Elderly patients with inflammatory bowel disease: Updated review of the therapeutic landscape
2019-08-26JeanFrricLeBlancDanielWisemanPeterLakatosTalatBessissow
Jean-Frédéric LeBlanc, Daniel Wiseman, Peter L Lakatos, Talat Bessissow
Abstract High-quality data remains scarce in terms of optimal management strategies in the elderly inflammatory bowel disease (IBD) population. Indeed, available trials have been mostly retrospective, of small sample size, likely owing to underrepresentation of such a population in the major randomized controlled trials.However, in the last five years, there has been a steady increase in the number of published trials, helping clarify the estimated benefits and toxicity of the existing IBD armamentarium. In the Everhov trial, prescription strategies were recorded over an average follow-up of 4.2 years. A minority of elderly IBD patients (1%-3%) were treated with biologics within the five years following diagnosis, whilst almost a quarter of these patients were receiving corticosteroid therapy at year five of follow-up, despite its multiple toxicities. The low use of biologic agents in real-life settings likely stems from limited data suggesting lower efficacy and higher toxicity. This minireview will aim to highlight current outcome measurements as it portends the elderly IBD patient, as well as summarize the available therapeutic strategies in view of a growing body of evidence.
Key words: Inflammatory bowel disease; Elderly; Outcomes; Glucocorticoids; Biological therapy; Surgery
INTRODUCTION
Crohn’s disease (CD) and ulcerative colitis (UC), collectively known as inflammatory bowel diseases (IBD), are most often diagnosed in a younger age group, although they are increasingly being recognized in the elderly population. Given that IBD is a chronic illness and the longer longevity, the proportion of elderly IBD patients will only increase over time. It is estimated that up to 25%-30% of the IBD population are aged sixty or older, of which half were diagnosed above the age of sixty, better known as elderly- or late-onset IBD[1]. Indeed, a Swedish population-based study compiled all incident cases of IBD over a seven-year period (total of 27834 patients): 23% were aged 60 or over (mean age at diagnosis of 69), which represents a sizeable proportion expected to rise[2]. Indeed, in a Canadian observational study, prevalence of IBD in the elderly increased by 5.8% between 1999 and 2008, compared to 3.9% in the nonelderly population[3]. Definition of older age in the IBD population may vary in the medical literature, from ages 55 to 70. The topical review on IBD in the elderly,published by the European Crohn’s and Colitis Organisation in late 2016, establishes the age of 60 as the most widely-accepted determinant of elderly age[4]. However,frailty assessment is believed to be a better predictor of poor IBD-related outcomes,more so than chronological age alone, based on limited surgical data[4-5]. The mean number of comorbidities in the elderly IBD population ranges from 2 to 3[4,6].Comorbid illnesses may complicate the management of elderly IBD patients. For example, a shorter lifespan from other comorbidities may limit the expected benefit of colorectal dysplasia screening protocols. Diabetes mellitus, congestive heart failure and chronic kidney disease represent common conditions in the elderly and may be affected by certain treatment regimens such as corticosteroids or biologic agents. In fact, in an American retrospective study, 393 elderly IBD patients were known for coronary artery disease (33.8%), chronic lung disease (22.6%), congestive heart failure(22.6%), diabetes mellitus (18.8%) and moderate to severe renal disease (11.5%) at the time of the IBD diagnosis[6].
The elderly IBD patient population should be separated into two groups (adultonset elderly IBD and elderly-onset IBD), based on their different disease phenotypes,prognoses and management plans. For example, adult-onset IBD patients aged 60 or above are considered to be at higher risk of disease progression in UC (28% vs 16% at ten years) and harbor an increased prevalence of perianal disease upon follow-up in CD (27% vs 17%, average follow-up of 6 years)[7-8]. Otherwise, patients with late-onset IBD tend to have milder, colonic disease. Most published cohorts from various countries have shown higher prevalence of UC cases in the elderly, compared to CD:11%-21% vs 5%-17% respectively[7-9]. In the previously-mentioned Swedish registry,left-sided disease in UC is seen more commonly in the elderly than the adult population (28% vs 15%), as opposed to proctitis (14% vs 23%), and extensive disease(28% vs 34%)[2]. In CD, fibrostenotic disease was more common in the elderly (23% vs 9%), contrasting with lower rates of penetrating disease (5% vs 11%). Extra-intestinal manifestations were also compared: the rates of primary sclerosing cholangitis and cutaneous manifestations were similar in both the elderly and non-elderly populations. Otherwise, arthritis was more commonly seen in the adult population(8% vs 6%, P value = 0.0001), while elderly patients had statistically higher rates of ocular manifestations (2% vs 1%, P value = 0.02)[2]. In regards to prescription practices,two population-based cohorts from Hungary and France have shown that age at diagnosis predicts higher utilization of corticosteroids and immunosuppressive drugs in the adult-onset population. Indeed, the Hungarian cohort showed that azathioprine was more commonly prescribed in adult-onset CD patients compared to the elderly population at a median follow-up of 11 years (42.6% vs 28.6%, P value < 0.001), as well as systemic steroids (39.8% vs 17%, P value < 0.001)[7]. The French EPIMAD cohort supports the findings from Hungary, describing decreased prescription rates of immunomodulator drugs in elderly-onset patients (cumulative probability of 27% in CD and 15% in UC at ten years of follow-up), as well as higher rates of 5-Aminosalicylic Acid products (cumulative probability of 80% in CD and 84% in UC),due to its perceived safety in the elderly[8].
