低温等离子气化消融术诱发的颈椎盘源性疼痛分布规律分析
2019-10-30何亮亮倪家骧曹国庆郭玉娜杨立强
何亮亮 倪家骧 曹国庆 郭玉娜 杨立强
[摘要] 目的 通过低温等离子技术气化消融神经诱发疼痛的方法,探讨颈椎盘源性疼痛的分布规律。 方法 选择2018年6~11月首都医科大学宣武医院疼痛科行CT引导下低温等离子椎间盘气化消融术的30例颈椎盘源性疼痛患者作为研究对象。术中,采用人体数字编码区域示意图记录诱发疼痛区域。 结果 低温等离子气化消融术的椎间盘节段包括14例C4~C5、17例C5~C6和5例C6~C7,其中C4~C5、C5~C6和C6~C7间盘均可诱发的疼痛区域包括颈肩交界、斜方肌后上方、肩胛骨、肩胛间、胸前、肩后。C4~C5间盘诱发的疼痛区域偏向头侧,包括前额、耳、枕后、枕下、颈后区域;C5~C6间盘诱发的疼痛区域包括颈后、颈前、颈肩交界、斜方肌后上方、肩胛骨、肩胛间、胸前、肩后、上臂、前臂、胸背;C6~C7间盘诱发的疼痛区域偏向足侧,包括上臂、前臂、胸背区域。 结论 颈椎盘源性疼痛的分布呈一定规律分布,具有重叠性、局限性、方向性和顺序性。
[关键词] 低温等离子;颈椎盘源性疼痛;间盘造影;疼痛分布
[中图分类号] R681 [文献标识码] A [文章编号] 1673-7210(2019)08(a)-0119-04
[Abstract] Objective To investigate the distribution of cervical discogenic pain through the method of low-temperature plasma gasification ablation technology to induce pain. Methods From June to November 2018, 30 patients with cervical discogenic pain underwent CT-guided low-temperature plasma intervertebral disc gasification ablation in Department of Pain of Xuanwu Hospital, Capital Medical University were selected as research objects. During the operation, the pain-inducing region was recorded by the schematic diagram of the digital coding region of human body. Results The intervertebral disc segments of low-temperature plasma gasification ablation included 14 cases of C4-C5, 17 cases of C5-C6, and 5 cases of C6-C7, among which, the pain areas induced by C4-C5, C5-C6, and C6-C7 intervertebral disc included the cervical and shoulder junction, the posterior upper part of the trapquadratus, the scapula, the interscapula, the chest, and the posterior shoulder. The pain areas induced by C4-C5 intervertebral disc were inclined to the cephalic side, including the forehead, ears, posterior occipital, suboccipital and posterior cervical areas. The pain areas induced by C5-C6 intervertebral disc included posterior, anterior, cervico-shoulder junction, posterior and upper part of the trapezius, scapula, interscapula, chest, posterior shoulder, upper arm, forearm and thorax. The pain areas induced by C6-C7 intervertebral disc were inclined to the side of the foot, including the upper arm, forearm and thoracodorsal areas. Conclusion The distribution of cervical discogenic pain is regular, with overlap, limitation, direction and sequence.
