*Combination group 11.86±6.74 5.07±1.07#*● 133.46±14.07 52.77±11.64#*● 11.97±3.87 5.17±1.39#*●Control Group 11.94±5.77 10.54±1.74 128.67±13.45 113.54±10.37# 11.23±3.56 9.67±1.24#Z-1.137 -4.127 -1.048 -4.367 -0.943 -5.034 P 0.257 <0.05 0.213 <0.05 0.354 <0.05
3.3.Shoulder movement degree of improvement
According to table 3, Melle scores in each group were significantly lower than before treatment (P < 0.05).Melle scores in the warm acupuncture group, massage group and combined treatment group were lower than those in the control group (P < 0.05).Moreover, the Melle score of the combined treatment group decreased significantly more than that of the other treatment groups (P < 0.05).
3.4. Improvement level of TCM syndrome score
According to table 4, all sorts of treatment can effectively improve the patient's clinical symptoms, the treatment of TCM symptom score was significantly lower than before treatment, after its differences with significant statistical significance (P < 0.05).And the joint treatment group patients with TCM syndrome score decline were significantly greater than other groups (P < 0.05).
3.5.Changes in serum inflammatory factors after prior treatment
According to table 5, the serum inflammatory factors in Periarthritis of Shoulder patients were decreased by different treatment schemes,and the serum inflammatory factors in the warm acupuncture group,massage group and combined treatment group were significantly lower after treatment than before treatment, with statistically significant differences (P < 0.05).In addition, the combination therapy had the most significant intervention on serum inflammatory factors, and the serum inflammatory factors after treatment were significantly lower than those in other groups (P < 0.05).
3.6.Clinical efficacy analysis
In this study, 7 patients in the combined treatment group were cured, 13 were effective, and 9 were effective. The overall effective rate was 96.67%.In the warm acupuncture group, 5 patients were cured clinically, 12 were effective, 9 were effective, and the overall effective rate was 86.67%.In the massage group, 4 patients were cured clinically, 12 were effective, 12 were effective, and the overall effective rate was 93.33%.In the control group, only 1 person was cured, 4 showed significant effect, and 18 were effective, with the overall effective rate of only 76.67%.In addition, the number of cured and effective patients in the combined treatment group was significantly higher than that in other groups, and the difference was statistically significant (P < 0.05).This indicates that the effect of warm acupuncture combined with massage manipulation in the treatment of Periarthritis of Shoulder is significantly better than that of conventional physical therapy, and the patients who only use warm acupuncture therapy or massage manipulation therapy.
4.Discussion
PS is a kind of chronic shoulder arthritis caused by trauma, longterm fatigue injury or inadequate warmth, and long-term exposure to cold and wet environment.Chronic and chronic inflammatory injury of the shoulder joint and surrounding connective tissue results in peri-shoulder pain, limited mobility and other clinical symptoms.In modern medicine, Periarthritis of Shoulder is divided into three consecutive pathological stages according to the pathological characteristics of patients with Periarthritis of Shoulder. Early,middle and late stages are also called pain, adhesion and relief.The pain stage (early stage) is mainly caused by acute inflammatory injury of the shoulder joint and its surrounding tissues, and pain is often the main clinical manifestation of the patient, accompanied or not accompanied by the movement disorder of the shoulder joint.Adhesion stage (middle stage) is mainly inflammatory adhesion of the shoulder joint and surrounding ligaments, tendons, fascia and other tissues. The most important clinical manifestation of the patients is the limited shoulder movement caused by adhesion.In the remission period (later period), the patients' shoulder pain and movement disorder were improved to varying degrees, with the shoulder pain gradually alleviated and the shoulder joint movement gradually increased.At this point, increasing the blood circulation in the shoulder joint area of patients, promoting the rehabilitation of shoulder joint mobility and preventing muscle atrophy become the key of clinical diagnosis and treatment[15-19].
At present, the treatment of PS in western medicine is mainly oral NSAIDs, closed therapy, conservative physical therapy and surgical treatment.Although these treatments can alleviate pain for a short period of time, they cannot effectively improve the limited movement of the shoulder joint.At the same time, the mental and physical injury caused by surgical treatment and the adverse reactions caused by long-term use of non-steroidal anti-inflammatory and analgesic drugs greatly limited the patient's compliance.In recent years, Periarthritis of Shoulder is a new treatment.Modern medical research believes that the acute inflammatory response of the shoulder joint and surrounding tissues is the main factor in the pain stage patients, and the pathological changes of the shoulder joint in this stage appear different degrees of inflammatory exudation in the synovium of the shoulder joint.A large number of neutrophils and other inflammatory cells can be seen in the tissue, releasing a large number of inflammatory factors including TNF-, il-6, il-1 and so on.Abnormal hyperplasia of blood vessels in local tissues accompanied by inflammatory exudation is the pathological mechanism leading to joint pain and movement limitation. Therefore, emphasis is placed on the treatment to alleviate pain, reduce tissue inflammatory damage and reduce joint inflammatory stimulation.In patients with adhesion,adhesion of various tissues was the most prominent pathological change. Imaging and pathological examination showed adhesion of various soft tissues in the lesion area.At this point, the use of a variety of treatment methods to release joint adhesion, increase the ability of shoulder joint movement is the key to the treatment of such patients.Remission period is the stage of patient's slow recovery. The key of this stage is to promote the recovery of shoulder joint mobility and prevent muscle atrophy.Therefore, in the treatment emphasis on increasing local blood supply, release the adhesion of fibrous connective tissue, promote the recovery of joint function[20].
