Ulcerative colitis complicated with colonic necrosis, septic shock and venous thromboembolism:A case report
2019-03-14MingYuZhuLiQunSun
Ming-Yu Zhu, Li-Qun Sun
Abstract
Key words: Ulcerative colitis; Total colonic necrosis; Venous thromboembolism; Sepsis;Septic shock; Case report
INTRODUCTION
Ulcerative colitis (UC) is a chronic inflammatory disease, is easy to relapse, and prognosis is poor once there are complications[1].Patients with UC have mucosal inflammation, which may extend continuously to the entire colon[2].Total colonic necrosis, a complication in UC, is rarely reported and can be life threating.We present a patient with UC who developed total colonic necrosis, septic shock and venous thromboembolism (VTE) accompanied by acute kidney injury (AKI).The patient was successfully treated with emergency surgery and support therapies.This case suggests that occurrence of colonic necrosis in UC should be noticed, and timely colectomy should be performed to prevent critical complications.
CASE PRESENTATION
Chief complaints
A 36-year-old female was admitted to our hospital with abdominal pain, diarrhea,mucus blood, pus and recurrent tenesmus attacks.
History of present illness
Her condition was improved with fecal microbiota transplantation.Nine days later,she complained of anuria, vomiting and diarrhea, which were more severe than before.
History of past illness
The patient was diagnosed with UC ten years previously.She was maintained on mesalazine and prednisone but without comprehensive treatment.
Physical examination
About 100 mL dark colored urine was drained, and bloody fluid was discharged from the urethral catheter.She appeared dyspneic with cold clammy limbs, increased pulse rate, abdominal cavity pressure of 25 mmHg and grade IV abdominal hypertension[3].
本文仅讨论旋翼UAV,且面向IoT设备数据的稳定采集,而非突发状况监测,因此假设飞行姿态恒定,加速度此时,UAV与移动IoT设备分簇的联合运动能耗主要由K个UAV的航路点变化与航路点间的速度决定.设t时刻第j个UAV由最优布署坐标运动到t+1时刻第l个UAV的最优布署坐标位移为则联合运动能耗为[20],
Laboratory and imaging examinations
The endoscopy demonstrated total colonic wall thickening, erosions in luminal surface of colon, hyperemia, friability, bleeding and ulcerations (Figure 1).Laboratory tests revealed white blood count of 40.77 × 109/L, red blood count of 2.41 × 1012/L,hemoglobin of 60 G/L and sequential organ failure assessment scores of 10 (Table 1).Emergent computed tomography showed suspicious thin perforations at rectosigmoid colon and massive ascites (Figure 2).
FINAL DIAGNOSIS
Septic shock, colonic perforation, UC, acute renal failure, disseminated intravascular coagulation and severe anemia.
TREATMENT
She underwent urgent total proctocolectomy and ileostomy.During surgery, massive ascites, total colonic necrosis, edema and dilatation of small intestine were observed(Figure 3) but with no obvious perforation and arterial thrombosis.The ascites culture was negative.Histopathological examination of the resected colon showed mucosal inflammation, necrosis and hemorrhage (Figure 4).After etiological treatment, the patient was transferred to the intensive care unit.Her symptoms were alleviated, and urine excretion was normal with maintenance of renal perfusion.Ascites fluid of 1880-3880 mL was drained daily for 7 d in the intensive care unit.The possibility ofthrombosis was considered.Following anticoagulant therapy, the volume of ascites was reduced gradually.The condition of the patient gradually improved after active treatment.Computed tomography angiography displayed thrombosis in the trunk of portal vein and its intrahepatic branches, the superior mesenteric vein and the splenic vein (Figure 5).The patient recovered and was discharged from the hospital after antibacterial, anticoagulant and nutritional support treatment.
