Evaluation and comparison of short chain fatty acids composition in gut diseases
2019-10-28ElenaNiccolaiSimoneBaldiFedericaRicciEddaRussoGiuliaNanniniMartaMenicattiGiovanniPoliAntonioTaddeiGianlucaBartolucciAntoninoSalvatoreCalabrFrancescoClaudioStingoAmedeoAmedei
Elena Niccolai, Simone Baldi, Federica Ricci, Edda Russo, Giulia Nannini, Marta Menicatti, Giovanni Poli,Antonio Taddei, Gianluca Bartolucci, Antonino Salvatore Calabrò, Francesco Claudio Stingo, Amedeo Amedei
Abstract BACKGROUND An altered (dysbiosis) and unhealthy status of the gut microbiota is usually responsible for a reduction of short chain fatty acids (SCFAs) concentration.SCFAs obtained from the carbohydrate fermentation processes are crucial in maintaining gut homeostasis and their determination in stool samples could provide a faster, reliable and cheaper method to highlight the presence of an intestinal dysbiosis and a biomarker for various gut diseases. We hypothesize that different intestinal diseases, such as celiac disease (CD), adenomatous polyposis (AP) and colorectal cancer (CRC) could display a particular fecal SCFAs' signature.AIM To compare the fecal SCFAs' profiles of CD, AP, CRC patients and healthy controls, using the same analytical method.METHODS In this cross-sectional study, we defined and compared the SCFAs' concentration in fecal samples of 9 AP, 16 CD, 19 CRC patients and 16 healthy controls (HC).The SCFAs' analysis were performed using a gas-chromatography coupled with mass spectrometry method. Data analysis was carried out using Wilcoxon ranksum test to assess pairwise differences of SCFAs' profiles, partial least squaresdiscriminate analysis (PLS-DA) to determine the status membership based on distinct SCFAs' profiles, and Dirichlet regression to determine factors influencing concentration levels of SCFAs.RESULTS We have not observed any difference in the SCFAs' amount and composition between CD and healthy control. On the contrary, the total amount of SCFAs was significantly lower in CRC patients compared to HC (P = 0.044) and CD (P =0.005). Moreover, the SCFAs' percentage composition was different in CRC and AP compared to HC. In detail, HC displayed higher percentage of acetic acid (P value = 1.3 × 10-6) and a lower amount of butyric (P value = 0.02192), isobutyric (P value = 7.4 × 10-5), isovaleric (P value = 0.00012) and valeric (P value = 0.00014)acids compared to CRC patients. AP showed a lower abundance of acetic acid (P value = 0.00062) and higher percentages of propionic (P value = 0.00433) and isovaleric (P value = 0.00433) acids compared to HC. Moreover, AP showed higher levels of propionic acid (P value = 0.03251) and a lower level of isobutyric acid (P value = 0.00427) in comparison to CRC. The PLS-DA model demonstrated a significant separation of CRC and AP groups from HC, although some degree of overlap was observed between CRC and AP.CONCLUSION Analysis of fecal SCFAs shows the potential to provide a non-invasive means of diagnosis to detect patients with CRC and AP, while CD patients cannot be discriminated from healthy subjects.
Key words: Short chain fatty acids; Microbiota; Colorectal cancer; Adenoma; Celiac disease
INTRODUCTION
Nowadays, it is well known that multiple factors can alter the normal composition of the gut microbiota (GM) favoring the onset of intestinal diseases, such as inflammatory bowel disease (IBD), celiac disease and colorectal cancer (CRC)[1-3]. The diet represents one of the main documented element responsible for changes in the structural and functional relationship between gut microbiota and the host[4]. The fermentative bacterial metabolism of dietary components, especially indigestible fibers, produces a large amount of biologically active compounds such as short chain fatty acids (SCFAs)[5-7]. SCFAs are saturated fatty acids composed by one to six carbons of which acetic (C2), propionic (C3), and butyric (C4) are in the largest quantity[8,9]with a generally constant respective molecular ratio of 60:20:20 in the colon as well as in the feces[10]. Beside these, other SCFAs, as iso-Butyric (C4), valeric (C5)and iso-Valeric (C5), are present in lower amounts. They can be absorbed by the colonic epithelium providing energy or enter the bloodstream playing a relevant role in the regulation of the metabolism of fatty acids, glucose, and cholesterol[11-14].Moreover, thanks to their ability to induce the production of antimicrobial peptides and to modulate the number and functions of Regulatory T cells (Tregs), SCFAs contribute to the modulation of host immune responses[15-17]. An unhealthy GM status is responsible for a reduction of SCFAs' concentration, which is essential for the host in order to prevent intestinal diseases[18]. In fact, they preserve the epithelial barrier functionality and contrast the onset of inflammatory reactions by the transcriptional regulation of tight junction proteins, particularly the claudin-1[19]. In addition, the SCFAs sustain the proliferation and differentiation of colonocytes and protect colonic epithelium by increasing the expression of mucin 2 and modulating both oxidative stress and immune response[20]. Different studies have well documented an alteration in SCFAs' composition in some human pathologies, such as IBD[8], irritable bowel syndrome[21], diarrhea[22]and cancer[23]and for this reason, they represent a target to measure intestinal health and have been proposed as potential diagnostic biomarkers[24]. Moreover, the SCFAs' evaluation in stool samples could provide a faster, reliable and cheaper method to highlight the presence of an intestinal dysbiosis instead of the microbiota characterization. Besides, genomics approaches cannot shed light on real fermentation processes and functional microbiota changes (metabolite production). Anyway, the high variability in protocols and analytical methods (i.e.,capillary electrophoresis, chromatography, nuclear magnetic resonance) for the SCFAs' determination[25], make difficult to compare literature data and bringing out real differences in SCFAs' profiles of the various intestinal diseases.
The principal objective of the research was to compare the fecal SCFAs' profile of patients with different intestinal diseases, in detail adenomatous polyposis (AP),celiac disease (CD) and CRC, to healthy controls (HC), applying the same protocols and analytical conditions gas chromatography-mass spectrometry (GC-MS) for their evaluation in order to point out whether these pathologies displayed a particular fecal SCFAs signature.