Advanced age in IBD has been associated with increased risk of infections,malignancy, polypharmacy, comorbidities, corticosteroid-induced complications,malnutrition, perioperative morbidity and mortality[10]. In fact, retrospective data suggest a ten-fold increase in the 30-day post-operative mortality among elderly IBD patients compared to a younger population (CD 4.2% vs 0.3%; UC 6.1% vs 0.7%)[11]. In order to avoid the IBD-related complications and their impact on elderly patients’quality of life, controlling disease remains crucial. Over the last twenty years, use of biologic agents has revolutionized the IBD therapeutic landscape, leading to major changes in therapeutic targets in order to prevent recurrent flares. However, concerns about decreased efficacy due to immune senescence and a higher side effect profile in the elderly population has led to a relative underutilization of biologic agents, not solely explained by milder disease severity seen in the elderly population. In the current state of evolving treatment targets, this review will provide an evidence-based summary of the efficacy and safety of the IBD therapeutic agents in the elderly population.
OUTCOME MEASURES
Influential IBD drug clinical trials have focused on disease-related outcomes, such as clinical response or remission, avoidance of corticosteroid use and post-operative morbidity and mortality. In the last ten years, American and European Associations have produced guidelines in order to ensure a transition towards objective outcomes,namely mucosal healing and its biochemical surrogates, such as C-reactive protein(CRP) and fecal calprotectin (FCAL)[12-13]. Although mucosal healing remains an ideal treatment target, therapeutic goals in elderly patients may be different in light of their relatively shorter lifespan compared to the adult population. Indeed, physicians may opt to tolerate mild endoscopic activity in view of perceived lower long-term risks of colorectal malignancy or IBD-related complications.
CRP and FCAL have not been specifically validated in the elderly IBD population.Firstly, geriatric frailty has been associated to a low-grade inflammation, inducing increased levels of serum CRP, tumor necrosis factor - alpha (TNF-α) and interleukin-6, despite excluding cardiovascular disease, diabetes and adjusting for basic demographic characteristics[14]. It can thus be difficult to ascertain whether CRP elevation in the elderly IBD population is a reflection of disease activity or a sign of frailty possibly due to malnutrition or other comorbidities. Secondly, FCAL levels are increased in the setting of various diseases, including, although not limited to,diverticulitis, ischemic colitis, colorectal malignancy, as well as certain drugs, such as proton pump inhibitors and nonsteroidal anti-inflammatory drugs, all of which are more commonly seen in the elderly population[15]. Biomarkers’ specificity to predict disease activity may thus be lower in the elderly IBD population. Further trials are needed to validate the use of biomarkers in the elderly IBD population.
A rising prevalence of elderly IBD patients implies higher costs and increased complexity of health-care delivery, thus justifying a shift towards a standardized model conceived by patient-reported outcomes (PROs) considered most relevant[16].Few studies in the elderly IBD population included FDA-recognized PROs as a primary outcome. One such trial assessed five types of PROs (depression, anxiety,pain interference, sleep disturbances and fatigue). At six months of follow-up, 636 elderly IBD patients on continued steroid use had higher rates of depression (mean 50.8 vs 48.2, P = 0.03) and anxiety (mean 52.6 vs 49.8, P = 0.04) based on validated questionnaires, compared to elderly patients on immunomodulators or anti-TNF agents (without steroid use) after adjusting for disease activity[17]. Depression, anxiety and sleep disturbances may further decrease elderly patients’ quality of life, therefore increasing the importance of corticosteroid-sparing therapy.
The Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE)program, designed to establish the appropriate treatment targets for IBD, suggests serial outpatient assessment of PROs minimally every three months until resolution,then every six to twelve months[18]. However, the optimal PRO instrument has not yet been clearly identified. In an effort to strive for value-based medicine, the International Consortium for Health Outcomes Measurement (ICHOM) and the Oxford Academic Health Network collaborated to devise four domains encompassing the most relevant IBD-related PROs: Symptoms and Quality of Life, Survival and Disease Control, Disutility of Care and Healthcare Utilization[19]. A short, inexpensive test, the IBD-Control questionnaire (IBD-CQ), was recommended as the most reliable measurement of PROs, although its validation process requires further prospective studies[19-20]. Although data in the elderly population is lacking, PRO instruments, such as the IBD-CQ, can potentially capture the decreased health-related quality of life in this vulnerable population and further guide the clinician towards symptom-specific strategies.
MEDICAL THERAPY
5-Aminosalicylic acid
Current guidelines suggest that 5-Aminosalicylic acid (5-ASA) should be used for inducing remission and for maintenance therapy in mild-to-moderate UC (AGA guidelines); however, the role of 5-ASA in CD is less clear and is currently not supported by major guidelines[21]. A recent population-based study from Hungary included 11240 elderly UC patients and 3172 elderly CD patients. In this study, 72% of elderly UC patients and 69% of elderly CD patients were receiving 5-ASA products.In the 20-59 year age group, 73% of UC patients and 71% of CD patients used 5-ASA products, indicating similar usage between these two age groups[21]. Similar results were seen in a retrospective analysis from Poland; out of 8,265 elderly UC patients,89% were using 5-ASA compared to 76.5% of elderly CD patients (total of 1387 elderly CD patients). In this trial, the exposure to 5-ASA was similar between the adult and elderly groups[23]. In contrast, in their cohort of 6443 cases, Everhov et al[2]found that,at 5-year follow-up, only 29% of elderly CD patients and 57% of elderly UC patients were using 5-ASA respectively. These findings demonstrate that, despite the current guidelines, a significant proportion of the elderly CD population are being prescribed 5-ASA products. One theory for the use of 5-ASA in the maintenance therapy of CD suggests that its popularity may be due to its relatively safe side-effect profile[24].While the studies above suggest that 5-ASAs are widely prescribed for both UC and CD, it is important to consider their potential side effects. In a recent retrospective review from the Swiss IBD cohort which included 3192 patients of all ages, 7.9% of patients discontinued their 5-ASA[25]. The most common reasons for discontinuation of therapy were nausea and/or diarrhea (0.9%), gastrointestinal intolerance (0.4%) and nephritis (0.3%). With regards to nephrotoxicity associated with 5-ASA, a recent genome-wide association study found that the median age of nephrotoxicity was 39.4 years old, that it could manifest itself at any age and that there is genetic predisposition explaining its development[26].
