Risk factors for local recurrence and appropriate surveillance interval after endoscopic resection
2019-04-15YoriakiKomedaTomohiroWatanabeToshiharuSakuraiMasashiKonoKazukiOkamotoTomoyukiNagaiMamoruTakenakaSatoruHagiwaraShigenagaMatsuiNaoshiNishidaNaokoTsujiHiroshiKashidaMasatoshiKudo
Yoriaki Komeda, Tomohiro Watanabe, Toshiharu Sakurai, Masashi Kono, Kazuki Okamoto, Tomoyuki Nagai,Mamoru Takenaka, Satoru Hagiwara, Shigenaga Matsui, Naoshi Nishida, Naoko Tsuji, Hiroshi Kashida,Masatoshi Kudo
Yoriaki Komeda, Tomohiro Watanabe, Toshiharu Sakurai, Masashi Kono, Kazuki Okamoto,
Tomoyuki Nagai, Mamoru Takenaka, Satoru Hagiwara, Shigenaga Matsui, Naoshi Nishida, Naoko Tsuji, Hiroshi Kashida, Masatoshi Kudo, Department of Gastroenterology and Hepatology,Kindai University Faculty of Medicine, Osaka 589-8511, Japan
Corresponding author: Yoriaki Komeda, MD, PhD, Assistant Professor, Department of Gastroenterology and Hepatology, Kindai University Faculty of Medicine, 377-2 Ohno-Higashi, Osaka-Sayama, Osaka 589-8511, Japan. y-komme@mvb.biglobe.ne.jp
Abstract BACKGROUND Risk factors for local recurrence after polypectomy, endoscopic mucosal resection(EMR), and endoscopic submucosal dissection (ESD) have not been identified.Additionally, the appropriate interval for endoscopic surveillance of colorectal tumors at high-risk of local recurrence has not been established.AIM To clarify the clinicopathological characteristics of recurrent lesions after endoscopic colorectal tumor resection and determine the appropriate interval.METHODS Three hundred and sixty patients (1412 colorectal tumors) who underwent polypectomy, EMR, or ESD and received endoscopic surveillance subsequently for more than one year to detect local recurrence were enrolled in this study. The clinicopathological factors associated with local recurrence were determined via univariate and multivariate analyses.RESULTS Local recurrence was observed in 31 of 360 (8.6%) patients [31 of 1412 (2.2%)lesions] after colorectal tumor resection. Piecemeal resection, tumor size of more than 2 cm, and the presence of villous components were associated with colorectal tumor recurrence after endoscopic resection. Of these three factors, the piecemeal resection procedure was identified as an independent risk factor for recurrence. Colorectal tumors resected into more than five pieces were associated with a high risk of recurrence since the average period from resection to recurrence in these cases was approximately 3 mo. The period to recurrence in cases resected into more than 5 pieces was much shorter than that in those resected into less than 4 pieces (3.8 ± 1.9 mo vs 7.9 ± 5.0 mo, P<0.05).CONCLUSION Local recurrence of endoscopically treated colorectal tumors depends upon the outcome of first endoscopic procedure. Piecemeal resection was the only significant risk factor associated with local recurrence after endoscopic resection.
Key words: Local recurrence; Colorectal tumor; Endoscopic surveillance; Piecemeal resection; Risk factors
INTRODUCTION
Colorectal cancer (CRC) is one of the leading causes of cancer-related deaths in both Western and Asian countries[1-3]. It is now generally accepted that most, if not all,CRCs arise from adenomas[4]. Based on this notion called the “adenoma-carcinoma sequence”, colorectal adenomas are considered the precursor lesions of CRCs. Thus,their endoscopic removal is strongly recommended for the prevention of CRCs[5].Several reports provide evidence that adenoma removal reduces the incidence of CRC and thereby improves patient survival[4,6]. Currently, three types of endoscopic techniques are performed for the resection of colorectal tumors; these are polypectomy,endoscopic mucosal resection (EMR), and endoscopic submucosal dissection(ESD)[7-12]. The introduction of ESD, which allowsen blocresection of flat or depressed colorectal tumors of more than 20 mm, has enabled endoscopists to remove adenomas as well as to remove early CRCs[13]. Thus, a wide variety of colorectal tumors,including adenomas and early CRCs, can be endoscopically resected using a selection of polypectomy, EMR, and ESD depending on the size and macroscopy of the tumors.
