Exhaled breath analysis in hepatology: State-of-the-art and perspectives
2019-08-26AntonioDeVincentisUmbertoVespasianiGentilucciAnnaSabatiniRaffaeleAntonelliIncalziAntonioPicardi
Antonio De Vincentis, Umberto Vespasiani-Gentilucci, Anna Sabatini, Raffaele Antonelli-Incalzi,Antonio Picardi
Abstract Liver disease is characterized by breath exhalation of peculiar volatile organic compounds (VOCs). Thanks to the availability of sensitive technologies for breath analysis, this empiric approach has recently gained increasing attention in the context of hepatology, following the good results obtained in other fields of medicine. After the first studies that led to the identification of selected VOCs for pathophysiological purposes, subsequent research has progressively turned towards the comprehensive assessment of exhaled breath for potential clinical application. Specific VOC patterns were found to discriminate subjects with liver cirrhosis, to rate disease severity, and, eventually, to forecast adverse clinical outcomes even beyond existing scores. Preliminary results suggest that breath analysis could be useful also for detecting and staging hepatic encephalopathy and for predicting steatohepatitis in patients with nonalcoholic fatty liver disease.However, clinical translation is still hampered by a number of methodological limitations, including the lack of standardization and the consequent poor comparability between studies and the absence of external validation of obtained results. Given the low-cost and easy execution at bedside of the new technologies(e-nose), larger and well-structured studies are expected in order to provide the adequate level of evidence to support VOC analysis in clinical practice.
Key words: Exhaled breath analysis; Electronic nose; Gas chromatography; Breath print;Liver cirrhosis; Nonalcoholic fatty liver disease; Hepatic encephalopathy
INTRODUCTION
Liver disease is well-known to be accompanied and clinically characterized by the exhalation of peculiar volatile organic compounds (VOCs). In ancient times, the typical musty breath aroma, termed fetor hepaticus, was among the most important clinical signs that physicians considered for diagnosis of liver insufficiency. In more recent years, this empiric approach has been supported by stronger evidence, thanks to the availability of sensitive technologies that have made exhaled breath analysis possible and reproducible on a large scale. VOCs are chemical intermediates generated by cellular metabolism and cleared from tissues and blood through the lungs. Several hepatic metabolic processes may be deranged during the course of chronic liver disease (CLD) and lead to the production and accumulation of various VOCs. Many of them can be odorless or be present in concentrations considerably below human sensorial threshold.
These compounds can be studied using different analytical techniques that are based on gas-chromatography and mass-spectrometry, which allow determining the exact concentration of a large spectrum of VOCs. Thus, these techniques are very useful to clarify biochemical underpinnings of diseases. However, this quantitative breath analysis can hardly provide a set of disease-specific compounds and is limited by a list of technical needs and high costs, making it suboptimal for breath profiling for diagnostic and prognostic purposes in the clinical practice. Conversely, the newer electronic (e-)nose technologies, which are based on the organization of gas sensors into arrays (i.e. gas sensor arrays), have been recently introduced for breath analysis.Although they cannot identify the chemical structure and concentration of each VOC,they provide a qualitative and semi-quantitative profile of the hundreds of VOCs (a sort of fingerprint of exhaled breath, breath-print) that can be associated with selected conditions by pattern recognition. This process mimics the “combinatorial selectivity”that enables natural olfaction to distinguish multiple different odors (Figure 1). A number of existing e-noses are already available[1-4], and this approach has been applied with good results in different clinical contexts[5-7], including the field of hepatology.
The aim of this article is to present the bulk of available studies in which the exhaled breath has been explored in patients with CLD. Starting from work initially focused on the description of VOCs for pathophysiological purposes, more recent research has progressively turned towards the comprehensive assessment of exhaled breath for potential clinical application. The state-of-the-art will be presented, along with a critical discussion of relevant data and perspectives of breath analysis in the field of hepatology.
STUDY ANALYSIS AND DISCUSSION
The pertinent studies were retrieved from MEDLINE using the following search terms: [(exhaled breath analysis OR electronic nose) AND (liver disease OR liver cirrhosis)]. Only English-language studies were considered. To identify additional studies, manual searching of bibliographies from gathered articles and reviews was also performed. Case reports, letters to editor, and commentaries, when adding relevant information, were also considered.