In addition, there is currently insufficient evidence to suggest that there exists a difference in the efficacy of 5-ASA between the younger and older IBD populations.Regardless of the type of the disease, in elderly IBD patients, certain particularities come to the forefront. For example, while many young IBD patients are able to autoadminister suppositories, this may be difficult for an older person. Also, the prevalence of fecal incontinence among elderly patients in the outpatient setting has been shown to be as high as 9.9%, which raises concern for inadequate absorption or administration of suppositories and enemas[27]. Of note, for the elderly population at risk for polypharmacy, 5-ASA has been shown to interact with Warfarin[28]. In addition, combining antacids and 5-ASA may hinder the therapeutic effects of 5-ASA[29].
Steroids
Corticosteroids play a n important role in inducing remission with IBD. However,current guidelines do not recommend their use for maintenance therapy largely because of their unfavorable side-effects (AGA). Studies analyzing treatment trends in elderly IBD patients have shown that this population seems to use less immunomodulators and biologic agents, and more corticosteroids than their younger counterparts[6]. In fact, the Everhov study revealed that, in regards to elderly CD patients, 17% were using immunomodulators and 22% were using corticosteroids by the 5thyear of follow-up[2]. In elderly UC patients, by the 5thyear of follow-up, 9%were using immunomodulators and 23% were using corticosteroids. Additionally, in a cohort study including 190 elderly patients with IBD, regular corticosteroid use seemed to remain common. When groups were stratified based on moderate-tosevere disease activity (n = 61), 71% of these patients were using corticosteroids chronically, only 25% and 35% had received biologics and immunomodulators,respectively. Furthermore, 24% of patients in remission or with mild disease were using chronic steroids[30].
In a recent population-based study analyzing 465 patients with elderly-onset ulcerative colitis, Duricova et al[31]found that there was a 20.4% cumulative probability that patients receive corticosteroids within the first year since diagnosis and a 31.5%cumulative probability within the first five years. A total of 151 patients were exposed to corticosteroids and patients had a yearly median exposure period of 23 d. Twelve patients (7.9%) experienced adverse events, with new-onset diabetes mellitus being the most common. With regards to steroid dependency, 31 patients (20.5%) became steroid dependent over the study period; there was no significant difference in the incidence of new-onset steroid-dependent disease between patients older and younger than 70 years. Finally, steroid resistance, defined as no response to maximal doses of intravenous steroids and therefore requiring surgery or need for additional cyclosporine or infliximab, was more common in elderly patients < 70 years vs those >70 years.
Studies have shown that there is an increased risk of adverse events in association with corticosteroid use in elderly IBD patients; these include (but are not limited to)both serious infections and death. Indeed, in the TREAT registry, 55 out of 6290 patients died. The independent predictors of death proved to age, duration of CD disease and the use of prednisone[32]. With regards to serious infections, 106 patients suffered from such a complication. The independent predictors of serious infection included race, duration of CD disease, moderate-to-severe CD disease, the use of narcotics and finally, the use of prednisone. In addition, in their study, Brassard et al.identified 564 cases of serious infection in their cohort of 3552 elderly-onset IBD patients[33]. The authors found that those patients currently using corticosteroids(within the last 45 d) and those exposed to corticosteroids within the last 90 days were at an increased risk for serious infections.
Additionally, in a recent retrospective study by Govani et al[34]with 12276 IBD patients 65 years and older, older patients were found to have a significantly increased fracture risk at 1 year following the initiation of corticosteroids when compared to younger patients. Of note, both venous thromboembolism and infection were more frequently encountered with corticosteroid users; although there was no significant difference in rates of these secondary effects between the older and younger patient groups. Also, in a cross-sectional study followed by longitudinal analysis, self-reported IBD patients 60 years and older treated with corticosteroid monotherapy had significantly worsened depression and anxiety at 6 month followups when compared to others (from the same age bracket) treated with immunomodulators or anti-TNF agents without corticosteroids. In addition, corticosteroid use was associated with sleep disturbance, fatigue and worsened anxiety when compared to non-corticosteroid users[16].
In addition to side effect profile, corticosteroids have the potential to interact with various medications as well. Interactions with Rifampin, Phenytoin and even anticoagulants have been reported and should be kept in mind when deciding on a therapeutic regime[35]. There is currently insufficient evidence to comment on the efficacy and safety of budesonide in the elderly IBD population. Notably, the authors of major trials mentioned that the geriatric population was under-represented[36].