As the indication for endoscopic colorectal tumor resection has expanded in terms of tumor size and depth of tumor invasion, it has become apparent that local recurrence occurs in a significant proportion of patients treatedviapolypectomy,EMR, or ESD[14]. According to a previous meta-analysis, a high incidence of local recurrence of up to 50% after EMR has been reported[15]. Although tumor size, intraprocedural bleeding, piecemeal resection, and high-grade dysplasia have been shown to be associated with local recurrence of colorectal adenoma after EMR[16], the related risk factors after polypectomy, EMR, and ESD have not been identified. Additionally,the appropriate interval of endoscopic surveillance for colorectal tumors with a high risk of local recurrence has not been established, although the American Cancer Society recommends an interval of 3 to 6 mo for follow-up endoscopic examinations after piecemeal resection for large or sessile polyps[17]. In this retrospective study, we attempted to clarify the clinicopathological characteristics of recurrent lesions after endoscopic colorectal tumor resection and propose the appropriate follow-up interval of colonoscopic surveillance.
MATERIALS AND METHODS
Patients
A total of 1020 patients underwent polypectomy, EMR, or ESD for 4236 lesions at Kindai University Hospital from January 2010 to December 2015. Among these patients, 360 patients (1412 lesions) received endoscopic surveillance for local recurrence for more than one year. Various factors associated with local recurrence after endoscopic resection was retrospectively analyzed in these patients. The factors used for the analysis included age, sex, past history of CRC, diabetes, macroscopic tumor type, tumor size and location, resection methods, number of adenomas, and histology. Although most previous reports[14-17]successfully identified lesional factors associated with the local recurrence of colonic tumors after endoscopic treatments,such as tumor sizes, endoscopic findings, and tumor locations, few reports have tried to identify patient factors, such as age, sex, history of colonic tumors, and diabetes. In this study, we performed univariate and multivariate analysis to identify patient factors associated with local recurrence. To this end, the largest tumor in size was selected in each patient for the analysis when more than 2 polyps are detected.Moreover, the most advanced type of histology was selected in each patient when more than 2 polyps were removed. Pathological diagnosis of the colorectal tumors was performed by experienced pathologists as described previously[18]. Cases diagnosed as intra-mucosal carcinoma by Japanese pathologists were categorized into high-grade dysplasia as described previously[19]. Invasive cancer was defined as invasion beyond the muscularis propria. Polypectomy, EMR, and ESD were performed for 157, 1130, and 125 colorectal tumors, respectively. Patients with inflammatory bowel disease or polyposis were excluded from the study. Ethical permission for this study was granted by the review board of Kindai University Faculty of Medicine (approval number: 30-157).
Endoscopic procedures
Polypectomy and EMR were performed as previously described by Komedaet al[20]and ESD was performed as previously described by Okamotoet al[18]. In our institute,the basic strategy for endoscopic resection isen blocresection; piecemeal resection is avoided as much as possible. We performed ESD for colorectal tumors of the flat or depressed type when EMR may result in piecemeal resection. The patients'endoscopic and medical records were retrospectively analyzed. The procedures followed were in accordance with the guidelines of the World Medical Association's Declaration of Helsinki.
Statistical analysis
Imputed data were statistically assessed using SPSS version 12.0 for Windows (SPSS Inc, Chicago, IL, United States). Odds ratios and 95% confidence intervals (95%CI)were evaluated for each category of variable indicators, including age, sex, past history of CRC, diabetes, macroscopic tumor type, tumor size, tumor location,resection method, number of adenomas, and histology. The statistical significance of the differences between the two groups was determinedviaStudent'st-test. A probability value of 0.05 or less was considered significant.
RESULTS
Incidence of local recurrence and location of recurrent lesions
Local recurrence was observed in 31/360 (8.6%) patients who received endoscopic surveillance for more than one year after colorectal tumor resection. The median observation period was 795 d. Of 31 patients included in the study, 24 and 7 were males and females, respectively. The locations of the recurrent lesions were distributed throughout the colorectum: 6, 9, 4, 2, 5, and 5 in the cecum, ascending colon, transverse colon, descending colon, sigmoid, and rectum, respectively.