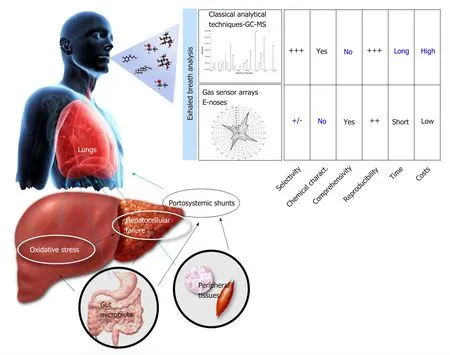
Figure 1 Schematic representation of volatile organic compounds origin in chronic liver disease and of the main technologies for exhaled breath analysis.Many pathophysiological processes can be altered during the course of chronic liver disease, leading to the production of specific VOCs. Oxidative stress secondary to hepatic inflammation can induce the production of many derivatives of cell membranes peroxidation. With advancing liver fibrosis, other VOCs sources can be represented by many other metabolic pathways that can be deranged with progressive hepatocellular failure. Peculiar VOCs also derive from the gut microbiome or directly from peripheral tissues, bypassing the liver through portosystemic shunts, typical of liver cirrhosis. After exhaled through the breath, VOCs can be sampled,pre-concentrated and stored thanks to dedicated procedures that have been detailed elsewhere[6]. Then, exhaled breath analysis can be carried out through different techniques: (1) The classical analytic techniques based on GC-MS; (2) The gas sensor arrays, commonly dubbed e-noses. Each method has its own pros and cons.Analytical techniques have the advantage of exactly identifying the chemical structure of VOCs, but they are expensive and require long time and high economic resources to be performed on large scale. Conversely, e-noses are portable, cheaper, and easier to perform even in elderly and disabled patients but are less selective and cannot identify the chemical structure of each VOC. Given their different features, each technique is preferable in different research or clinical scenarios,as explained in the text. GC-MS: Gas chromatography and mass spectrometry; VOCs: Volatile organic compounds.
The first works date back to 1970, when Chen et al[8]examined the exhaled breath of two independent groups of 13 and 15 patients with liver cirrhosis (LC), evidencing increased levels of sulfur compounds (such as mercaptans) and volatile aliphatic acids(mainly acetic and propionic acid)[9]. These findings were then confirmed by additional studies[10-16], which further extended this list to nitrogen compounds,various aliphatic acids, alkanes, alkenes, terpenes, ketones, and alcoholic derivatives.Dimethylsulfide was finally identified as the main compound responsible for fetor hepaticus[12]. The exact origin of all these molecules was barely explored, but many pathophysiological speculations linking them with different types of liver disease have been hypothesized involving a wide range of metabolic and inflammatory derangements (presented in Table 1).
Table 2 summarizes the discriminative performances of exhaled breath analysis with respect to the characterization of CLD patients. Van den Velde et al[17]analyzed the breath of 52 patients with established LC. Using gas chromatography mass spectrometry (GC-MS) techniques, they found that dimethylsulfide, acetone, 2-pentanone, and 2-butanone were significantly increased in LC and firstly showed the quite good discriminative capacities of a set of VOCs to distinguish patients with LC from healthy subjects (sensitivity of 100% and specificity of 70%). Subsequently, other studies replicated this finding[18-25], further highlighting the capability of exhaled breath analysis to discriminate LC also from non-cirrhotic CLD[24,25]. Interestingly, a set of 11 VOCs discriminated LC significantly better than five serological markers[alanine aminotransferase (ALT), gamma-glutamyl transferase, bilirubin, albumin and platelets], which are commonly used in clinical practice for this purpose[24].