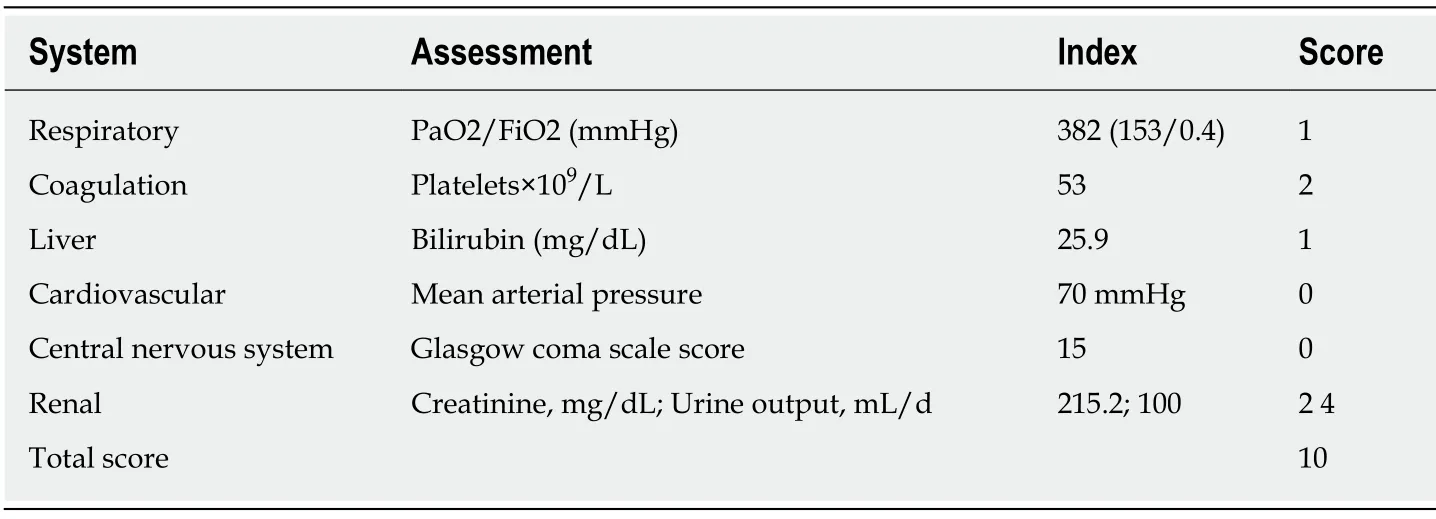
Table 1 Sepsis-related organ failure assessment score
DISCUSSION
UC affects the colon and most commonly afflicting young adults aged 30-40 years[4].UC complicated with total colonic necrosis has not been reported, and the mortality rate of septic shock secondary to colon necrosis is extremely high.Such severe UC is potentially a life-threatening condition that requires attention and early recognition[5].The present patient had a long course of UC involving the whole colon.Fecal microbiota transplantation through the jejunum tube does not damage the colon.Related factors for colon necrosis in this patient included non-occlusive mesenteric ischemia, shock and long-term inflammation.Immediate surgical intervention for refractory UC could improve outcomes[6].Restorative proctocolectomy with ileal pouch-anal anastomosis is the most commonly performed surgery for UC.
Sepsis is defined as life-threatening organ dysfunction caused by an overwhelming immune response to infection[7].Septic shock is associated with a greater risk of mortality than sepsis alone[8].Sepsis with a sequential organ failure assessment score of ≥ 2 in a patient with suspected infection indicates a risk of death[9].The sequential organ failure assessment score of our patient was 10 and was highly associated with serious infection.Total colonic necrosis is the etiology of sepsis.Tissue hypoperfusion accompanied by septic shock, if persistent may lead to organ dysfunction and failure[10].The cases of AKI account for more than 50% in sepsis[11].Septic AKI is diagnosed with an increase in serum creatinine or a decrease in urinary output[12].The patient developed anuria after abdominal pain, which is a sign of renal dysfunction.The compression of the renal artery by abdominal hypertension is also one of the causes of AKI.In this case, the renal function recovered, making computed tomography angiography imaging possible.Source control measures are important in the treatment of abdominal sepsis[13].Removal of total colonic necrosis helps alleviate septic shock and lower the abdominal pressure.Volume resuscitation, vasopressor and antimicrobial therapy are the main treatments for septic shock[14].Manifestations of sepsis depends on the infection, the organ dysfunction, the underlying health condition of the patient and the aggressive treatment used[15].Septic shock in this patient was caused by abdominal infection and characterized by coagulation disorders and AKI rather than circulatory and respiratory dysfunctions.