Pathological characteristics of primary and recurrent colorectal tumors
The characteristics of primary and recurrent lesions are shown in Figure 1. The sizes of the lesions were 29.1 ± 21.6 mm and 8.1 ± 6.9 mm (mean ± standard error),respectively. Primary colorectal tumors comprised 17 low-grade adenomas, 13 highgrade adenomas, and one submucosal invasion cancer (T1). Pathological examinations of the initial recurrent lesions showed that 24, 5, and 2 cases were diagnosed as lowgrade adenoma, high-grade adenoma, and submucosal invasion cancer (T1),respectively. Intra-mucosal cancer was regarded as high-grade adenoma in accordance with previous reports[19]. Interestingly, 17 cases (70.8%) and 7 cases (29.2%)of recurrent low-grade adenoma arose from primary low-grade and high-grade adenomas, respectively. Five cases (100%) of recurrent high-grade adenomas originated from primary high-grade adenomas. Two cases of recurrent submucosal invasion cancer originated from one submucosal invasion cancer and one high-grade adenoma (Figures 2 and 3). These pathological findings strongly suggested that primary low-grade adenomas and submucosal invasion cancer manifest their recurrent lesions as primary pathological features. In contrast, primary high-grade adenomas may develop into a wide pathological variety of colorectal tumors, ranging from low-grade adenomas to submucosal invasion cancers.
Patient characteristics and recurrence of colorectal tumors
Having obtained the pathological relationship between primary and recurrent colorectal tumors, we attempted to identify the clinicopathological risk factors associated with recurrence using univariate analysis. As shown in Table 1, no significant correlation was observed between recurrence and age, sex, history of colorectal tumors, or diabetes mellitus.
Endoscopic procedures, macroscopic appearance of colorectal tumors, and tumor recurrence
Next, we examined whether the macroscopic appearance of tumors or the endoscopic procedures were associated with the recurrence of colorectal tumors. Analysis of the correlation between the endoscopic procedures and recurrence showed that all the patients who experienced recurrence (31 patients) were those in which a previous treatment resulted in piecemeal resection (25 patients, 80.6%, Table 1) or those who had a positive margin (6 patients, 19.4%). The 25 patients included 15 and 10 patients who underwent EMR and ESD, respectively. As shown in Table 2, the recurrence rate of colorectal tumors that were treatedviapiecemeal resection was much higher(25/63, 39.7%) than that of those treatedvia en blocresection (6/297, 2.0%). Of the 31 recurrent lesions, 30 lesions were successfully treated using endoscopy without complications and one lesion was surgically treated due to cancerous submucosal invasion. Regarding the recurrent colorectal tumors, owing to the much higher rate of piecemeal resection than ofen blocresection, piecemeal resection was identified as a risk factor for recurrence.
Subsequently, we focused on the relationship between the macroscopic appearance of colorectal tumors and recurrence. As shown in Table 2, the recurrence rate of colorectal tumors of more than 2 cm was much higher (20/121, 16.5%) than that of tumors of less than 2 cm (6/297, 4.6%).
In contrast, no significant correlation was identified between recurrence and the macroscopic appearance of colorectal tumors in terms of growth type: Laterally spreading tumor granular type (LST-G), LST-non granular type (LST-NG) IIa, IIc, Ip,and Is. Consistent with the high rate of previous piecemeal resection and the recurrent colorectal tumor size of more than 2 cm, univariate analysis identified piecemeal resection and tumor size of more than 2 cm as risk factors for recurrence.
Pathological features of the colorectal tumors and recurrence
We attempted to determine the relationship between the pathological features and recurrence of colorectal tumors. As shown in Table 1, neither the number of adenomas nor the pathological diagnosis of the tumors (low-grade adenoma, high-grade adenoma, and submucosal invasion cancer) was associated with tumor recurrence.Interestingly, the recurrence rate of colorectal tumors with villous components was much higher (6/27, 22.2%) than that of those without villous components (25/333,7.5%). Univariate analysis identified the presence of villous components as a risk factor for tumor recurrence.
Piecemeal resection and intervals of recurrence of the colorectal tumors
Having identified piecemeal resection, tumor size of more than 2 cm, and the presence of villous components as possible risk factors for the recurrence of endoscopically-treated colorectal tumors, we performed multivariate analysis. As shown in Table 2, the piecemeal resection technique was the only independent risk factor for colorectal tumor recurrence.