MATERIALS AND METHODS
Study design and biological samples
In this cross-sectional study, we used the biological samples of 44 patients with different gut diseases (19 patients with CRC, 9 patients with AP, 16 patients with CD)and 16 healthy controls, collected for different studies between January 2016 and February 2019 at the Careggi Hospital and University of Florence, Italy. All patients'fecal samples were taken at diagnosis, before starting any treatment (i.e., surgical resection, chemotherapy, gluten-free diet). All patients were on an omnivorous diet and none of them reported special dietary habits or dietary restrictions. Moreover,any one reported antibiotic drugs or probiotic/prebiotic products intake during the last 3 mo. Clinical characteristics of patients are shown in Table 1. The study has received the local Ethics Committee approval (CE: 11166_spe and CE: 10443_oss) and an informed written consent has been obtained from each participant.
Instrumental and chemicals
The SCFAs' analysis was performed by Agilent GC-MS system composed with 5971 single quadrupole mass spectrometer, 5890 gas-chromatograph and 7673 autosampler. Methanol and tert-Butyl methyl ether (Chromasolv grade), Sodium bicarbonate and Hydrochloric acid (Reagent grade), [2H3]Acetic, [2H3]Propionic,[2H7]iso-Butyric and [2H9]iso-Valeric, used as internal standards (ISTDs), acetic acid,propionic acid, butyric acid, isobutyric acid, valeric acid and isovaleric acid (analytical standards grade) were purchased by Sigma-Aldrich (Milan, Italy). MilliQ water 18 MΩ was obtained from Millipore's Simplicity system (Milan, Italy).
GC-MS method
The SCFAs in the samples were analyzed as free acid form using a Supelco Nukol column 30 m length, 0.25 mm internal diameter and 0.25 μm of film thickness with the temperatures program as follows: Initial temperature of 40 °C was held for 1 min,then it was increased to 150 °C at 30 °C/min, finally grow up to 220 °C at 20°C/min[26]. A 1 μL aliquot of extracted sample was injected in splitless mode (splitless time 1 min) at 250 °C, while the transfer line temperature was 280 °C. The used carriergas was helium and its flow rate maintained at 1 mL/min for whole run time. The MS acquisition was carried out in single ion monitoring by apply a proper dwell time (20 ms for each ion monitored) to guarantee a detection frequency of 4 cycle/s.

Table 1 Clinical characteristics of patients
The quantitative determination of SCFAs in each sample was carried out by the ratio between the area abundance of the analytes with the area abundance of respective labeled internal standard (isotopic dilution method). The value of this ratio was named peak area ratio (PAR) and it was used as abundance of each analyte in the quantitative evaluation. The ionic signals of SCFAs' and the reference internal standards used for the quantitation of each SCFAs were reported in the Table 2.
Standard solutions and calibration curves
The stock solutions of each analyte and each ISTDs were prepared in mQ water at 50 mg/mL and stored at 4 °C. Since the quantity of each SCFA in the samples could be different, different concentration ranges of each analyte were defined. Therefore, to easily build up these calibration levels, two working mixtures of analytes (Mix 1 and Mix 2) and a mixture of ISTDs in 10 mM NaHCO3solution were prepared. The compositions and the concentrations of these mixtures are reported in the Table 3.
A five levels calibration curve was prepared by adding proper volumes of Mix 1 or 2 solution, 50 μL of ISTDs mixture, 1 mL of tert-butyl methyl ether and 50 μL of 1.0 mol/L HCl solution in microcentrifuge tube. Then, each tube was shaken in vortex apparatus for 2 min, centrifuged at 10000 rpm for 5 min, and finally the solvent layer was transferred in autosampler vial and analyzed three times by GC-MS method.Final concentrations of calibration levels are shown in the Table 4.
Sample preparation
Fecal samples were collected in 15 mL falcon tubes and stored at -80 °C. Just before the analysis, each sample was thawed, weighted (between 0.5-1.0 g) and added of sodium bicarbonate 10mM solution (1:1 w/v) in a 1.5 mL centrifuge tube. The obtained suspension was briefly stirred in vortex apparatus, extracted in ultrasonic bath (for 5 min) and then centrifuged at 5000 rpm (for 10 min). The supernatant was collected and transferred in 1.5 mL centrifuge tube (sample solution). The SCFAs were finally extracted as follow: An aliquot of 100 μL of sample solution (corresponding to 0.1 mg of stool sample) was added of 50 μL of ISTDs mixture, 1 mL of tert-butyl methyl ether and 50 μL of 1.0 M HCl solution in 1.5 mL centrifuge tube. Afterwards,each tube was shaken in vortex apparatus for 2 min, centrifuged at 10000 rpm for 5 min, and finally the solvent layer was trasferred in autosampler vial and analyzed by GC-MS method. Each samples were prepared and processed, by the method described above, three times.
Calibration curves
Calibration curves of analytes were obtained by plotting the PAR, between quantitation ions of each analyte and relative ISTD, vs the nominal concentration of the calibration solution. A linear regression analysis was applied to obtain the best fitting function between the calibration points.
In order to obtain reliable limit of detection (LOD) and limit of quantitation values,the standard deviation of response and slope approach was employed. The estimated standard deviations of responses of each analyte were obtained by the calculated standard deviation of y-intercepts of regression lines. The obtained linear regressions coefficients, the r-squared and the estimated LOD values for each analyte are reported
in the Table 5.
Statistical analysis
Statistical analysis on the SCFAs' composition were implemented in R (version 3.5.3,2019-03-11) and all the graphs were plotted with ggplot2 (v. 3.1.1). Pairwise differences in SCFAs' composition, between patient groups defined by state, wereassessed using Wilcoxon rank-sum test.