Thiopurines
Similarly to 5-ASA, there is insufficient evidence to suggest that the treatment efficacy of thiopurines in the older IBD population is different than that of the younger population. Still, studies have shown a low usage of thiopurines in the elderly population that is most likely driven by the higher risk of malignancy associated with this class of drugs[29,37]. Indeed, in their various prospective observational studies, the CESAME Study group has found that ongoing and previous exposure to thiopurines increase the risk of developing non-melanoma skin cancer, that previous exposure comes with a seven-fold increased risk of developing a myeloid disorder and that ongoing exposure increases the risk of urinary tract cancers[38-39]. In the study by Duricova et al[31], there was a 2.6% probability that patients underwent thiopurine therapy within the first year since diagnosis and a 9.7% probability within the five years since diagnosis. Thiopurines were used in 44 subjects (9.4% of patients). Five of these patients experienced a cytopenia and four patients experienced gastrointestinal intolerance. In a population-based study including 4107 elderly IBD patients, Alexakis et al[37]found that, in patients with elderly-onset UC (60 years and older at diagnosis),there was a 70% reduced risk of colectomy in those patients treated with thiopurines for more than 12 mo. Of note, this reduction in surgical risk was not observed in elderly-onset Crohn’s disease patients who had received thiopurine treatment for more than 12 mo.
While these findings are interesting, the side effects of these agents must be considered. Reports of increased risk of developing malignancy in association with thiopurine use have surfaced. In fact, a recent cohort study (in which patients 65 years and older represented 12% of the study population) by Lemaitre et al[40]found that risk of lymphoma was higher in patients treated with thiopurine monotherapy (mean exposure time was 17 mo) and those treated with combination therapy (thiopurine and anti-TNF, mean exposure time was 8 mo) in comparison to those patients unexposed to such treatments. In addition, in their retrospective observational study,Bahi et al[41]showed a potentially multiplicative risk of non-melanoma skin cancer with increasing age in thiopurine-exposed IBD patients (6 months or longer exposure,median exposure of 42 months). In contrast, a recent cohort study by Cheddani et al[42]of elderly-onset IBD found that thiopurine exposure was not associated with an increased risk of developing cancer when using a time-dependant Cox model.
Besides malignancy, in a French cohort study including 190694 IBD patients aged 18 years and older, both patient groups exposed to thiopurine monotherapy and combination therapy (thiopurine and anti-TNF) were at increased risk for serious infections and opportunistic infections when compared to those who were unexposed to these regimens. Of note, the absolute risks of developing either serious or opportunistic infections were at least double in patients 65 years and older, compared to younger patients[43]. Furthermore, in a post hoc analysis of the Thiopurine response Optimisation by Pharmacogenetic testing in Inflammatory Bowel Disease Clinics(TOPIC) trial, both older age and combination therapy with thiopurines and biologics were associated with an increased risk of infection in patient without a TPMT variant[44]. This trial included 105 patients 60 years and older.
Otherwise, several interactions have been reported with thiopurines. They have been shown to inhibit the effects of warfarin[28]. Also, when combined with 5-ASA or allopurinol, thiopurine metabolite levels may increase leading to serious complications[45].
Methotrexate
While studies evaluating the efficacy of methotrexate (MTX) in both the paediatric and adult IBD populations have been done, there is limited evidence regarding its role in older IBD patients. Currently, methotrexate is recommended for steroiddependant Crohn’s disease and for maintenance of remission (AGA).
Common side effects of methotrexate include (but are not limited to) nausea, liver toxicity and bone marrow suppression[24]. In a recent retrospective review including 3192 IBD patients of all ages, 19.8% of patients treated with Methotrexate discontinued the drug due to side effects. The most common reasons for dis-continuation were gastrointestinal effects, namely nausea and vomiting, but also an increase in liver enzymes. Furthermore, one study analyzing the use of methotrexate in 112 IBD patients found that patients not receiving folic acid were at a fivefold increased risk of experiencing side effects[46]. While the addition of folic acid may seem insignificant,this may pose a challenge to the older IBD patient who is already at risk for polypharmacy and may have more difficulty complying to a complicated medical regimen.
Of note, methotrexate is mainly excreted by the kidneys; therefore, drug accumulation occurs with a lower glomerular filtration rate, as seen more commonly in the elderly population, thus potentially intensifying its side effects[47].
Biologic agents
Biologic therapy regroups a wide array of immunosuppressive agents, wherein the main mechanism of action relies on antibody-mediated downregulation of the inflammatory cascade. Infliximab and adalimumab, the first biologics used in the treatment IBD, directly inhibits the effects of serum and mucosal TNF, thereby reducing mucosal inflammation. Trials showed that a third of patients lose response to TNF blockers within 1 year, compounded to a non-negligible infectious risk.Therefore, newer biologics were introduced in order to target downstream mediators of gut inflammation, such as the anti-integrins (vedolizumab) and the anti-interleukin 12-23 (ustekinumab). Based on retrospective and population-based data, biologic agents in the elderly IBD population are rarely utilized, as low as 2% in UC patients and 6% in CD patients at 5 years following date of diagnosis, compared to 7% and 20% in the adult population[2,29]. In these trials, 20%-32% were receiving maintenance prednisone, defined as a treatment duration of six months or more. Existing evidence,although limited, has suggested lower efficacy and increased risk of infections,possibly mortality, of biologic agents used in the elderly population, likely resulting in suboptimal management strategies, including corticosteroid prescriptions.