Table 3 shows the different types of techniques (polypectomy,en blocEMR,piecemeal EMR,en blocESD, and piecemeal ESD), and provides evidence that endoscopic procedures are associated with local recurrence. Piecemeal resection(piecemeal EMR, piecemeal ESD) had a clear and significant relationship with local recurrence compared toen blockresection. We also tried to confirm these results with another approach. As shown in Figure 4, we performed a sub-analysis to identify the types of techniques (polypectomy,en blocEMR, piecemeal EMR,en blocESD, and piecemeal ESD) associated with local recurrence. This analysis also showed clearly that piecemeal resection (piecemeal EMR, piecemeal ESD) was highly related to local recurrence compared toen blockresection.
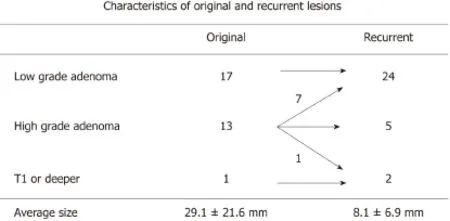
Figure 1 Pathological characteristics of primary and recurrent colorectal tumors. Most of the recurrent lesions were low grade adenoma.
Finding that piecemeal resection was the strongest risk factor for colorectal tumor recurrence prompted us to examine the recurrence periods from the initial endoscopic procedure. The average period between the initial resection and recurrence for all cases was 6.1 ± 4.5 mo (range, 2 to 15 mo). Table 4 summarizes the relationship between the number of resected pieces and the time to recurrence. The period from the initial endoscopic procedure to the recurrence of colorectal tumors resected into 2,3, and 4 pieces were 9.0 ± 3.8, 10.1 ± 6.3, and 5 mo, respectively. In contrast, the period to recurrence in the 13 cases resected into 5 or more pieces was 3.8 ± 1.9 mo. Thus, the period from the initial endoscopic procedure to the local recurrence for tumors resected into more than 5 pieces was very short. Therefore, such cases might require endoscopic surveillance soon after the initial endoscopic procedure.
DISCUSSION
In this study, we attempted to determine the risk factors associated with the recurrence of endoscopically-treated colorectal tumors. For this purpose, we analyzed 360 patients (1412 lesions) in a retrospective manner; the local recurrence rate was 31/360 (8.6%). Among a variety of factors including clinical characteristics,endoscopic procedure, and pathological features, univariate analysis identified piecemeal resection, tumor size of more than 2 cm, and the presence of villous tumor components as possible risk factors for recurrence. Further multivariate analysis identified piecemeal resection as an independent risk factor for recurrence. In this study, the recurrence rate of colorectal tumors treated using piecemeal resection was 39.7% and that of lesions beyond 2 cm in size was 16.5%. These data are in line with a recent report that showed that piecemeal resection is the important risk factor for local recurrence in colorectal tumors treatedviaEMR or ESD[21]. Moreover, our results are consistent with a recent meta-analysis that showed that recurrence varies from 10% to 55% after endoscopic piecemeal mucosal resection in tumors measuring more than 2 cm[15]. However, we need to be cautious in the comparison of our data with those obtained in Western countries due to the difference in endoscopic resection methods.In our facility, the strategy for endoscopic removal of colorectal tumors isen blocresectionviaESD; in contrast, wide-filed EMR rather than ESD is widely used in Western countries[22]. In any case, it is likely that tumors of more than 2 cm and piecemeal resection both increase the risk of local recurrence.
En blocresectionviathe ESD technique is recommended for the endoscopic resection of large colorectal tumors of more than 2 cm since accumulating evidence provides a reduced rate of local recurrence in patients treated using ESD[21]. However,colonic ESD does not always result inen blocresection in difficult situations such as bowel peristalsis, fibrosis in the submucosa, bleeding, or inexperience skill of the endoscopist[23-25]. In this study, 10 and 21 cases treated with ESD and EMR,respectively, exhibited local recurrence. Among the 21 cases, 15 tumors were resectedviathe piecemeal technique and 6 tumors had a positive resection margin. The 10 cases treatedviaESD were resected using piecemeal resection. Therefore, our study strongly suggests that piecemeal resection increases the risk of local colorectal tumor recurrence regardless of the endoscopic resection method employed.