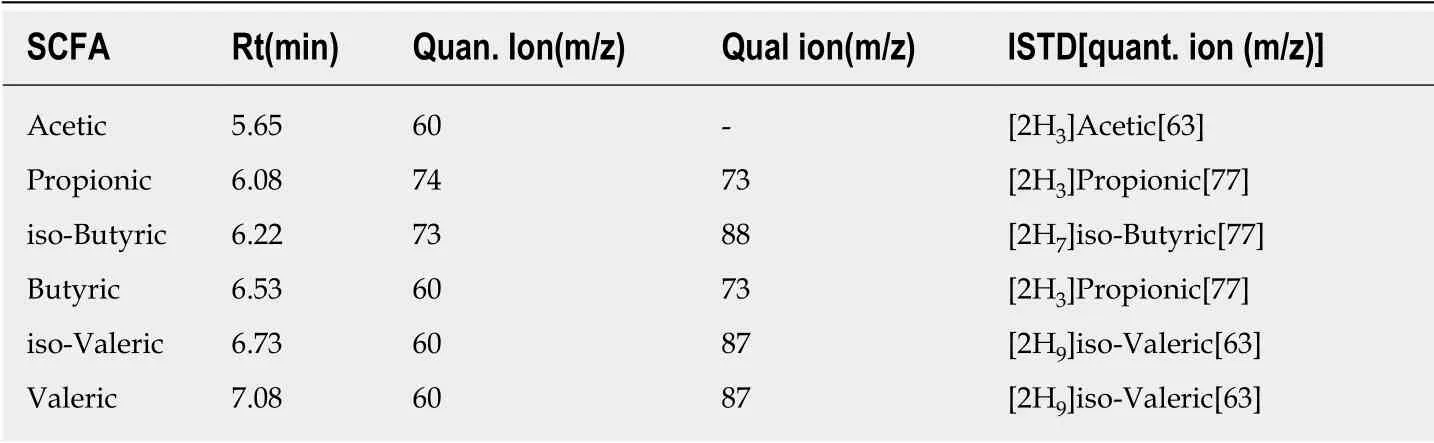
Table 2 Retention times, ionic signals, internal standards for each short chain fatty acid
A partial least squares discriminant analysis (PLS-DA) was performed with R package “DiscrMiner” (v. 0.1-29) in order to sharpen the separation between groups(States) of the diverse SCFA's percentages composition. Dirichlet regression was estimated with the package “DirichletReg” (v. 0.6-3.1) in order to assess which factors influence SCFAs' concentration levels, accounting for gender and age. P values of less than 0.05 were considered statically significant, no multiplicity correction was applied and findings are interpreted as hypothesis generating.
RESULTS
Pairwise comparisons: Pre-neoplastic and neoplastic diseases show a distinct SCFAs' profile
The concentration of SCFAs (μmol/g) was not significantly different in stools of CD and AP patients compared to HC. On the contrary, the total amount of SCFAs was significantly lower in CRC patients compared to HC (P = 0.044) and CD (P = 0.005)(Table 6). In detail, CRC patients showed lower concentration of acetic acid compared to CD patients and HC (P < 0.001). Since the previous results may be influenced by the total amount of SCFAs' concentration level, we have repeated the same comparisons on the SCFAs' percentage compositions: HC and CD shared a similar profile, which was different in comparison to CRC and AP patients (Figure 1).
In detail, the percentage of each SCFA did not differ between HC and CD (Figure 2), but changed in CRC and AP patients compared to HC. In particular, HC displayed a higher percentage of acetic acid (P value = 1.3 × 10-6) and a lower amount of butyric(P value = 0.02192), isobutyric (P value = 7.4 × 10-5), isovaleric (P value = 0.00012) and valeric (P value = 0.00014) acids compared to CRC patients. Regarding AP patients,they showed a lower abundance of acetic acid (P value = 0.00062) and higher percentages of propionic (P value = 0.00433) and isovaleric (P value = 0.00433) acids compared to HC. Moreover, AP showed higher levels of propionic acid (P value =0.03251) and a lower level of isobutyric acid (P value = 0.00427) in comparison to CRC.
Characterization of state specific SCFAs' profile
The PLS-DA model performed on the SCFAs' percentages matrix, confirmed that an almost perfect overlap of HC and CD patients groups exists, while CRC and AP patients showed a separation from the other two groups and were not coinciding(Figure 3). Anyway, along the first component, two CRC patients and two AP patients were included in the HC and CD patients groups.
Dirichlet's regression
Since the confounding effects of age and sex differences between groups of patients,cannot be excluded, the covariates of sex, age and status were tested using Dirichlet regression.The Dirichlet regression was estimated with sex, age and unhealthy status as covariates and the assigned baseline was the healthy status. As reported in Table 7,in the new model the difference between HC and CD patients wasn't relevant in any regression on SCFAs. The coefficient of CRC and AP were statistically significant (or close to 0.05 significance level) for acetic, propionic and butyric acids. The covariates effect in a Dirichlet regression can be investigated looking at the plots of the SCFAs'percentages expected values (Figure 4). The Dirichlet's model shows that HC and CD patients have a higher percentage of acetic acid and lower levels of the other SCFAs than CRC and AP patients. The effect of age on the levels of the acetic acid isstatistically significant, although the expected values curves have slopes of small magnitude. In particular, with the increasing age of CRC, AP, CD patients and HC occurs a reduction of acetic, propionic and valeric acids percentages, while the butyric, isobutyric and isovaleric acids percentages increase.