TNF-α blockade:Data is conflicting regarding the efficacy and safety of biologic agents in the elderly, mostly explained by the limited number of elderly patients in the major IBD randomized controlled trials, wherein median age is in the range of 35 to 40[48-50]. Either elderly patients are explicitly excluded from these trials, or the intensity of follow-up visits leads to incomplete data collection and consideration as a loss to follow-up.
Of the few trials assessing efficacy of anti-TNF therapy in the elderly, outcomes have been largely clinical, rarely including biochemical and endoscopic parameters(as shown on Table 1), the latter two deemed more reliable in predicting disease course in most international guidelines. A Leuven nested case-controlled study of 66 elderly-onset IBD patients on anti-TNF therapy showed a significantly lower rate of short-term clinical response at 10 weeks in the elderly IBD (68% vs 89%: P < 0.001)[51].However, efficacy was similar between younger and elderly patients at 6 months of biologic therapy, suggesting a prolonged time to treatment effect in the elderly.Interestingly, in this trial, elderly-onset and adult-onset IBD patients had similar rates of clinical response. In a study of 58 patients by Desai et al[52], 61% of elderly IBD patients achieved complete or partial clinical response at 12 mo, compared to 83% of the younger population. Discontinuation of anti-TNF therapy is reported as more common in the elderly population compared to non-elderly patients (25% vs 7%assessed at 12 mo: P < 0.001), explained by lower rates of clinical response and increased infectious complications[51].
More recent data has suggested sustained efficacy rates over a twelve-month period, although not compared to a younger population. In a large multicenter,retrospective trial by Adar et al[53], 131 elderly IBD patients on anti-TNF maintained remission status, defined as a peer-reviewed clinical, biochemical and endoscopic assessment, in 50% of cases at 3 mo, 54% at 6 mo and 58% at 12 mo. Lower rates of remissions were associated with increasing age (for each one-year increase in age: OR= 0.94, 95%CI: 0.89-0.99). Notably, at the initiation of the anti-TNF, 36% of these patients were treated with combination therapy (using thiopurine or methotrexate combined to a biologic agent). Compared to anti-TNF monotherapy, combination therapy was not associated with increased rates of remission at any time period (P >0.10). In the existing elderly IBD-related literature, data is otherwise scarce regarding the potentially higher efficacy of combination therapy seen in younger patient populations.
Safety profile remains a significant issue in the elderly IBD population for most therapeutic agents. Higher rates of adverse events due to steroids, immunomodulators and biologic agents in the elderly population can be explained by senescence of the immune system, increased comorbidities and potential drug interactions. Upper and lower respiratory tract infections remain the most commonlyreported infections. In the previously-mentioned Leuven study, advanced age (≥ 65 years) was associated with higher rates of serious adverse events on anti-TNF therapy, such as infections and malignancy (relative risk 4.7; P < 0.001), compared to non-elderly IBD patients[51]. Upon adjustment for comorbidities, rates of malignancy were similar between the two groups (HR = 2.64, 95%CI: 0.70-10.04), implying that presence of comorbidities in the elderly IBD population represents the main risk factor for malignancy. A large, multicenter observational trial showed similar results:elderly IBD patients were more likely to suffer from infections compared to a younger population, malignancy and even death, irrespective of disease duration (13% vs 2.6%,3% vs 0% and 10% vs 1%, respectively), as seen on Table 1[54]. In multiple studies,advanced age in IBD is recognized as an independent risk factor for lymphoproliferative disorders, especially in the setting of thiopurine use[55-56]. Data from the TREAT registry suggests that anti-TNF monotherapy does not infer an increased risk of lymphoproliferative disorders (five-year incidence of 0.05 per 100 patientyears, compared to 0.06 per 100 patient-years in IBD patients who received other treatments only)[57]. Longer-term studies are needed to establish the risk of lymphoproliferative disorders in elderly IBD patients on biologic therapy, including effect measurement of prior thiopurine use.
A recently-accepted meta-analysis by Borren et al[58]assessed the safety profile of biologic agents in the treatment of elderly patient with auto-immune diseases (IBD,rheumatoid arthritis, psoriasis). Of the fourteen included studies, six retrospective studies focused solely on IBD, comprising a total of 349 elderly biologic users, 450 elderly non-biologic users and 822 non-elderly biologic users. Elderly IBD patients on biologic therapy (mostly anti-TNF) were three times more at risk of infections (OR =3.48, 95%CI: 1.98-6.14) and malignancy (OR = 3.47, 95%CI: 1.71-7.03), compared to their younger counterparts. Upon considering strictly elderly patients, the authors noticed that patients on biologic agents were eleven times at higher risk of infections compared to those not receiving biologics (OR = 11.22, 95%CI: 3.6-34.99), while similar rates of malignancy were measured between these two groups (OR = 0.53, 95%CI:0.26-1.08). As expected in a meta-analysis of small retrospective studies, several data points are missing, such as comorbidity risk scores, types of malignancy and infections and active corticosteroid or immunomodulator therapy, limiting this study’s impact on clinical practice. Existing data in the elderly IBD population suggests that use of anti-TNF agents is an independent risk factor for infections(minor and severe), emphasizing the importance of prophylactic measures, such as hand hygiene and immunization guidelines. Current data regarding malignancy risk remains conflicting; no specific screening is deemed required as per the ECCO Topical Review on IBD in the elderly[4]. Otherwise, anti-TNF agents should be avoided in severe cases of congestive heart failure, whereas milder disease requires closer surveillance, although data is lacking regarding cardiovascular surveillance protocols[4].