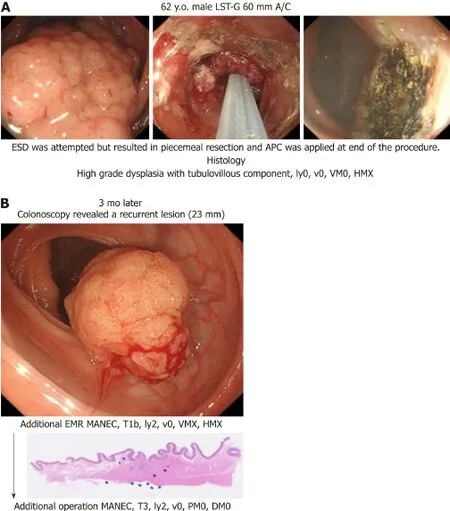
Figure 2 Endoscopic submucosal dissection was attempted for a lateral spreading tumor-granular measuring 60 mm and was located in the ascending colon. A: However, the surgery was converted to a piecemeal resection and argon plasma coagulation was performed at the end of the procedure. The tumor histology was tubulovillous adenoma and the horizontal margin was unclear; B: After 3 mo, colonoscopy revealed a recurrent lesion and thus additional endoscopic mucosal resection was performed. Surprisingly, the histological analysis revealed mixed adeno-endocrine carcinoma T1b with indistinct margins. Thereafter, additional surgery was performed. The final depth was T3 (sub-serosal). APC: Argon plasma coagulation; EMR: Endoscopic mucosal resection; ESD: Endoscopic submucosal dissection; MANEC: Mixed adeno-endocrine carcinoma; LST-G: Laterally spreading tumor granular type.
Colon adenomas with villous components are considered high-risk tumors with the ability to differentiate into CRC[26]. In fact, in this study, the rate of local recurrence was higher for colorectal adenomas bearing villous components. However, the presence of villous components in colon adenomas was not defined as an independent risk factor for recurrence in the multivariate analysis. Future prospective studies are necessary to determine whether the presence of villous components in colon adenomas increases the risk of recurrence after endoscopic treatment.
The identification of piecemeal resection as an independent risk factor for the recurrence of colorectal tumors led us to investigate the periods from the endoscopic resection to recurrence. Interestingly, the period to recurrence in cases resected into more than 5 pieces was much shorter than that in those resected into less than 4 pieces(3.8 ± 1.9 movs7.9 ± 5.0 mo,P<0.05). Thus, colorectal tumors endoscopically resected into more than 5 pieces bear a very high risk of recurrence within 3 mo post-resection while those resected into less than 4 pieces bear a high risk for recurrence within 8 mo. Consistent with these data, previous reports[11,14]provide the evidence that the recurrence rate is higher and the interval to recurrence tends to be shorter for colorectal tumors resected into more than 5 pieces. Our analysis of the periods from the initial endoscopic treatment to tumor recurrence prompts us to propose appropriate intervals for endoscopic surveillance. Because the period to recurrence in cases resected into 1 piece with unclear margin (incomplete margin) was 6.1 ± 4.5 months in this study, surveillance endoscopy needed to be performed within 1 to 3 mo after the resection. In addition, surveillance endoscopy needed to be performed within 1 to 3 mo in cases resected into more than 5 pieces, and within 4 to 6 mo in cases resected into less than 4 pieces. Based on these, we strongly suggest that not only the piecemeal resection procedure but also the number of the resected pieces increase the risk of colorectal tumor recurrence (Table 4). In Table 5, we provide our recommendation for the interval preceding repeat colonoscopy.
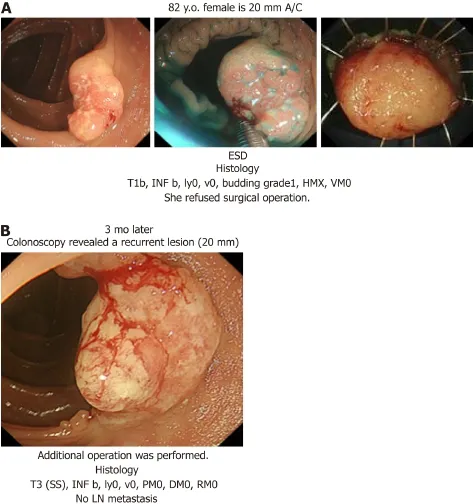
Figure 3 An 82-year-old woman underwent Endoscopic submucosal dissection for a sessile polyp that measured 20 mm in diameter and was located in the ascending colon. A: The tumor histology was T1b cancer with an indistinct margin; however, the patient refused surgical operation because of her old age; B: After 3 mo,colonoscopy revealed a recurrent lesion and surgery was performed. ESD: Endoscopic submucosal dissection.