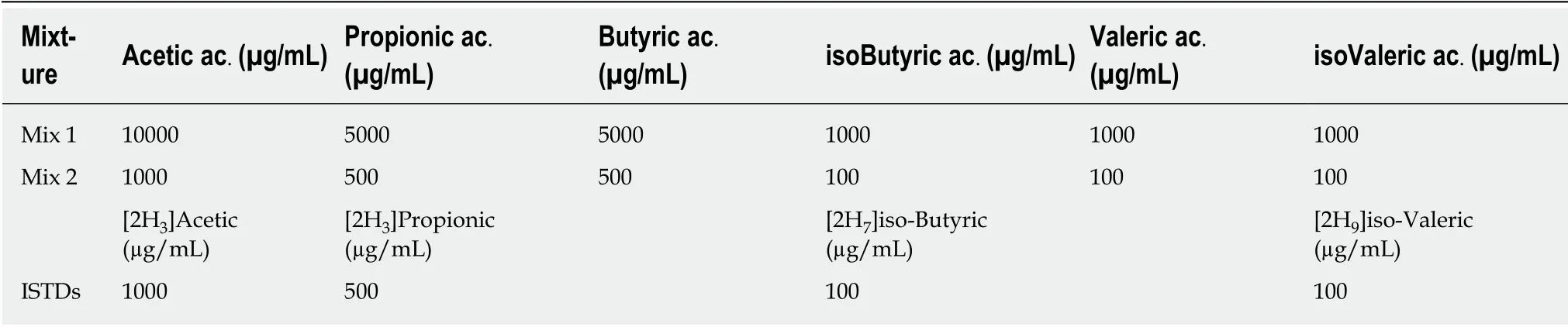
Table 3 Compositions and concentrations of standard and internal standards mixtures
DISCUSSION
In this study, we evaluated the fecal SCFAs' profiles (in term of quality and quantity)of patients with different intestinal diseases, namely colorectal cancer, adenoma and celiac disease, using gas-chromatography coupled with mass spectrometry. The study of SCFAs by GC-MS could represent an innovative way to discover non-invasive biomarkers of a disorder. Changing of the metabolic content of various human body fluids has been yet proposed for the diagnosis of different pathological conditions and for shedding light on their pathogenic mechanisms. Indeed, alteration of the fecal metabolites patterns in patients with different pathologies, such as inflammatory bowel diseases, preterm infants with necrotising enterocolitis, children with celiac disease, and obese patients with non-alcoholic fatty liver disease has been previously demonstrated[27-30]. Generally, SCFAs are reduced in dysbiotic conditions[31]. In fact,changes in the microbiota of patients with various disease have been linked with decreased bacterial diversity and fecal quantities of SCFAs (for example for the loss of butyrogenic gut bacteria such as F. prausnitzii)[32-34].
In recent years, various strategies have been applied to detect SCFAs in biological specimens, enclosing high performance liquid chromatography[35], electrochemical detection[36], mass spectrometry (MS)[37], gas chromatography (GC)[38]and capillary electrophoresis[39]. However, owing to SCFAs' chemical properties (i.e., volatility) and the advantages of the detectors that can be associated to these instruments, the GCMS is the most frequently used analytical technique. Moreover, the GC-MS system take the advantages of the isotopic dilution method in quantitative evaluation. In fact,this method employs an isotopologue of the analyte as internal standard, providing specificity, accuracy and robustness to the obtained quantitative data.
Our data documented a significant reduction of total SCFAs in stool samples of CRC patients compared with HC. In addition, the total amount of SCFAs in adenoma patients tend to be lower compared to healthy subjects even if not significantly.SCFAs, generated by the intestinal microbiota from the metabolism of undigested carbohydrates, are fundamental in keeping up the colonic mucosa wellbeing. An alteration in the fecal SCFAs' profile may be the result of gut microbiota dysbiosis,inflammatory changes or both. The literature data regarding the fecal SCFAs'composition in patients with the above mentioned gut diseases (CRC, AP) show a large discrepancy in the results[36-39]. In line with our data, various studies have demonstrated a decreased production of SCFAs in CRC patients compared to non-CRC[40,41]. But others authors have observed a higher amount of fecal acetic acid and a lower amount of fecal butyric acid in CRC patients compared to healthy individuals[42,43]. Butyric acid, produced by anaerobic bacterial fermentation of dietary fiber, has important homeostatic functions in human colon and it has been demonstrated, both in vivo and in vitro, to be important in the prevention of colon cancer[44-46]. Some reasons of the anticancer effect include its impact on genetic/epigenetic modulation, signaling pathways and immune response[44,46]. For example,butyric acid is able to increase the Tregs' number, resulting in decreased inflammation[47].
Although our study confirmed the reduction of the SCFAs amount in CRC, we have shown a lower relative concentration of fecal acetic acid and higher relative concentrations of butyric, isobutyric, valeric and isovaleric acids in CRC patientscompared to healthy controls. This is interesting because, even if a butyrate insufficiency has been usually implicated in cancer development[48,49], butyrate is also able to stimulate the proliferation of colon epithelial cells, and depending on its concentration, lead to cancer development, suggesting a double-edged role (“butyrate paradox”)[50]. Moreover, its ability to suppress inflammation by promoting Tregs'differentation, could be no longer protective in the end stages of cancer, since the Tregs can be co-opted by tumors assuming a pro tumorigenic role and so, favoring the tumor immunoescape[51]. Interestingly, the higher amount of butyric acid in CRC patients could depend also by the fact that cancerous colonocytes prefer the glucose utilization as primary energy source instead of oxidize butyrate and recently, Anna Han and coll. have demonstrated that butyrate decreased its own oxidation in cancerous colonocytes[52].
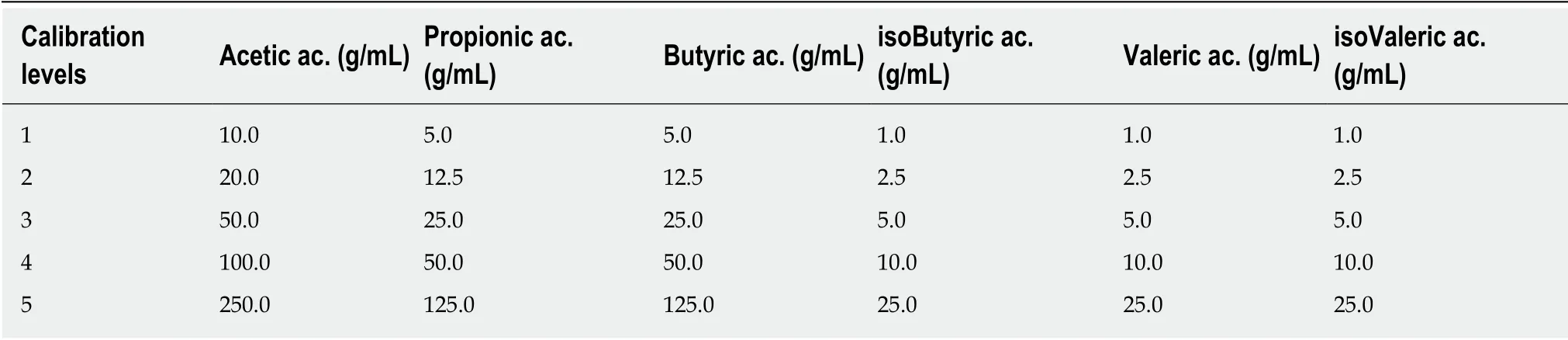
Table 4 Concentrations of each analyte in the calibration levels
According to our findings, a recent study demonstrated that patients with CRC and adenoma have lower concentration of total organic acids and acetic acid, and that adenoma patients show a SCFAs' profile intermediate to the CRC and the nonadenoma subjects[41]. We have demonstrated that the total amount and the relative percentage of all the examined SCFAs (with the exception of propionic acid) in adenoma group is intermediate to the CRC patients and HC. Moreover, the PLS-DA model performed on the SCFAs' percentages matrix, confirmed that CRC and AP patients showed a distinct separation from the healthy subjects and were not coinciding. Of note, the existence of a distinct and intermediate SCFAs' profile in AP compared to CRC and HC sustain the theory that the CRC develops in an intestinal environment that has already changed instead of being the tumor progression that modifies the local environment[43]. Besides, the presence of a distinct fecal SCFAs'profile both in AP and CRC patients, make the analysis of the fecal SCFAs composition a reliable biomarker for the disease detection.