At the same time, combining the treatment methods of Periarthritis of Shoulder by stages in modern medicine with the treatment methods of traditional Chinese medicine has gradually become the hot spot of diagnosis and treatment in recent years.PS treatment by stages is consistent with the theory of "syndrome differentiation and treatment" of traditional Chinese medicine, reflecting the idea of treating diseases with the dynamic changes of the disease[21]. Warm acupuncture and massage manipulation is one of the characteristic treatment methods of traditional Chinese medicine.Numerous clinical and experimental studies have proved that warm acupuncture, massage and other characteristic therapies of traditional Chinese medicine can improve the Shoulder motion ability of patients with Periarthritis of Shoulder, relieve Shoulder pain, and improve clinical symptoms.[1, 22-24]
As for Periarthritis of Shoulder, the internal cause of Periarthritis of Shoulder is lack of tidecane and deficiency of liver and kidney essence.Such patients often have a history of years of overwork,inadequate rest, or inadequate recovery from shoulder trauma.Lead to local channels and collaterals obstruction, qi and blood stagnation and congestion, and by the cold or trauma induced by the disease.Therefore, for PS patients, simple analgesic treatment can only temporarily improve the clinical symptoms of patients, and cannot fundamentally solve the pain of patients.Traditional Chinese medicine treatment PS emphasizes to pay attention to the specimen,both internal and external treatment, treatment based on syndrome differentiation, should in the liver and kidney, tonifying qi and blood on the basis, dispel the wind and dehumidification, warm through the collaterals, promote blood circulation pain. A large number of clinical studies have shown that warm acupuncture can effectively relieve shoulder pain and improve shoulder joint mobility in the treatment of PS[1, 5, 10-12, 22, 24-26]. Similarly, a large number of clinical studies have shown that various massage techniques can dredge channels and collaterals, release adhesion, dredge joints and relieve pain through various techniques, which can effectively relieve shoulder joint pain, improve shoulder joint movement ability and promote rehabilitation of patients[4, 13, 14, 23, 27, 28].
On the basis of previous studies, this study combined warm acupuncture and massage therapy with massage manipulation,deeply explored the clinical efficacy of treating Periarthritis of Shoulder with warm acupuncture and massage alone and combined with warm acupuncture and massage manipulation, and compared the treatment scheme with ultra-short wave combined plaster external application.The study found that these treatment regimens could effectively reduce the use of ibuprofen sustained release capsules,reduce the VAS pain score and the Melle shoulder joint mobility limitation score, significantly improve the clinical symptoms of patients, and reduce the TCM symptom score of patients.In addition,these treatment regimens can effectively reduce the level of serum inflammatory factors and improve the microinflammatory state in patients, and the overall effect is between 76.67% and 96.67%.However, the combination of warm acupuncture and massage technique can more effectively alleviate the shoulder pain, movement disorders and other clinical symptoms of PS patients, further reduce the use of ibuprofen in PS patients compared with other groups,and reduce the VAS score and Melle score.This indicates that warm acupuncture combined with massage can further enhance the therapeutic effect of using warm acupuncture or massage alone,significantly improve the clinical symptoms of patients, increase the level of Shoulder joint activity, and reduce the serum inflammatory factor level of patients with Periarthritis of Shoulder, which has a good clinical effect.In conclusion, the combination of warm acupuncture and massage can significantly improve the clinical symptoms of PS patients and promote their recovery.Compared with physical therapy alone and the application of warm acupuncture or massage manipulation alone, the combined treatment of warm acupuncture and massage manipulation can better alleviate shoulder pain and improve the range of motion of shoulder joint, which is worthy of further promotion and application in clinical practice.
杂志排行
Journal of Hainan Medical College的其它文章
- Meta analysis and medication analysis of TCM compound in the treatment of senile osteoporosis
- The Effect of Clinically Used Crystalloid Solution on the Clearance Rate of Lactic Acid in Septic Shock Patients
- Efficacy of intravitreal injection of ranibizumab in the treatment of macular edema secondary to non-ischemic branch retinal vein occlusion
- Efficacy of PC-PRL implantation in the treatment of high myopia and its complications
- Expression and clinical significance of lncRNA SNHG3 in peripheral blood mononuclear cells of patients with chronic obstructive pulmonary disease
- Effects of Pioglitazone on Renal Mitochondrial calcium and cytochrome C levels in Early Diabetic Nephropathy Rats