Inhibition of leukocyte trafficking:Vedolizumab, a monoclonal antibody directed against the integrin subunit α4β7, prevents circulating lymphocytes to interact with mucosal cell adhesion molecule-1 (MAdCAM-1), thereby reducing the migration of inflammatory cells towards colonic mucosa. A post hoc analysis of the GEMINI trials from Yajnik et al[59]showed that, across different age groups (≤ 35, 35-55, ≥ 55),vedolizumab had similar rates of corticosteroid-free remission at 52 weeks,respectively 32.6% vs 26.7% vs 28.6% for CD and 33.3% vs 42.3% vs 38.1% in UC. In the same trial, rates of malignancy and infections in the elderly population were mostly similar compared to their younger counterparts, as in 0.4% vs 0.5% vs 0% for malignancy, as high as 87% vs 84.7% vs 77.4% for any infection and 7.5% vs 4.4% vs 0.9% for serious infections (see Table 2 for the study demographics). The unusual trend of higher serious infections in the younger population was also captured in the original GEMINI trials, which were not designed to assess these specific subgroups.Indeed, these results should be interpreted with caution due to the small sample size(only 90 patients aged 55 or older, compared to 582 and 443 in the other two groups)and inadequate power to detect statistical significance.
In the previously-mentioned Adar et al. trial, 234 elderly-onset patients were assessed retrospectively at the time of biologic initiation, separated in two groups:anti-TNF agents (n = 131) and vedolizumab (n = 103)[53]. As can be expected, the main measurable difference between groups was the increased proportions of perianal disease in the anti-TNF group (25% vs 14%, P = 0.02). Rates of remission were numerically higher, although not statistically significant, in the anti-TNF group at 3 months (50% vs 38%, P = 0.07), then became comparable at 6 mo (54% vs 45%, P =0.23) and 12 mo (58% vs 54%, P = 0.63). Additionally, use of anti-TNF was associated with higher odds of remission in CD at 3 months (OR = 2.82, 95%CI: 1.18-6.76) but not UC (OR = 1.74, 95%CI: 0.74-4.13) and comparable odds between groups at 6 and 12 mo. In keeping with existing data on biologic agents’ pharmacokinetics, these findings suggest a relatively quicker onset of action from anti-TNF agents compared to vedolizumab. Data from the 6- and 12-mo period suggest that both agents share similar durability of response.
Notably, rates of significant infections are comparable between groups within one year of initiation: 20% for anti-TNF and 17% for vedolizumab, most commonly pneumonia in both groups. Vedolizumab was thought to potentially increase the risk of gastrointestinal infections due its gut-selective mechanism of action, a risk not encountered in the GEMINI trials and in this trial. Incidence rates of Clostridium difficile infection and gastrointestinal infections were also similar between groups(21% vs 18%, P = 0.57). New primary or recurrent malignancies were diagnosed in 3%of anti-TNF patients and 1% of vedolizumab-treated patients, although not statistically significant (P = 0.27)[53]. The Adar et al[53]study is the largest to compare efficacy and safety of biologic agents in the elderly IBD population. As opposed to extrapolations from the GEMINI data (similar rates of infections between vedolizumab and placebo arms), the findings from Adar et al[53]do not capture significantly lower rates of infections compared to anti-TNF agents, possibly explained by the small sample size, short follow-up period and retrospective nature of the trial. Additional trials of comparable size are needed to better elucidate the safety profile of vedolizumab compared to anti-TNF agents.
Interleukin 12 and 23 blockade:Otherwise, ustekinumab, a monoclonal antibody targeting the common p40 subunit of interleukin-12/23, has shown favorable efficacy and safety outcomes in the UNITI and IM-UNITI trials[50]. However, stratification by age was not performed, resulting in the analysis of a relatively young patient population (average age of 38). Data is otherwise scarce for ustekinumab in the treatment of elderly IBD patients. Regarding the psoriasis literature, two small retrospective trials (46 patients in total) suggested no increased risk of adverse events with ustekinumab at 52 wk, although ustekinumab dosing is significantly lower in psoriasis treatment compared to IBD dosing[60-61]. Such limited data has not clearly proven that clinicians should opt for the newer classes of biologic agents as a first-line intent in the hopes of blunting potential toxicity in the elderly IBD population.