Otherwise, the total amount of SCFAs in CD patients tend to be higher compared to HC, even not significantly. Accordingly, previous works found that SCFAs in untreated and trated CD patients were more copious than in healthy adults[53,54].Anyway, our study did not find a significant separation between CD patients and healthy controls, with no compositional differences in the levels of SCFAs. This is in contrast with previous data that showed a different SCFAs' profile in celiac patients[2,55], even if those findings often regard pediatric patients, with a significant difference in age compared to our CD group[55]. After all, as we demonstrated, the age significantly affects the composition of SCFAs, thus explaining the contrasting results present in literature. Even so, the Dirichlet regression model clearly demonstrated that differences in state specific SCFAs' profiles stand after accounting for the potential confounding effect of sex and age; particularly, we observed strong differences of the concentration levels of acetic acid, and relevant differences of concentration levels of propionic and butyric acid.
In conclusion, the small sample size of study does not allow us to reach definitive conclusions and our findings remain exploratory but we has clearly shown the existence of a fecal SCFAs fingerprint in patients with CRC, with a clear separation(with significant qualitative and quantitative differences) in the SCFAs' composition compared to healthy control. In addition, AP patients have showed a characteristic SCFAs' profile, distinguishable from CRC and healthy subjects. On the contrary, no separation between celiac patients and healthy controls was obtained regarding the SCFAs' composition profile. Finally, the fecal SCFAs' analysis through GC-MS could be considered as noninvasive and reliable diagnostic marker for the detection of adenoma and CRC patients.
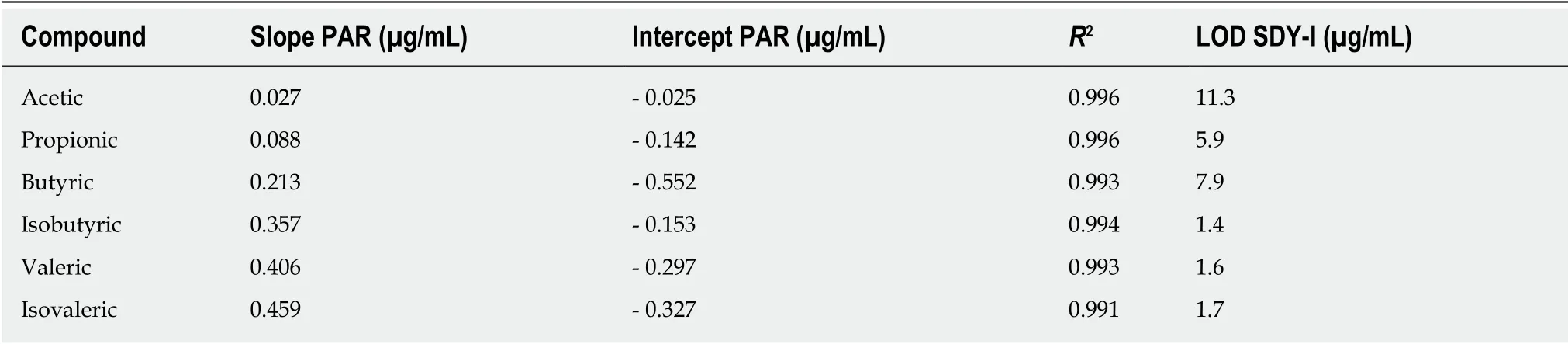
Table 5 Linear regressions data, R-squared and limit of detection values obtained for each analyte
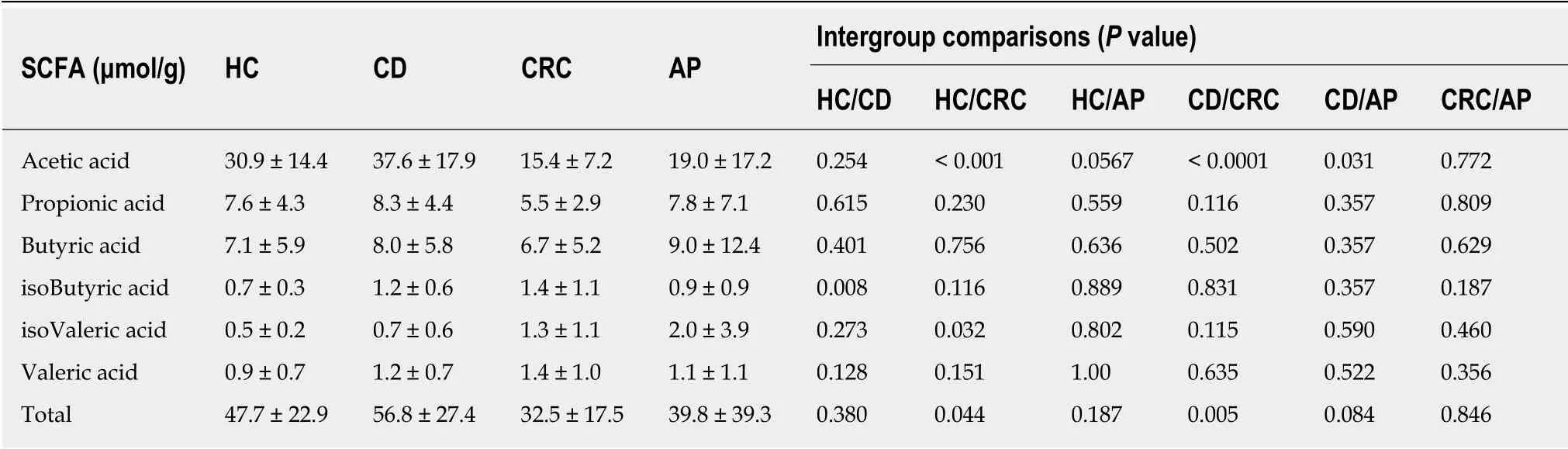
Table 6 Median ± standard deviation of each short chain fatty acid' concentration (μmol/g) in patients and healthy controls
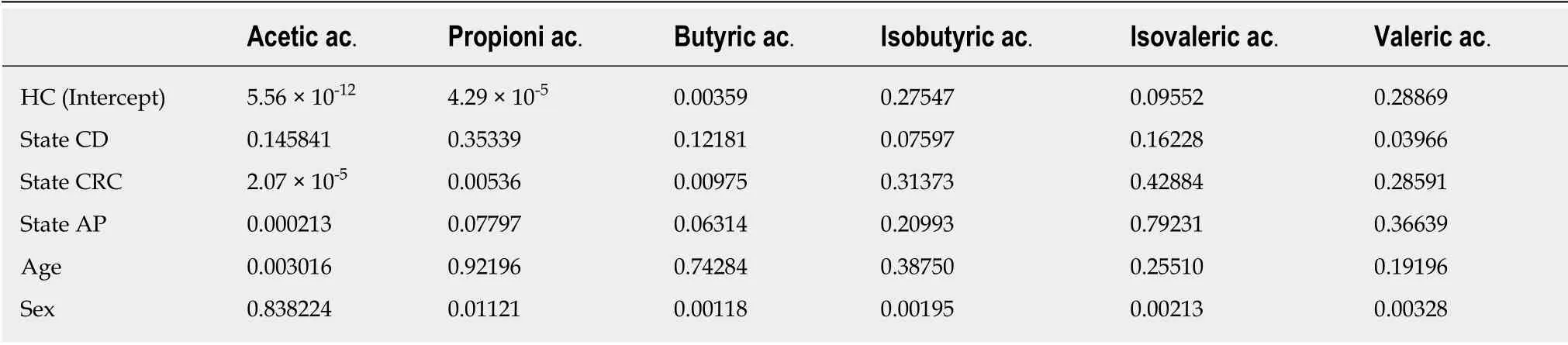
Table 7 P values of the Wald test conducted on the Dirichlet regression coefficients
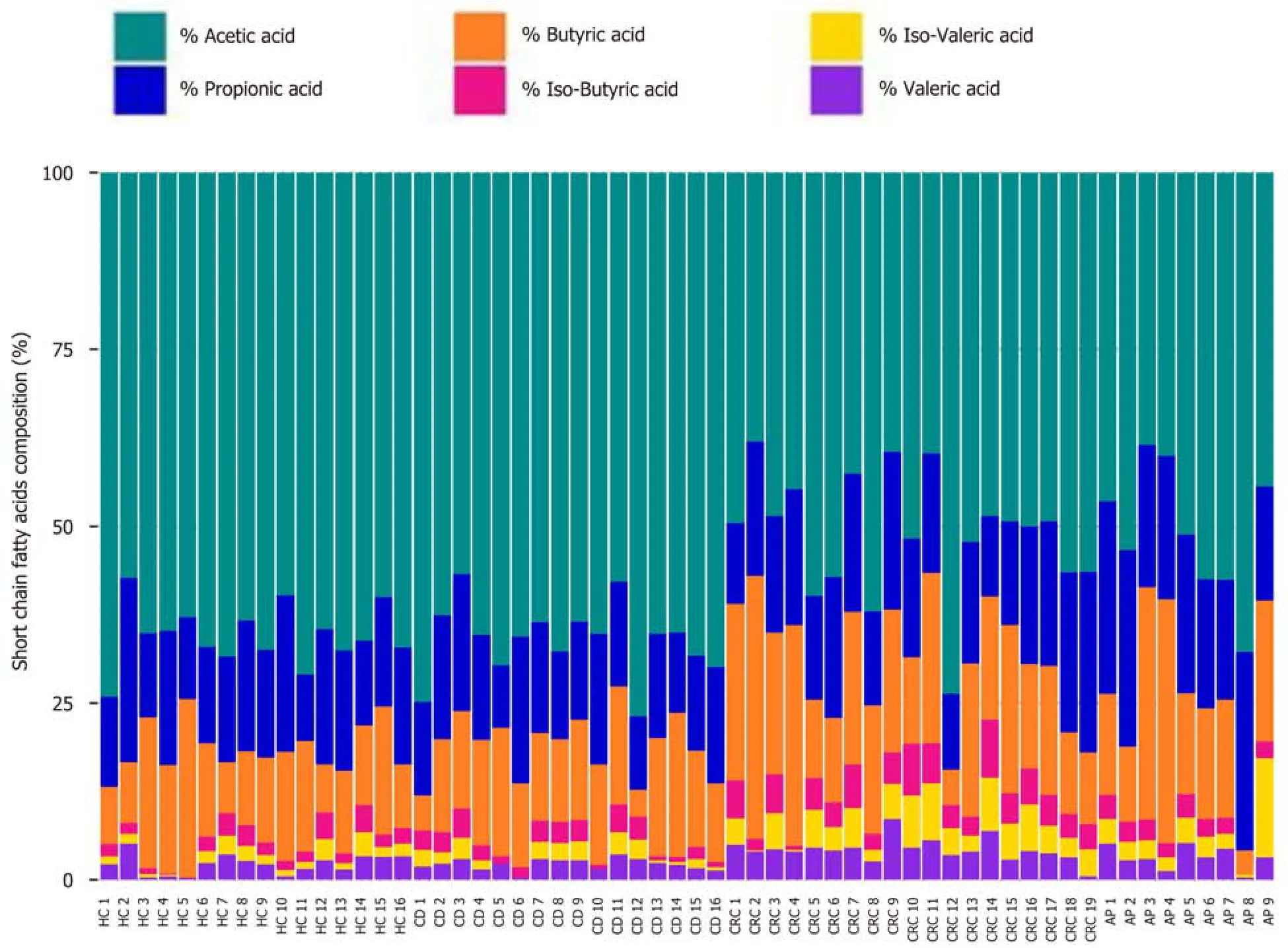
Figure 1 Barplot of relative abundances of fecal short chain fatty acids' of healthy controls and celiac disease, colorectal cancer, adenomatous polyposis patients.
