Comprehensive lifestyle intervention vs soy protein-based meal regimen in non-alcoholic steatohepatitis
2019-03-11PeterDeibertAdharaLazaroDeniseSchaffnerAloysBergDanielKoenigWolfgangKreiselManfredBaumstarkDanielSteinmannMartinBuechertThomasLange
Peter Deibert, Adhara Lazaro, Denise Schaffner, Aloys Berg, Daniel Koenig, Wolfgang Kreisel,Manfred W Baumstark, Daniel Steinmann, Martin Buechert, Thomas Lange
Abstract BACKGROUND Non-alcoholic steatohepatitis (NASH) has become one of the leading causes of liver disease in the western world. In obese patients weight reduction is recommended. Up to now there are no specific guidelines for weight loss in order to reduce hepatic fat content.AIM To investigate the effects of a 24-wk guided lifestyle intervention program compared to a meal replacement regimen based on soy protein.METHODS Twenty-six subjects with NASH participated in a randomized single-center study. They were randomly assigned to either meal replacement group (MR-G)with soy-yogurt-honey preparation or to guided lifestyle change group (LC-G)with endurance activity and nutrition counselling. Serum alanine transaminase(ALT), aspartate transaminase (AST), lipid parameters, and adipokines were measured. Liver fat content and lipid composition were determined by magnetic resonance imaging and magnetic resonance spectroscopy. Body fat mass and lean body mass were assessed using Bod Pod® device. Pre- and post-intervention monitoring of parameters was performed. Statistical analyses were conducted with SPSS software, results were expressed as median (interquartile range).RESULTS Twenty-two subjects (MR-G, n = 11 and LC-G, n = 11) completed the study (9 women, 13 men; age 52.1 (15.0) years, body mass index (BMI) 32.3 (3.3) kg/m²).In both groups a significant weight loss was achieved (MR-G: -6.4 (3.6) kg, P <0.01; LC-G: -9.1 (10.4) kg, P < 0.01). BMI dropped in both groups (MR-G: -2.3 (1.5)kg/m2, P = 0.003; LC-G: -3.0 (3.4) kg/m2, P = 0.006). Internal fat and hepatic lipid content were markedly reduced in both groups in comparable amount. There was a strong correlation between reduction in liver fat and decrease in ALT.Likewise, both groups showed an improvement in glycemic control and lipid profile. Changes in adipokines, particularly in adiponectin and leptin were closely related to intrahepatic lipid changes.CONCLUSION Comprehensive lifestyle intervention and meal replacement regimen have comparable effects on body and liver fat, as well as decrease in markers of hepatic inflammation among NASH patients.
Key words: Non-alcoholic steatohepatitis; Meal replacement therapy; Soy protein;Lifestyle change; Weight reduction; Obesity
INTRODUCTION
Non-alcoholic steatohepatitis (NASH) has become one of the leading causes of liver disease in western countries. It is estimated that about 20% to 30% of adults in developed countries have excess fat accumulation in the liver, 50% among people with diabetes, and about 80% in the obese and morbidly obese[1]. The main feature of NASH is the presence of fat in the liver accompanied by signs of inflammation and/or damage. Without the latter, the condition is referred to as non-alcoholic fatty liver disease (NAFLD)[2].
NASH may lead to liver cirrhosis and portal hypertension with severe sequelae including hepatocellular carcinoma. It is the most rapidly growing indication for liver transplantation in patients with hepatocellular carcinoma in the United States[3]Though there are no established guidelines for the prevention or treatment of NASH an increase of physical activity or weight loss are recommended.
Physical activity has been known to improve insulin resistance, maintain weight loss, and improve liver histology in NASH patients. An increase in physical performance has been associated with improved hepatic metabolism, even independent of body weight reduction[4-7]. Physical activity increases hepatic fatty acid oxidation and decreases the intermediates of fatty acid synthesis, resulting in a decrease of hepatic steatosis[8]. Habitual leisure-time physical activity or aerobic exercise training may play a protective role in NAFLD[7,9,10]. However, there is no evidence on the specific kinds of exercise (e.g. in terms of duration, intensity) which will be of most benefit[11].