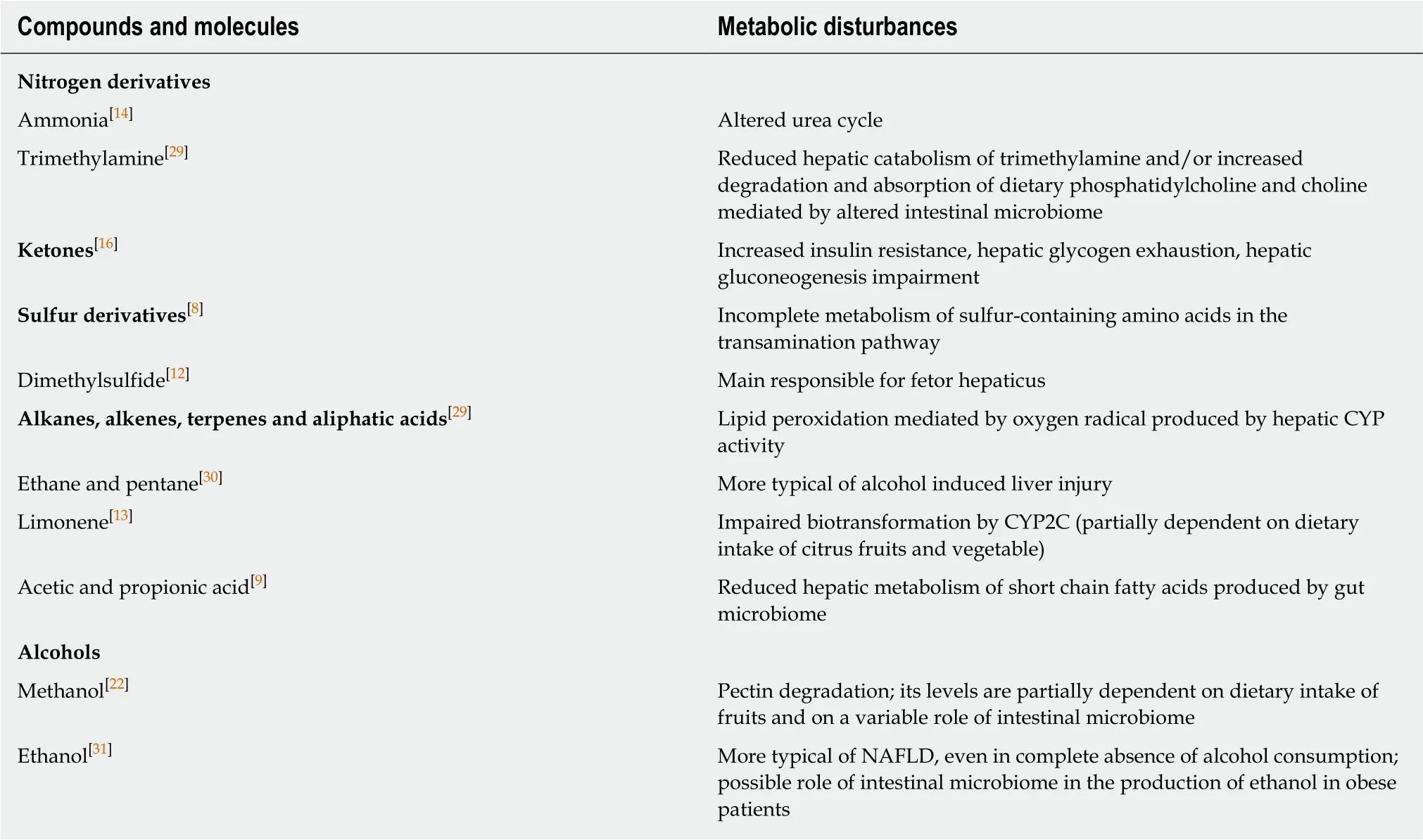
Table 1 Summary of the main volatile organic compounds found in the exhaled breath of patients with liver cirrhosis
Sub-analysis including only patients with LC was carried out in two cases[22,25]. In the first study, exhaled breath analysis correctly classified subjects with decompensated LC in 92% of the cases[22]. In the second one, a lower accuracy of 70%was found, while end-stage liver disease was predicted with a sensitivity of 88% and a specificity of 64%[25]. These results suggest selected VOC patterns to characterize LC through their patterns changing along with the progressive hepatocellular failure, as represented by Child-Pugh classes (CPC). Although most of these works were crosssectional, their findings have been recently substantiated by a prospective study in which specific VOCs breath-prints by e-nose were found to predict hospitalization and death of patients with LC even in multiple adjusted models[26]. These associations,independent also of CPC and Model for End-stage of Liver Disease score, suggest that, in the context of LC, the exhaled breath profile may add relevant prognostic information that is not properly captured by the available tools.