The risk of VTE in patients with UC is 3-4 times higher than that in the normal population with an overall incidence up to 7%[16], especially in those with a long-term use of prednisone.VTE is associated with disease activity in UC[17].Portal vein thrombosis and mesenteric venous thrombosis in our patient were severe complications associated with UC and surgery.The prevalence of portal vein thrombosis in the general population is about 1%[18].A large amount of ascites before,during and after surgery was considered to be associated with portal vein thrombosis,but angiography could not be performed in these patients because of AKI.Patients with mesenteric venous thrombosis can present with acute abdominal pain, but most of them have vague clinical presentation, which makes it difficult to be diagnosed in time[19].VTE is often a critical condition and anti-coagulate therapy should be given as soon as the diagnosis is made[20].It is important to prevent VTE during hospitalization.

Figure 1 Endoscopy demonstrated total colonic wall thickening, erosions in luminal surface of colon,hyperemia, friability, bleeding and ulcerations.
CONCLUSION
Early computed tomography angiography is necessary in patients with severe UC.Total colonic necrosis is a rare complication in UC.If medical therapy fails, close observation of surgical indications and timely colectomy should be performed to prevent critical complications.

Figure 2 Thin flaws and perforations at rectosigmoid colon and a large amount of fluid in abdominal cavity and pelvis were found by emergency computed tomography.

Figure 3 Total colonic necrosis was seen during operation.
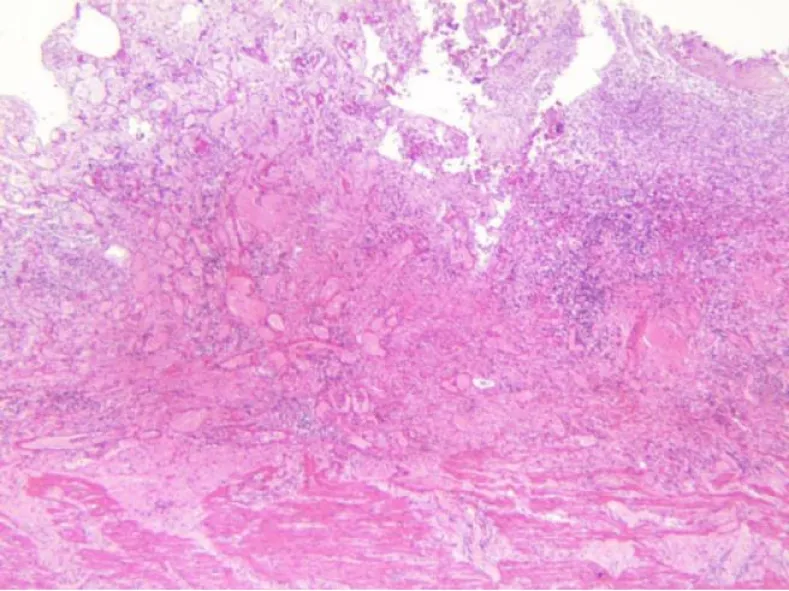
Figure 4 Histopathological examination of the resected colon in the patient showed extensive hemorrhage, necrosis and exudation involving the whole intestinal wall and the extraserous adipose tissue.

Figure 5 Plain computed tomography scanning and contrast enhancement of abdomen display thrombosis in the trunk of portal vein and its intrahepatic branches, the superior mesenteric vein and the splenic vein.
猜你喜欢
杂志排行
World Journal of Clinical Cases的其它文章
- Malignant syphilis accompanied with neurosyphilis in a malnourished patient:A case report
- Ex vivo revascularization of renal artery aneurysms in a patient with solitary kidney:A case report
- Pseudothrombus deposition accompanied with minimal change nephrotic syndrome and chronic kidney disease in a patient with Waldenström's macroglobulinemia:A case report
- Hepatocellular carcinoma successfully treated with ALPPS and apatinib:A case report
- Treatment of invasive fungal disease:A case report
- Acute pancreatitis connected with hypercalcemia crisis in hyperparathyroidism:A case report