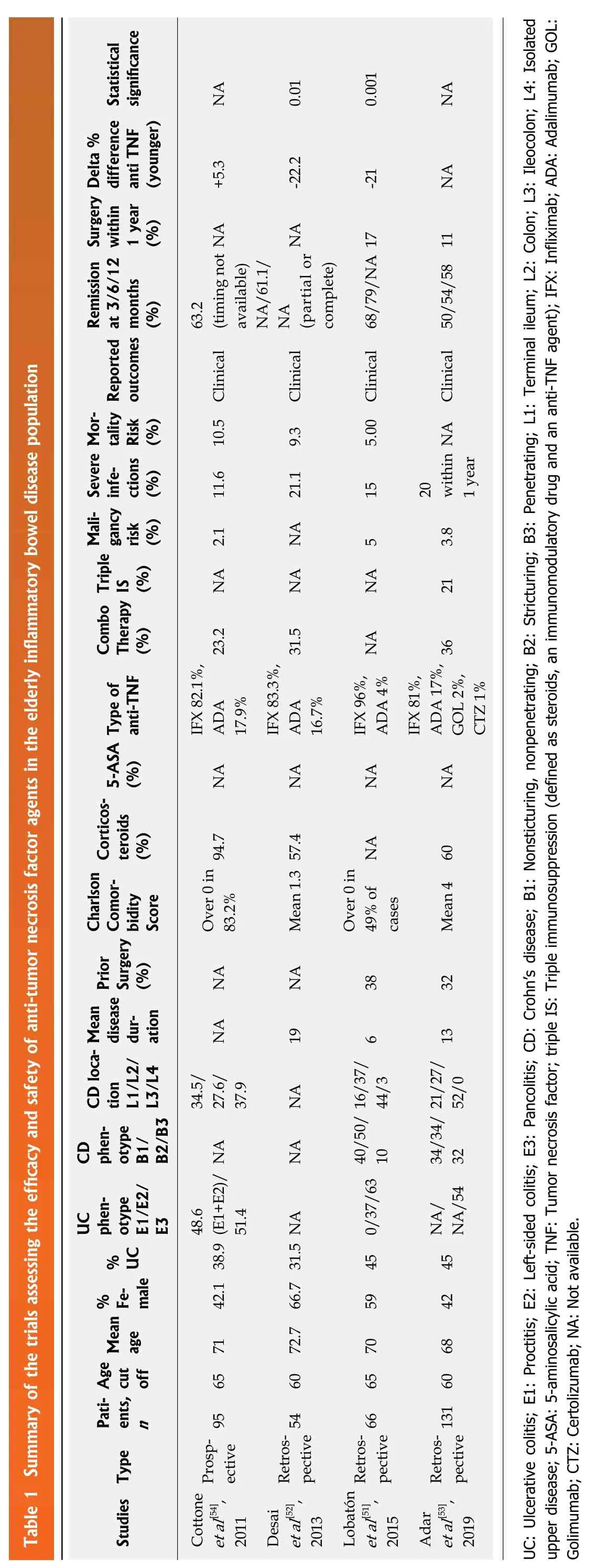
Table 1 Summary of the trials assessing the efficacy and safety of anti-tumor necrosis factor agents in the elderly inflammatory bowel disease population Statistical significance NA 0.01 0.001 NA Delta %Surgery difference anti TNF(younger)+5.3-22.2-21 NA within 1 year(%)NA NA Remission at 3/6/12 months(%)63.2(timing not available)NA/61.1/NA (partial or complete)Mor-Reported outcomes Clinical Severe tality Risk(%)10.5 Clinical 9.3 5.00 Clinical 68/79/NA 17 NA Clinical 50/54/58 11 infections(%)11.6 21.1 15 20 within 1 year Maligancy risk(%)2.1 NA 5 3.8 Triple IS (%)NA NA NA 21 Combo Therapy(%)23.2 31.5 36 Type of anti-TNF IFX 82.1%,ADA 17.9%IFX 83.3%,ADA 16.7%IFX 96%,ADA 4% NA IFX 81%,ADA 17%,GOL 2%,CTZ 1%5-ASA(%)NA NA NA NA Corticosteroids(%)94.7 NA Charlson Comorbidity Score Over 0 in 83.2%Mean 1.3 57.4 Over 0 in 49% of cases Mean 4 60 Prior Surgery(%)NA NA 38 32 Mean CD locadisease duration NA 19 6 13 tion L1/L2/L3/L4 34.5/27.6/37.9 NA 16/37/44/3 21/27/52/0 CD phenotype B1/B2/B3 NA NA 10 34/34/32 UCphenotype E1/E2/E3 48.6(E1+E2)/51.4 NA/54% UC 45 0/37/63 40/50/45 NA/% Female 42.1 38.9 59 42 Mean age Age Paticut ents,off 65 71 60 72.7 66.7 31.5 NA 65 70 n Studies Type Prospective 95 Retrospective 54 Retrospective 66 Retrospective 131 60 68 Cottone et al[54],2011 Desai et al[52],2013 Lobatón et al[51],2015 Adar et al[53],2019 UC: Ulcerative colitis; E1: Proctitis; E2: Left-sided colitis; E3: Pancolitis; CD: Crohn’s disease; B1: Nonsticturing, nonpenetrating; B2: Stricturing; B3: Penetrating; L1: Terminal ileum; L2: Colon; L3: Ileocolon; L4: Isolated upper disease; 5-ASA: 5-aminosalicylic acid; TNF: Tumor necrosis factor; triple IS: Triple immunosuppression (defined as steroids, an immunomodulatory drug and an anti-TNF agent); IFX: Infliximab; ADA: Adalimumab; GOL:Golimumab; CTZ: Certolizumab; NA: Not available.

Table 2 Summary of the trials assessing the efficacy and safety of vedolizumab in the elderly inflammatory bowel disease population Malignancy risk (%)NA 0 2 Surgery Infectious risk (%)14 77 (any)vs 0.9(serious)17(significant infections)within 1 year(%)NA 10 Remission at 3-6-12 months (%)38/NA/41 10.3 41.8/IS (%) Outcomes NA/40.7 38/45/54 Clinical Clinical Clinical Triple NA 12.5 23 Combo Therapy(%)NA 17.4 33 Corticosteroids(%)NA 36.5 70 Charlson Comorbidity Score NA NA 4 Prior Surgery(%)NA 57 for CD 31 Prior anti-TNF use(%)69 51.6 60 Mean dis-ease duration 16 CD location L1/L2/L3 (%)21/79(L2+L3) NA 29/36/35 12.1 20/24/56/0 CD phen-UC phenotype B1/B2/B3 (%)43/25/32 otype E1/E2/E3 (%)0/20/80 NA 11/48/41 NA NA/NA/55% Female % UC 34 49.5 50 58 40 42 Mean age 67 61.7 68 Age cutoff 60 55 60 Patients,n Type Retrospective 29 Retrospective 112 Retrospective 103 Vedolizumab trials Navaneethan et al[69], 2017 Yajnik et al[59], 2017 Adar et al[53], 2019 UC: Ulcerative colitis; E1: Proctitis; E2: Left-sided colitis; E3: Pancolitis; CD: Crohn’s disease; B1: Nonsticturing, nonpenetrating; B2: Stricturing; B3: Penetrating; L1: Terminal ileum; L2: Colon; L3: Ileocolon; L4: Isolated upper disease; TNF: Tumor necrosis factor; triple IS: Triple immunosuppression (defined as steroids, immunomodulatory drug and vedolizumab); NA: Not available.