On the other hand, limited data are available on the diagnosis and grading of hepatic encephalopathy (HE) by exhaled breath. Khalid et al[21]firstly evidenced 13 VOCS to predict HE with an accuracy of 88% in 33 subjects with alcoholic LC. Later on, Arasaradnam et al[27]confirmed an accuracy of 84% in a wider cohort. Overall,exhaled breath analysis was found to identify patients with HE with respect to healthy controls with sensitivity ranging 88%-91% and specificity ranging 73%-87%[21,27]; however, the only study comparing overt and covert HE in LC patients found a significantly lower diagnostic accuracy (sensitivity of 79%, specificity of 50%,and area under the curve of 0.71)[27]. It is plausible that the broad metabolic derangements underlying the great clinical heterogeneity of HE (minimal, episodic,recurrent, and persistent) accounts for the heterogeneous VOC patterns and also for poor discriminatory potential of exhaled breath analysis within HE patients.
Similarly, exhaled breath analysis cannot be used with confidence for discrimination of liver diseases from different etiologies. A large study, including patients with infective, alcoholic, and metabolic liver diseases, reported a very poor sensitivity (29%) for the discrimination of infective etiology[25]. Another work, carried out on a much more limited sample, evidenced an accuracy of 65% for the detection of the alcoholic etiology of liver disease[21].
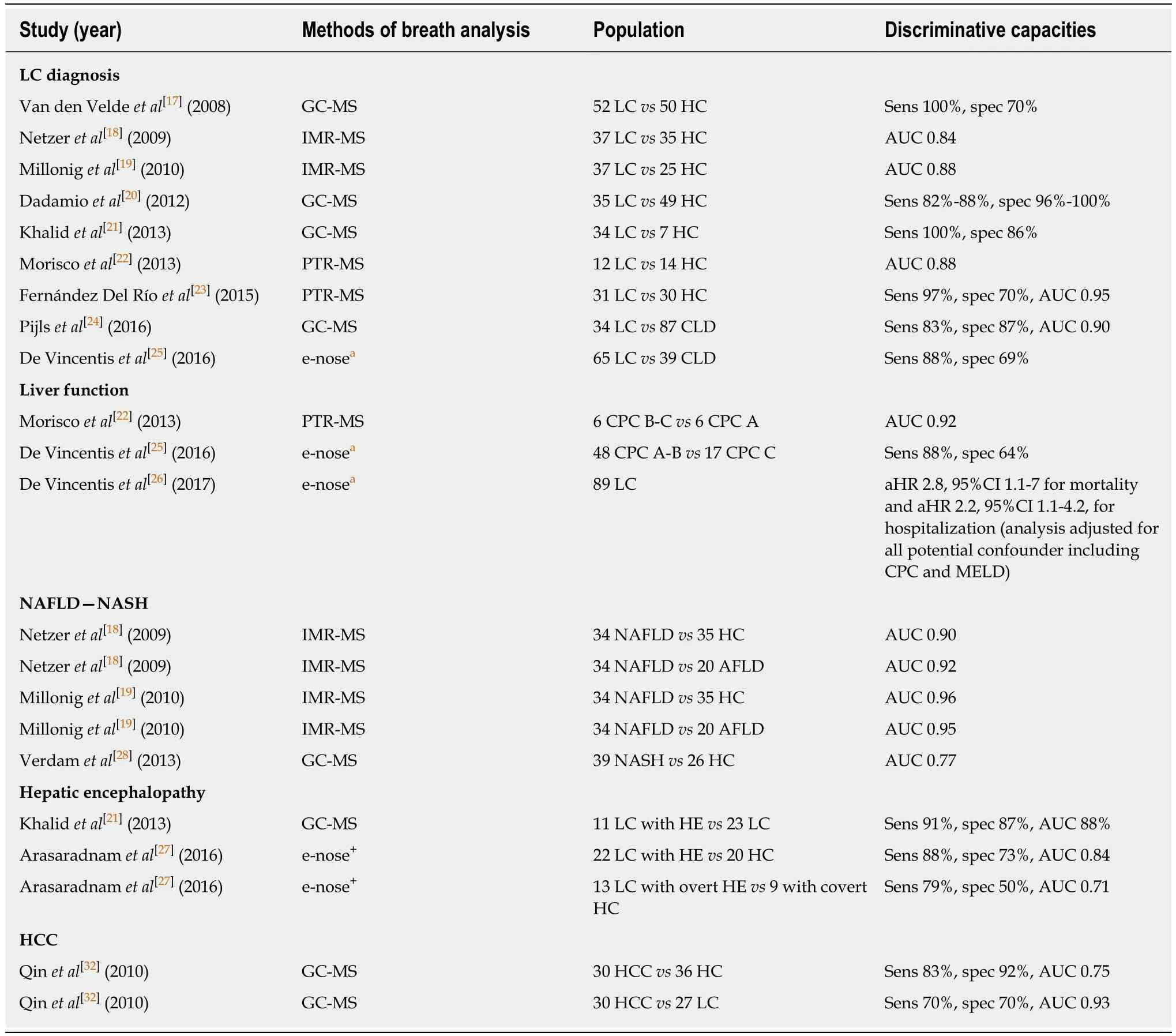
Table 2 Discriminative capacities of exhaled breath analysis for clinically relevant applications in hepatology
In apparent contrast with these results, nonalcoholic fatty liver disease (NAFLD)seemed to retain a more distinctive breath pattern. In a cohort of 89 subjects, patients with NAFLD were correctly discriminated from healthy subjects in 90% of the cases and from patients with alcoholic liver disease in 92% of the cases[18]. A subsequent similar study reported even higher accuracies (96% and 95%, respectively, for the same comparisons)[19]. Moreover, three VOCs (an alcohol, an alkane, and a nitrogen derivate) were shown to detect nonalcoholic steatohepatitis (NASH)-defined by liver histology- with an accuracy of 77%, which was higher than those observed for other non-invasive biomarkers (e.g., elevated serum ALT or the aspartate aminotransferase to ALT ratio)[28]. The application of breath analysis reduced the proportion of undiagnosed cases from 67%-79% to 10% and that of misdiagnosed cases from 49%-51% to 18%[28].