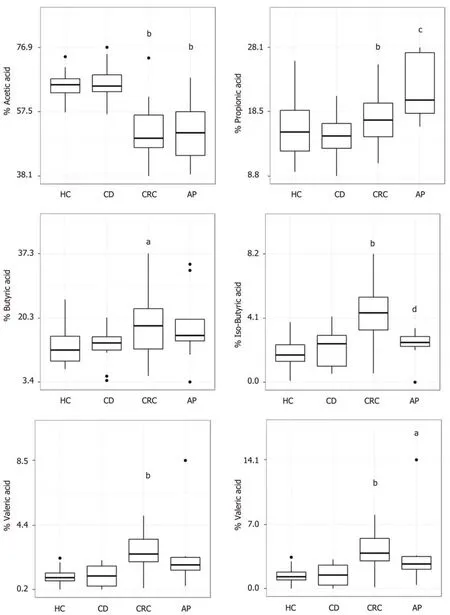
Figure 2 Representation of each short chain fatty acid percentage in celiac disease, colorectal cancer, adenomatous polyposis patients and healthy controls. The differences between States were assessed using the Wilcoxon test. aP < 0.05 vs HC, bP < 0.01 vs HC, cP < 0.05 vs CRC and dP < 0.01 vs CRC.
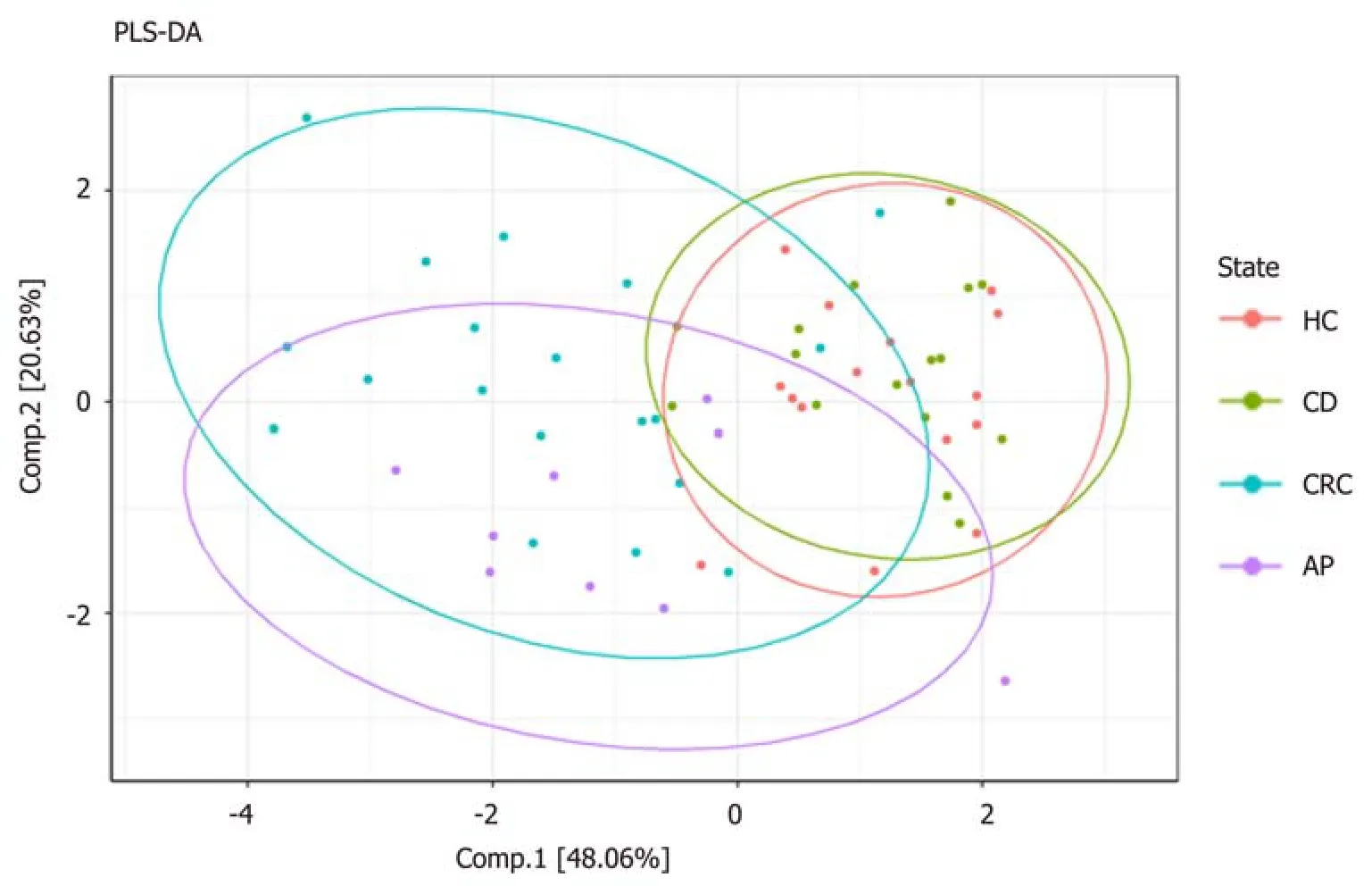
Figure 3 Partial Least Squares Discriminant Analysis scores plot. PLS-DA: Partial Least Squares Discriminant Analysis; HC: Healthy control; CD: Celiac disease;CRC: Colorectal cancer; AP: Adenomatous polyposis.