[Key words] Low-temperature plasma; Cervical discogenic pain; Discography; Pain distribution
颈椎神经根性疼痛和颈椎盘源性疼痛被认为是颈椎间盘源性疼痛的两个重要临床表现[1-2]。颈椎神经根性疼痛与椎间盘突出压迫刺激神经根有关,其疼痛区域遵循神经根支配的分布规律;而颈椎盘源性疼痛与椎间盘内神经末梢受到盘内高压或化学性伤害刺激有关,其受刺激的病变神经是椎间盘内的神经末梢而非神经根,因此其疼痛分布不具有神经根性疼痛的体表分布规律[3-8]。由于,颈椎间盘MRI影像学特征与颈椎盘源性疼痛临床症状的相关性差[9-10],且颈椎盘源性疼痛分布规律与椎间盘的关系缺乏共识,常造成“责任间盘”的漏诊或误诊。因此,探讨颈椎盘源性疼痛的分布规律、提高责任间盘定位的准确性是提高手術疗效的关键问题。
低温等离子椎间盘气化消融术治疗颈椎盘源性疼痛的治疗机制与低温等离子气化消融盘内神经末梢有关,而气化消融神经末梢的直接表现就是诱发疼痛[12-13]。因此,通过观察记录低温等离子气化消融椎间盘内神经末梢而诱发的疼痛区域,可以为颈椎盘源性疼痛的分布规律获得直接的数据支持。本研究旨在利用低温等离子技术气化消融神经进而复制疼痛的方法,探讨颈椎盘源性疼痛的分布规律。
1 资料与方法
1.1 一般资料
本研究已获首都医科大学宣武医院(以下简称“我院”)医学伦理委员会批准,患者或其家属已签署知情同意书。2018年6~11月我院疼痛科进行颈椎低温等离子椎间盘气化消融术的颈椎间盘源性疼痛患者30例,ASAⅠ~Ⅱ级,男16例,女14例,年龄≥18岁,身高不限,体重不限,疼痛时间>3个月,疼痛视觉模拟评分(VAS)≥4分。经保守治疗、椎间孔或关节突关节注射治疗无效,MRI提示颈椎椎间盘包容性突出,突出<3 mm,突出节段≤2个,椎间盘高度>50%相邻椎间盘高度,排除感染、血液病、凝血功能异常、脊髓炎、脊髓栓系、脊髓肿瘤、椎体滑脱等。
1.2 方法
患者入手术室后,开放上肢静脉通道,以10 mL/(kg·h)速率输入乳酸钠林格液,术前静脉滴注阿托品0.5 mg。监测心率、血压、血氧饱和度(SpO2)。患者取仰卧位,颈肩部下垫1个10 cm高薄枕,保持颈椎轻度后仰位,颈前手术皮肤区域消毒、铺巾后,5 mL 0.5%利多卡因(生产商:山东华鲁制药有限公司;批号:C1806203)在颈前正中旁开1.5~2 cm处行局部浸润麻醉。患者保持清醒,术中出现诱发疼痛或异常神经刺激症状,应与术者及观察者准确沟通。首先,CT引导定位穿刺进针路径和角度,使用18G、8 cm穿刺针经左侧/右侧前入路至椎间盘,反复结合CT引导定位,再沿穿刺针内径置入等离子刀头(生产商:高通,中国;批号:1702181050),其刀头的工作端超出穿刺针尖端大约5 mm,再结合CT引导验证,确保等离子刀头不超过椎间盘后缘。位置无误后,启用热凝模式,工作强度1′,工作时间0.5~1 s,测试有无异常神经根刺激症状或异常感觉症状出现。启用消融模式,工作强度2′,顺时针旋转等离子刀头360°消融灭活纤维环内神经末梢,每次旋转工作时间<10 s,根据疼痛复制情况和椎间盘内压情况,酌情增加消融次数。
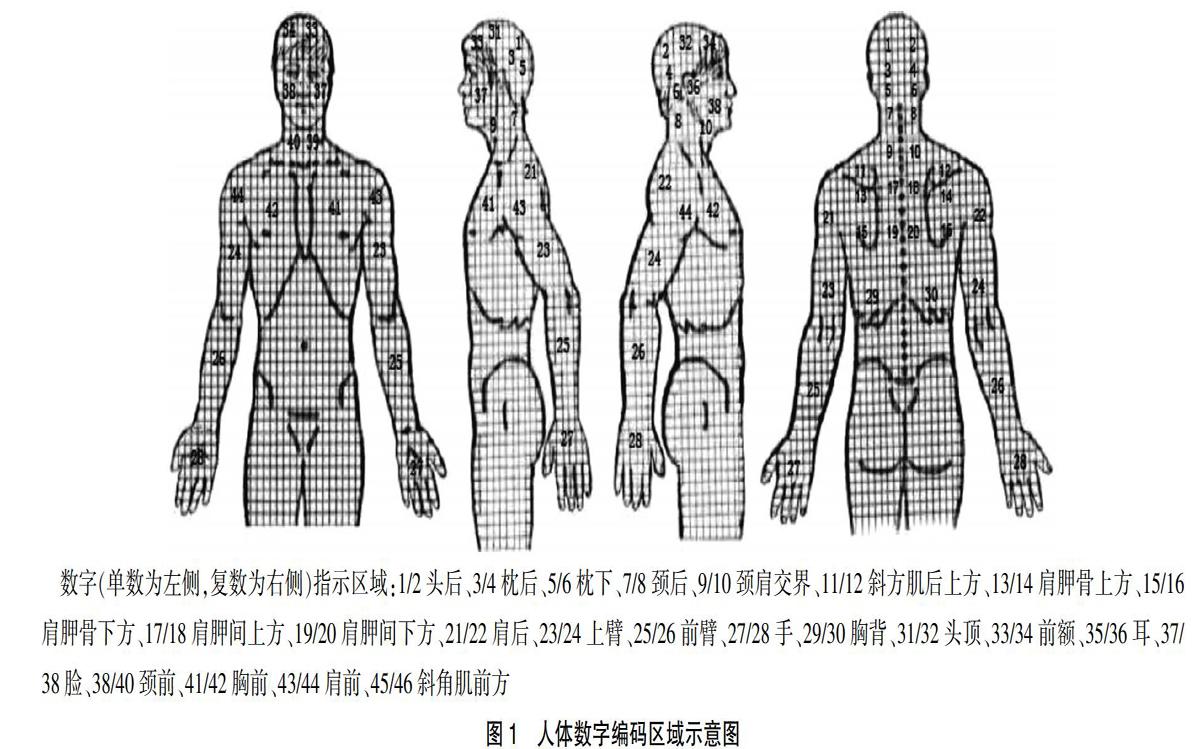
消融过程中,记录人询问患者诱发疼痛区域,在人体数字编码区域示意图中标记。同时记录术中低温等离子消融侧别、疼痛性质。如术中消融过程未诱发疼痛,则记录无。见图1。