Overall, despite encouraging results, some limitations seem to arise from the critical appraisal of all the above-mentioned studies. First of all, in the great majority of studies, VOC profiles of patients with CLD were compared to healthy controls rather than to the more appropriate control population. Indeed, it would be more sensible to compare patients with LC to those with non-cirrhotic CLD and patients with HE to patients with LC without HE. Moreover, study cohorts were often limited in numerosity, and subjects were generally free from significant comorbidities,thereby being not particularly representative of the real-life setting. Indeed, when larger populations with a greater burden of coexisting diseases were analyzed[24,25],slightly worse results were obtained.
Except for one study[28], the stage of hepatic fibrosis was not determined through the gold standard method (i.e. liver biopsy). Therefore, we lack data on the relation between VOCs and hepatic inflammatory activity as well as on the VOCs pattern in the different stages of liver fibrosis that precedes LC. Worthy of comment is also the fact that classical analytical GC-MS techniques have been applied in the majority of these works, while the e-nose technologies have been recently tested in two studies[25,26]following the good results obtained in respiratory diseases[6]. Both methods have their own limitations (Figure 1). GC-MS is expensive, is difficult to execute at bedside, and can hardly detect a set of disease specific VOCs; conversely, enose is poorly selective and cannot identify the chemical structure of selected VOCs.Hence, this great methodological heterogeneity, as well as the lack of external validation of findings obtained by each study, and the differences by which data was statistically analyzed and reported, weakens the overall relevance of these studies and make them barely comparable.