There are some limitations to this study. Firstly, it was retrospective and was conducted at a single university hospital. Secondly, each endoscopist determined the schedule of the endoscopic surveillance as no Japanese guideline was available. Some of the patients who underwent complete endoscopic resection did not receive careful endoscopic surveillance.
In conclusions, local recurrence of endoscopically treated colorectal tumors depends on the outcome of the first endoscopic procedure. Piecemeal resection was the only significant risk factor associated with local recurrence after endoscopic resection. The interval between endoscopic resection for colorectal tumors and surveillance colonoscopy need to be determined based on the number of pieces.
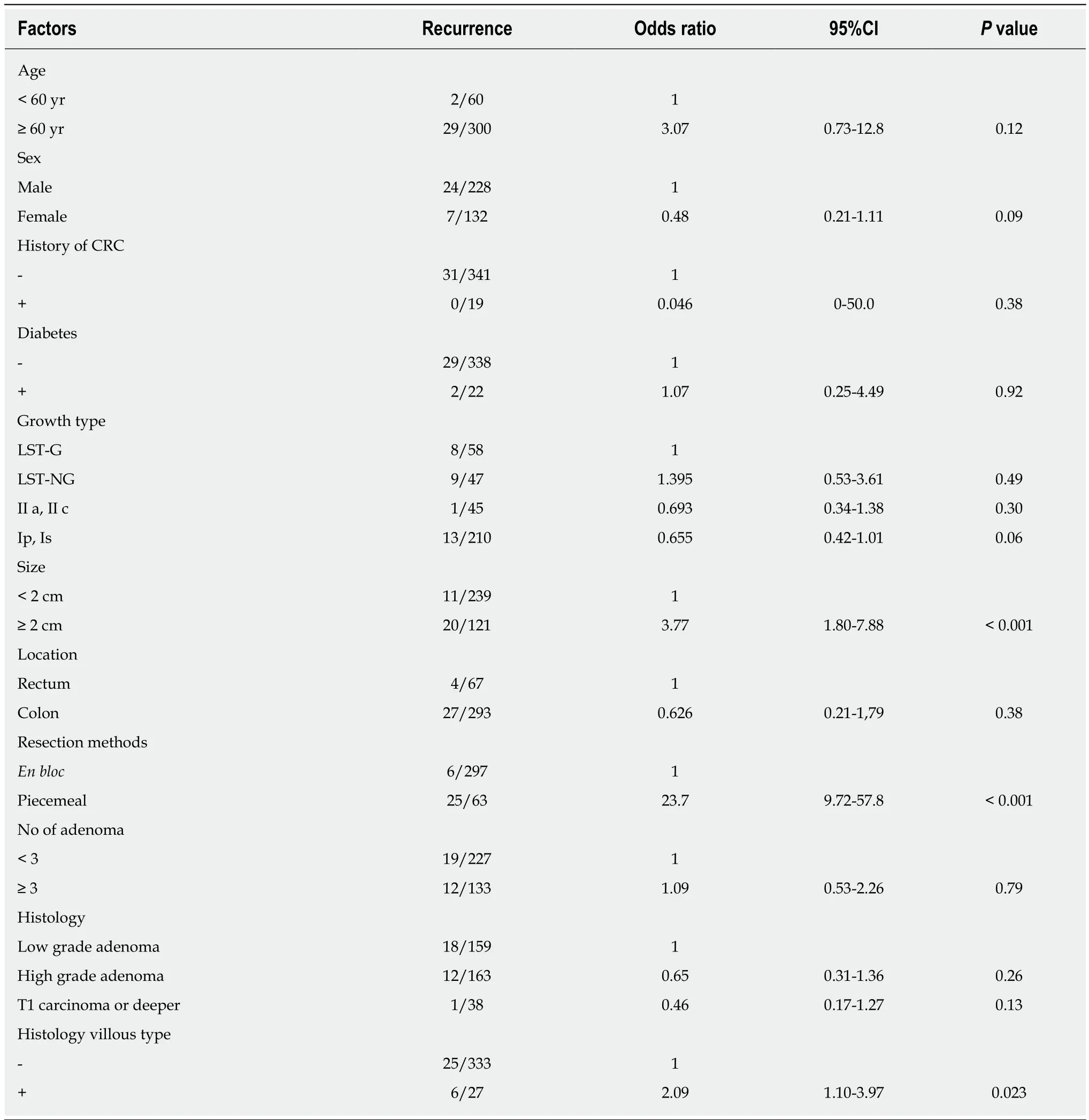
Table 1 Univariate analysis of risk factors for local recurrence

Table 2 Multivariate analysis of risk factors for local recurrence

Table 3 Recurrence rate for the different types of techniques

Table 4 Number of pieces and time to recurrence

Table 5 Recommendation of interval before repeat colonoscopy
ARTICLE HIGHLIGHTS proportion of patients treatedviapolypectomy, endoscopic mucosal resection (EMR), or endoscopic submucosal dissection (ESD). According to a previous meta-analysis, a high incidence of local recurrence of up to 50% after EMR has been reported. Although tumor size,intraprocedural bleeding, piecemeal resection, and high-grade dysplasia have been shown to be associated with local recurrence of colorectal adenoma after EMR, the related risk factors after polypectomy, EMR, and ESD have not been identified. Additionally, the appropriate interval of endoscopic surveillance for colorectal tumors with a high risk of local recurrence has not been established, although the American Cancer Society recommends an interval of 3 to 6 mo for follow-up endoscopic examinations after piecemeal resection for large or sessile polyps.
Research motivation
We need to be cautious in the comparison of our data with those obtained in Western countries due to the difference in endoscopic resection methods.
Research objectives
We attempted to clarify the clinicopathological characteristics of recurrent lesions after endoscopic colorectal tumor resection and determine the appropriate interval.
Research methods