2 结果
本研究中,共36个节段的椎间盘进行低温等离子气化消融术,术中均诱发疼痛。
男16例,女14例;年龄(53±11)岁;身高(169±7)cm;体重(68±9)kg;疼痛时间(28±23)个月;疼痛VAS评分(7.1±0.9)分。
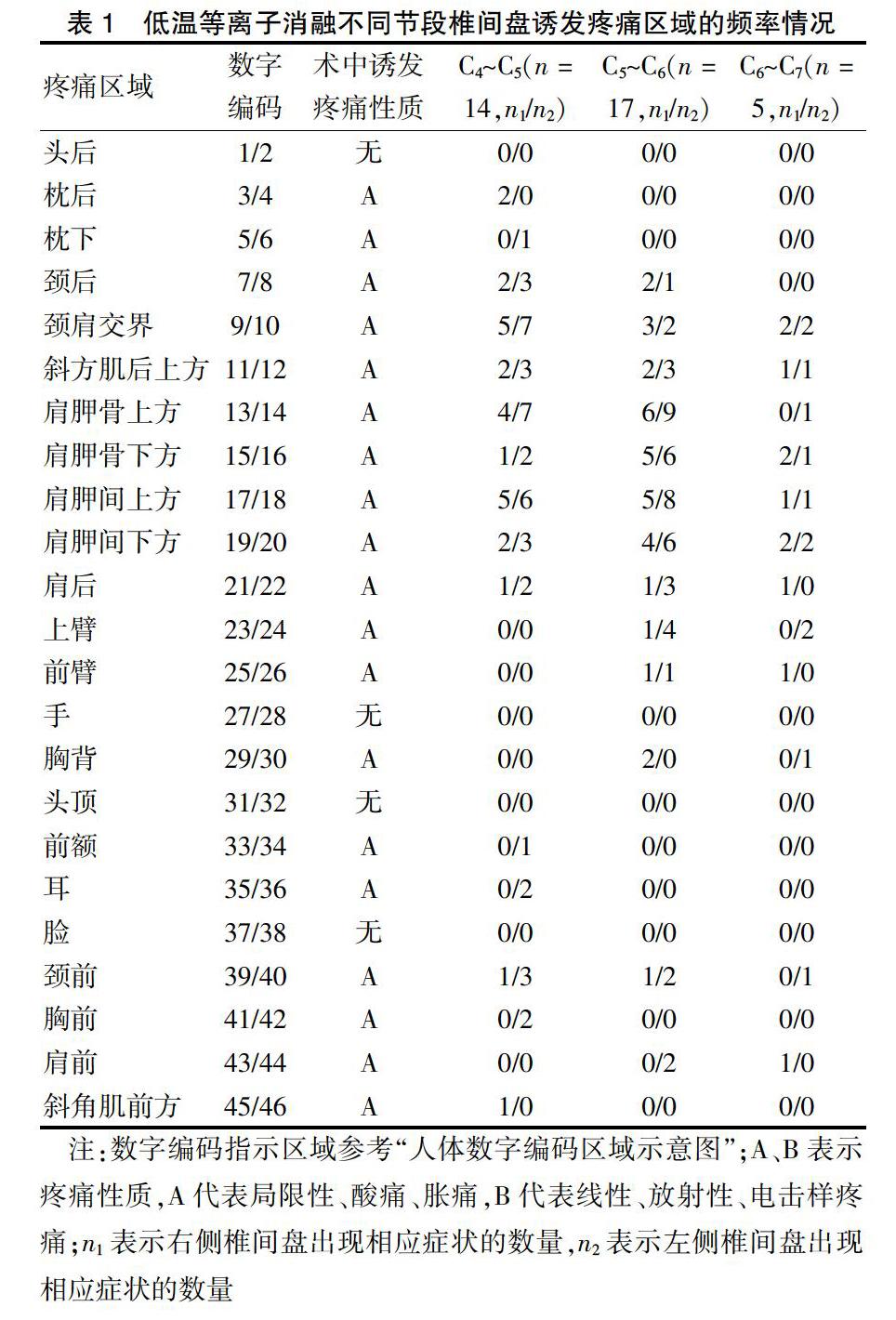
C4~C5、C5~C6和C6~C7椎间盘的例数分别是14、17、5例。14例C4~C5中,消融侧别是:左侧6例,右侧8例;17例C5~C6中,消融侧别是:左侧7例,右侧10例;5例C6~C7中,消融侧别是:左侧2例,右侧3例。其中,C4~C5诱发疼痛区域包括前额、耳、枕后、枕下、颈后、颈前、颈肩交界、斜方肌后上方、斜方肌后前方、肩胛骨、肩胛间、胸前、肩后(表1,图2A);C5~C6诱发疼痛区域包括颈后、颈前、颈肩交界、斜方肌后上方、肩胛骨、肩胛间、胸前、肩后、上臂、前臂、胸背(表1,图2B);C6~C7诱发疼痛区域包括颈肩交界、斜方肌后上方、肩胛骨、肩胛间、胸前、肩后、上臂、前臂、胸背(表1,图2C)。
3 讨论
本研究首次通过低温等离子消融颈椎间盘内神经诱发疼痛的方法,描述了颈椎盘源性疼痛区域的分布情况。研究结果提示,从C4~C5到C6~C7诱发疼痛区域包括前额、耳、枕后、枕下、颈后、颈前、颈肩交界、斜方肌后上方、斜方肌后上方、肩胛骨、肩胛间、胸前、肩后、上臂、前臂、胸背等区域,疼痛区域呈现出局限性、重叠性、方向性和顺序性的分布规律。
本研究结果提示,颈椎盘源性疼痛区域具有局限性分布的特点。36例颈椎间盘诱发疼痛区域以轴性疼痛区域分布为主,除3例椎间盘诱发疼痛区域牵涉至前臂,其余均未超过肘关节。研究结果与Cloward[5]进行颈椎间盘造影术发现的结果一致,颈椎盘源性疼痛大多数疼痛并未放射至肘关节以下,几乎很少患者主诉疼痛或异常感觉可放射至手或手指。
本研究结果提示,颈椎盘源性疼痛区域具有重叠性分布的特点。36例颈椎间盘诱发疼痛区域以颈肩交界、肩胛骨、肩胛间分布为主,其中C4~C5到C6~C7诱发疼痛区域包括颈肩交界、斜方肌后上方、肩胛骨、肩胛间、胸前、肩后,C5~C6到C6~C7诱发疼痛区域包括上臂、前臂、胸背区域。与Grubb等[14]、Slipman等[15]研究结果相似,C4~C5、C5~C6、C6~C7均可诱发肩胛骨、肩胛间区域的的疼痛症状。其机制可能与多个椎间盘同时接受来自同一水平节段的窦椎神经、前支、交通支、交感干发出的神经纤维支配有关[16]。
本研究结果提示,颈椎盘源性疼痛区域具有方向性分布的特点。36例颈椎间盘低温等离子气化消融期间,消融左侧诱发疼痛区域在左侧,消融右侧诱发疼痛区域在右侧,其诱发疼痛区域与消融侧别一致。另外,由内侧向外侧改变消融靶点方向,其诱发疼痛区域也呈现由内向外的改变趋势。Cloward[5]报道了类似现象,在刺激颈椎椎间盘正中线时,疼痛位于椎体正中线处,而刺激点偏向外侧2~3 mm时,疼痛位置则转移至同侧肩胛区域,提示盘源性疼痛区域与椎间盘的病变位置有关。
本研究结果提示,颈椎盘源性疼痛区域具有顺序性分布的特点。尽管,36例颈椎间盘诱发疼痛区域具有明显的重叠性,但不同节段椎间盘诱发的疼痛区域仍然存在部分未重叠现象。与颈椎间盘造影的研究结果一致[17],高节段椎间盘诱发疼痛区域偏向头侧,低节段椎间盘诱发疼痛区域偏向尾侧,提示颈椎盘源性疼痛分布区域与椎间盤位置的高低顺序有关。