FUTURE PERSPECTIVES AND CONCLUSIONS
Potential applications of exhaled breath analysis in patients with liver disease seem to emerge from the bulk of currently available studies and deserve particular consideration. Staging CLD and diagnosing LC are actually achieved either through the physician’s judgment based on different clinical, biochemical, or ultrasound data or by means of liver biopsy, which still represents the gold standard. The former is susceptible to poor accuracy, while the latter is invasive and expensive, hence, not feasible on large scale. Newer non-invasive methods based on clinical scores or elastographic techniques have been recently introduced to overcome these limitations,but their diagnostic performance seems unsatisfactory in selected disease scenarios(e.g., in obese and NAFLD subjects). In this context, exhaled breath analysis could serve as an adjunctive tool to refine diagnosis. In addition, VOCs could qualify as indicators of disease severity and prognosis in patients with LC. In fact, different degrees of liver failure are known to be accompanied by several inflammatory and metabolic derangements, which could be mirrored by different VOC patterns and interpreted for risk stratification. This could be particularly relevant, because,although retaining the strongest prognostic information, available scores (i.e. CPC and Model for End-stage of Liver Disease score) can only moderately capture the great phenotypical variability, which is typical of advanced liver disease. A major contribution to this variability is conferred by the onset of HE, which is among the most invalidating complications of LC with a major impact on health status and quality of life, possibly presenting with a various blend of cognitive, behavioral, and motor function alterations. To date, its diagnosis and classification is based on clinical criteria (West-Haven criteria) and subject to high interobserver variability, and its predictors have not been fully clarified. VOCs might complement the evaluation of patients with HE in order to allow a more effective approach in the diagnostic and prognostic phase. Similarly, VOCs could help in the context of NAFLD for the detection of NASH, which is currently achievable only by performing a liver biopsy.Hence, non-invasive alternatives would be eagerly welcomed.
Despite these perspectives, the clinical significance of exhaled breath analysis in hepatology is still hindered by the absence of a sufficient strength of evidence allowing definitive conclusions. Indeed, larger studies providing a better characterization of patients in terms of liver fibrosis and of comorbidities (e.g., diabetes mellitus, obesity, dyslipidemia, chronic kidney disease) and more representative of real life populations are now needed. These studies are expected to validate the observed discriminative capacities in external cohorts, clarifying the impact of coexistent diseases, which might per se influence VOCs, on disease-specific breath patterns. Aside from better investigating their discriminative capabilities, longitudinal studies should determine whether VOCs could also reliably predict LC patients at increased risk of developing overt episodes of HE within a short period. This property would be clearly invaluable, since HE severely affects the quality of life of patients and their caregivers. Individuating those patients at higher risk of HE could allow for tailoring of individualized prophylactic strategies aimed at improving patients’ safety and social and working related activities.
An associated issue concerns the standardization of exhaled breath analysis techniques. If the intention is to promote an application in clinical practice, cheaper and quicker devices (such as e-noses) should be preferred. In addition, their easy execution at bedside or also at patients’ home makes them particularly suitable for elderly, disabled, and more comorbid subjects (see Figure 1). Conversely, “classical”analytical techniques, based on GC-MS, should be limited only to studies aiming at raising our pathophysiological understanding of the underlying mechanisms in hepatopathies.
In conclusion, exhaled breath analysis could be successfully applied for detecting and monitoring the course of liver diseases only after its diagnostic, classificatory, and predictive properties are comprehensively defined. Efforts should be directed towards the enrollment of better characterized cohorts of patients in larger cooperative and prospective studies, providing adequate outcome specific follow-up periods. An increasing awareness of the potentialities of this technique is eagerly awaited in order to stimulate future research in this field and involve other research groups.
杂志排行

World Journal of Gastroenterology的其它文章
- Miniature gastrointestinal endoscopy: Now and the future
- Issues and controversies in esophageal inlet patch
- Role of hepatocyte nuclear factor 4-alpha in gastrointestinal and liver diseases
- G protein-coupled estrogen receptor in colon function, immune regulation and carcinogenesis
- Helicobacter pylori and cytokine gene variants as predictors of premalignant gastric lesions
- Intestinal enteroids/organoids: A novel platform for drug discovery in inflammatory bowel diseases