SURGERY
Advanced age confers an increased risk of post-operative morbidity and mortality,mostly driven by the number of comorbidities, especially renal disease (OR = 8.15 95%CI: 5.44-14.05), congestive heart failure (OR = 3.5, 95%CI: 2.63-4.62), thromboembolic disease (OR = 4.19, 85%CI: 3.37-5.21) and liver disease (respective ORs= 8.15, 95%CI: 5.44-14.05)[62].
Elderly patients require surgical interventions more commonly than the nonelderly, most of these happening within the first year of diagnosis. Either their disease will be refractory to medical therapy, or the treating physician has chosen an alternative to chronic immunosuppression due to the potentially higher rates of infections and malignancy or the inconveniences related to parenteral delivery of biologic agents. In Everhov et al[2], 13% of elderly IBD patients (22% in CD, 6% in UC)had undergone bowel surgery at 5 years, significantly higher than the 10% adult population (16% in CD, 5% in UC). Similarly higher rates of surgery in the elderly UC population were reported in a meta-analysis of 43 studies by Ananthakrishnan et al[63](OR = 1.36; 95%CI: 1.18-1.57), compared to similar rates in the elderly CD population(OR = 0.70; 95%CI: 0.4-1.22). Cumulative risk of colectomy in elderly UC patients is considered higher in distal and extensive UC (P values 0.04 and 0.0001, respectively),compared to younger populations[2].
Restorative proctocolectomy with ileal pouch-anal anastomososis (IPAA) and proctocolectomy with ileostomy are two commonly-used surgical interventions in the care of UC. Multiple trials have shown comparable short-term morbidity and mortality between both procedures in the elderly population, similar to the younger population[64-65]. Significantly higher rates of re-admission were seen in the IPAA group (55% vs 24%, P = 0.02), mostly due to dehydration from high ostomy output[66].Historically, IPAA was avoided in the elderly population due to perceived higher rates of fecal incontinence. IPAA is currently increasingly used in autonomous elderly patients with a subjectively-measured intact anal sphincter. This is largely due to a growing body of evidence which suggests no difference in daytime or nocturnal incontinence after three years of follow-up (3.8% vs 2.5% or 7.7% vs 2.5%, nonstatistically significant in a population ≥ 70 years old)[67]. Otherwise, IPAA in the elderly population are associated with similar rates of pouchitis and chronic pouch disorder, as well as high rates of sustained patient satisfaction and perceived quality of life[68].
For CD-related complications, such as stricturoplasty or abscess drainage,therapeutic approach should be similar in elderly and adult populations[4]. Data remains conflicting in terms of the rates of postoperative recurrence of CD in the elderly population, compared to the younger population. Prophylaxis of postoperative recurrence has not been studied in elderly CD patients.
CONCLUSION
Over the last few decades, the prevalence of IBD in the elderly has been steadily rising. An increasing number of adult-onset IBD patients are living past 60 years old.Earlier age at diagnosis and longer disease duration have translated into an increased risk of disease progression and immunosuppressive drug exposure in these patients.On the other end of the spectrum, elderly-onset IBD patients present as predominantly-colonic disease, mostly left-sided colitis in UC, as well as exhibiting lower rates of penetrating disease in CD. More recent, population-based trials have shown statistically higher utilization of steroids in the elderly population, compared to their younger counterparts, despite well-established toxicities. Biologic agents are seldom used in the elderly IBD population, owing to the higher infectious risks reported for anti-TNF agents and to the limited existing data regarding vedolizumab and ustekinumab. Anti-TNF have been shown to be effective but potentially lead to higher infectious and malignancy risks. Relative risk of serious infections due to recurrent corticosteroid use vs anti-TNF agents has not been directly compared strictly in the elderly IBD population. Vedolizumab may be a safe alternative in the elderly IBD population although supported by small, underpowered trials. Trials assessing IBDrelated surgical interventions have shown comparable short- and long-term morbidity and mortality compared to the younger population, highlighting a potential alternative to systemic immunosuppression. More prospective data is required to better define the efficacy and safety of biologic treatment for elderly IBD patients.
杂志排行

World Journal of Gastroenterology的其它文章
- Exhaled breath analysis in hepatology: State-of-the-art and perspectives
- Miniature gastrointestinal endoscopy: Now and the future
- Issues and controversies in esophageal inlet patch
- Role of hepatocyte nuclear factor 4-alpha in gastrointestinal and liver diseases
- G protein-coupled estrogen receptor in colon function, immune regulation and carcinogenesis
- Helicobacter pylori and cytokine gene variants as predictors of premalignant gastric lesions