本研究提示,在椎间盘气化消融过程中出现上肢跳动现象,但无疼痛反应。此现象可能与感觉-运动反射有关[17]:即刺激支配椎间盘内部窦椎神经末梢后,伤害性感受信号沿窦椎神经进入背根神经节,传递至脊髓背角,通过局部神经反射,激活脊髓前角诱发运动神经支配区域肌肉收缩痉挛,出现肌肉跳动现象。判断是否损伤神经根,主要依据4点:①CT验证刀头位置;②是否是线性、放射样疼痛性质;③是否出现麻木、感觉缺失等异常现象;④是否出现肌力减退。
综上所述,本研究通过低温等离子技术气化消融神经诱发疼痛的方法,发现颈椎盘源性疼痛区域呈局限性、重叠性、方向性和顺序性的分布规律。
[参考文献]
[1] Manchikanti L,Soin A,Benyamin RM,et al. An Update of the Systematic Appraisal of the Accuracy and Utility of Discography in Chronic Spinal Pain [J]. Pain Physician,2018,21(2):91-110.
[2] Benditz A,Brunner M,Zeman F,et al. Effectiveness of a multimodal pain management concept for patients with cervical radiculopathy with focus on cervical epidural injections [J]. Sci Rep,2017,7(1):7866.
[3] Peng B,DePalma MJ. Cervical disc degeneration and neck pain [J]. J Pain Res,2018,14(11):2853-2857.
[4] Cohen SP,Hooten WM. Advances in the diagnosis and management of neck pain [J]. BMJ,2017,358:j3221.
[5] Cloward RB. Cervical discography:A contribution to the etiologu and mechanism of neck,shoulder and arm pain [J]. Ann Srug,1959,150(6):1052-1064.
[6] Evans G. Identifying and treating the causes of neck pain [J]. Med Clin North Am,2014,98(3):645-661.
[7] Yin W,Bogduk N. The nature of neck pain in a private pain clinic in the United States [J]. Pain Med,2008,9(2):196-203.
[8] Sainoh T,Sakuma Y,Miyagi M,et al. Efficacy of anti-nerve growth factor therapy for discogenic neck pain in rats [J]. Spine,2014,39(13):e757-e762.
[9] Onyewu O,Manchikanti L,Falco FJ,et al. An update of the appraisal of the accuracy and utility of cervical discography in chronic neck pain [J]. Pain Physician,2012,15(6):e777-e806.