Three hundred and sixty patients (1412 colorectal tumors) who underwent polypectomy, EMR,or ESD and received endoscopic surveillance subsequently for more than one year to detect local recurrence were enrolled in this study. Although most previous reports successfully identified lesional factors associated with the local recurrence of colonic tumors after endoscopic treatments, such as tumor sizes, endoscopic findings, and tumor locations, few reports have tried to identify patient factors, such as age, sex, history of colonic tumors, and diabetes. In this study,we performed univariate and multivariate analysis to identify patient factors associated with local recurrence.
Research results
Local recurrence was observed in 31 of 360 (8.6%) patients [31 of 1412 (2.2%) lesions] after colorectal tumor resection. Piecemeal resection, tumor size of more than 2 cm, and the presence of villous components were associated with colorectal tumor recurrence after endoscopic resection. Of these three factors, the piecemeal resection procedure was identified as an independent risk factor for recurrence. Colorectal tumors resected into more than five pieces were associated with a high risk of recurrence since the average period from resection to recurrence in these cases was approximately 3 mo. The period to recurrence in cases resected into more than 5 pieces was much shorter than that in those resected into less than 4 pieces (3.8 ±1.9 movs7.9 ± 5.0 mo,P<0.05).
Research conclusions
Local recurrence of endoscopically treated colorectal tumors depends upon the outcome of first endoscopic procedure. Piecemeal resection was the only significant risk factor associated with local recurrence after endoscopic resection. The interval between endoscopic resection for colorectal tumors and surveillance colonoscopy need to be determined based on the number of pieces.
Research perspectives
The interval between endoscopic resection for colorectal tumors and surveillance colonoscopy need to be determined based on the number of pieces in prospective study.
杂志排行

World Journal of Gastroenterology的其它文章
- International consensus statement on robotic hepatectomy surgery in 2018
- Growing burden of alcoholic liver disease in China: A review
- ?Esophageal diverticulum: New perspectives in the era of minimally invasive endoscopic treatment
- Gut microbiota profile in healthy Indonesians
- Ursodeoxycholic acid ameliorates hepatic lipid metabolism in LO2 cells by regulating the AKT/mTOR/SREBP-1 signaling pathway
- Accuracy of multi-echo Dixon sequence in quantification of hepatic steatosis in Chinese children and adolescents