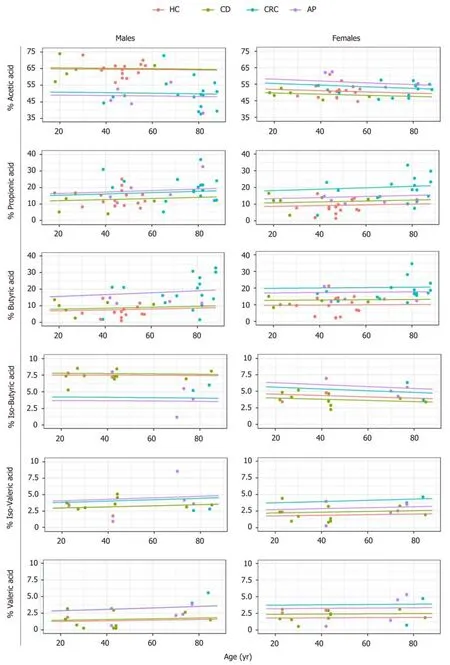
Figure 4 Expected proportions from the dirichlet regression model (lines) vs short chain fatty acids' observed values (points), color coded by state. HC:Healthy control; CD: Celiac disease; CRC: Colorectal cancer; AP: Adenomatous polyposis.
ARTICLE HIGHLIGHTS
Research background
An alterated status of the gut microbiota is usually responsible for a reduction of short chain fatty acids (SCFAs), the major metabolites produced by bacterial fermentation, that are essential in maintaining gut homeostasis. Different studies have documented an alteration in SCFAs'composition in various human pathologies, that may reflect a dysbiotic condition affecting the healthy status.
Research motivation
The SCFAs' determination in stool samples could provide a faster, reliable and cheaper method to highlight the presence of an intestinal dysbiosis. Anyway, the high heterogeneity of methods used for their determination (i.e., gas chromatography, high performance liquid chromatography, nuclear magnetic resonance, capillary electrophoresis) make difficult to compare literature data and bringing out real differences in SCFAs' profiles of various disorders. Indeed,the use of a standardized protocol for their evaluation is essential to understand if the fecal SCFAs signature could represent a potential biomarker in the clinical practice, for example for the detection of different gut diseases.
Research objectives
The main objective of this study was to compare the fecal SCFAs' profile of patients with adenomatous polyposis (AP), celiac disease (CD) and colorectal cancer (CRC) to healthy controls(HC), applying the same protocols and analytical conditions gas chromatography-mass spectrometry (GC-MS) for their evaluation, in order to point out whether these pathologies displayed a particular fecal SCFAs signature.
Research methods
In this cross-sectional study, we defined and compared the SCFAs' concentration in fecal samples of 44 patients with different gut diseases (19 with CRC, 9 with AP, 16 with CD) and 16 healthy controls. The SCFAs' analysis were performed using a GC-MS method. Data analysis was carried out using Wilcoxon rank-sum test to assess pairwise differences of SCFAs' profiles,partial least squares-discriminate analysis (PLS-DA) to determine the status membership based on distinct SCFAs' profiles, and Dirichlet regression to determine factors influencing concentration levels of SCFAs.
Research results
In our study, we have not observed any difference in the SCFAs' amount and composition between CD and healthy control. On the contrary, the total amount of SCFAs was significantly lower in CRC patients compared to HC and CD. Moreover, the percentage of each SCFA changed in CRC and AP patients compared to HC. In particular, HC displayed a higher percentage of acetic acid and a lower amount of butyric, isobutyric, isovaleric and valeric acids compared to CRC patients. Regarding AP patients, they showed a lower abundance of acetic acid and higher percentages of propionic and isovaleric acids compared to HC. Moreover, the PLS-DA model performed on the SCFAs' percentages matrix, confirmed that CRC and AP patients showed a distinct separation from the healthy subjects and were not coinciding. Overall the small sample size of this study does not allow us to reach definitive conclusions, and our findings remain exploratory.
Research conclusions
In this study we have analyzed, for the first time, the fecal SCFAs' profile of patients with different gut diseases (AP, CD and CRC) and healthy subjects, applying the same protocols and analytical conditions (GC-MS). Even if the small sample size of study does not allow us to reach definitive conclusions, our findings shown the existence of a fecal SCFAs fingerprint in patients with CRC, with a clear separation (with significant qualitative and quantitative differences) in the SCFAs' composition, compared to healthy control. In addition, AP patients have showed a characteristic SCFAs' profile, distinguishable from CRC and healthy subjects. On the contrary,no separation between celiac patients and healthy controls was obtained regarding the SCFAs'composition profile. If confirmed in larger cohorts of patients, we think that the fecal SCFAs'analysis through GC-MS could be considered as a noninvasive and reliable diagnostic marker for the detection of adenoma and CRC patients.
Research perspectives
By comparing the fecal SCFAs signatures of different gut disease using the same analytical method, we realized the clinical and diagnostic potential of our preliminary result, suggesting the use of SCFAs as potential biomarker in adenomatous polyposis and colorectal cancer. In our future research we will enlarge the sample size of this study to confirm the specific fecal SCFAs fingerprints in CRC and AP, in order to develop a non-invasive diagnostic protocol to be used in gastrointestinal clinical practice. The best method for future research is to continue the comparison of fecal SCFA profile in cohorts of patients with different diseases, where the microbiota has been shown to be involved. Examining a statistically significant number of patients with the same protocol used in this study, will be crucial to reach definitive conclusions.If our result will be confirmed, the fecal SCFAs' analysis through GC-MS could be proposed as an innovative, noninvasive and reliable diagnostic method for the detection of adenoma and CRC patients and, in future, for other pathologies.
杂志排行

World Journal of Gastroenterology的其它文章
- Chinese guidelines on management of hepatic encephalopathy in cirrhosis
- Sexual health and fertility for individuals with inflammatory bowel disease
- High mobility group box-1 release from H2O2-injured hepatocytes due to sirt1 functional inhibition
- Zinc-α2-glycoprotein 1 attenuates non-alcoholic fatty liver disease by negatively regulating tumour necrosis factor-α
- Clostridium butyricum alleviates intestinal low-grade inflammation in TNBS-induced irritable bowel syndrome in mice by regulating functional status of lamina propria dendritic cells
- CARMA3/NF-κB signaling contributes to tumorigenesis of hepatocellular carcinoma and is inhibited by sodium aescinate