[10] Nystr?觟m B,Weber H,Schillberg B,et al. Symptoms and signs possibly indicating segmental, discogenic pain. A fusion study with 18 years of follow-up [J]. Scand J Pain,2017,16:213-220.
[11] Sim SE,Ko ES,Kim DK,et al. The results of cervical nucleoplasty in patients with cervical disorder:a retrospective clinical study of 22 patients [J]. Korean J Pain,2011,24(1):36-43.
[12] He L,Yang L,Wu B,et al. Efficacy of coblation annuloplasty combined with nucleoplasty in cervical discogenic and radicular pain [J]. Int J Clin Exp Med,2017,10(2):3147-3154.
[13] He L,Tang Y,Li X,et al. Efficacy of coblation technology in treating cervical discogenic upper back pain [J]. Medicine(Baltimore),2015,94(20):e858.
[14] Grubb SA,Kelly CK. Cervical discography:Clinical implications from 12 years of experience [J]. Spine(Phila Pa 1976),2000,25(11):1382-1389.
[15] Slipman CW,Plastaras C,Patel R,et al. Provocative cervical discography symptom mapping [J]. Spine J,2005,5(4):381-388.
[16] Fujimoto K,Miyagi M,Ishikawa T,et al. Sensory and autonomic innervation of the cervical intervertebral disc in rats: the pathomechanics of chronic discogenic neck pain [J]. Spine(Phila Pa 1976),2012,37(16):1357-1362.
[17] Cloward RB. The clinical significance of the sinu-vertebral nerve of the cervical spine in relation to the cervical disk syndrome [J]. J Neurol Neurosurg Psychiatry,1960, 23:321-326.
(收稿日期:2018-12-03 本文編辑:张瑜杰)