Weight loss due to caloric restriction has been proven to reduce hepatic fat content.With a gradual weight reduction under a balanced diet, Uenoet al[12]demonstrated significant reduction in hepatic steatosis and an improvement in hepatic inflammation and fibrosis. Hepatic lipid content is also influenced by other factors such as lipid composition of the diet and the condition of the anti-oxidant system[13,14]. However, the optimal dietary restrictions are still under debate, thus a clear recommendation for the patients is still lacking[15]. As insulin resistance is a key mechanism in both metabolic syndrome and NASH, observational studies consistently reported an association between higher liver fat content and high risk of coronary artery disease. There is an increased risk for cardiovascular disease in patients with NASH[16].
On the other hand, liver fat content seems to be a risk factor that is not strictly related to insulin resistance[6,17]and may be of further significance. With MRS liver fat content is quantifiable. This method is regarded as gold standard to detect the accumulation of liver fatin vivo[18]. Moreover, the chain length of stored fatty acids and the percentage of saturated lipids can be estimated noninvasively. In a previous randomized controlled study, it was shown that with respect to weight reduction the effect of therapeutic lifestyle changes is comparable to a meal replacement regimen based on soy protein[19]. Furthermore, parameters defining the metabolic syndrome can be improved with either intervention[20,21].
Fat storing cells are no longer considered as energy stores only, as they also influence the metabolism by secretion of polypeptide hormones known as adipokines.Adiponectin has anti-inflammatory, anti-diabetic, and anti-atherogenic properties[22].Its expression and plasma concentration are inversely related to insulin resistance,metabolic syndrome and type 2 diabetes mellitus, as well as obesity. Leptin is secreted proportionally to the amount of white adipose mass. Its levels in the circulation depend on the amount of adipose tissue and the status of energy balance[23]. High levels of leptin in the circulation are associated with the severity of NAFLD[24]. On the other hand, fetuin A has been suggested as noninvasive biomarker of hepatic steatosis and as an early indicator of NAFLD[25,26]. Vaspin was seen to be associated with NAFLD and grade of hepatic inflammation[27,28]. However, other studies yielded conflicting results, thus the role of Vaspin in NAFLD remains unclear. Lastly, resistin has been positively associated with histological steatosis and portal inflammation[29].
This study aims to compare a guided intensive lifestyle intervention program and a soy protein-based meal replacement therapy in patients with NASH. The effects of a significant weight loss after 24 wk on liver fat content, lipid composition, and markers of liver inflammation were analyzed. Changes in abdominal, subcutaneous and intrahepatic fat, as well as body composition in both interventions were also studied.In a subgroup, the proportion of saturated and unsaturated lipids of intrahepatic fat was quantified and analyzed in relation to serum adipokines.
MATERIALS AND METHODS
Patients eligible for participation were obese adults with body mass index (BMI)between 30 and 40 and with sonographic findings of fatty liver, as well as elevated liver enzymes [at least alanine transaminase (ALT) of > 20% the ULN]. Daily alcohol consumption had to be less than 20 g in males and less than 10g in females. Secondary causes of fatty liver disease other than overweight and obesity were excluded by anamnesis. The possibility and willingness to participate in a physical training program was another prerequisite.
Exclusion criteria included limited physical performance (ergometer test: < 75 Watt for 2 min), insufficiently treated arterial hypertension, insulin-dependent diabetes mellitus, renal disease with compromised renal function, psychiatric disorder, and intake of hormones. All subjects completed a comprehensive medical examination,routine blood tests, and ultrasound at the screening visit. Exercise tests were done using a cycling ergometer (Ergoline, Siemens, Germany) starting with a workload of 25 W, increasing by 25 W every 2 min until exhaustion. Written informed consent was provided by all subjects and the study protocol was approved by the Ethics Review Board of the University of Freiburg Medical Center.
The subjects were randomly assigned to the treatment groups using a random list.During the first six weeks of the program, the subjects in the meal replacement group(MR-G) were instructed to replace two daily meals with a commercially available soyyogurt-honey preparation (Almased®) as recently described in a study by Koohkanet al[30]. In the following 18 wk, one daily meal was replaced by the preparation. In addition, the dietary intake of fat during this second phase was not to exceed 60g per day. The first 6-wk diet contained 1000 kcal per day for women and 1200 kcal for men,while in the following weeks the dietary program was aimed at a maximum of 1500 kcal for women and 1700 kcal for men. These guidelines were given at a group session after randomization by a dietician.
On the other hand, the lifestyle change group (LC-G) attended 6 weekly teaching sessions about nutrition and physical exercise. They had individual consultations preintervention and then again at week 6. All sessions were conducted by experts in nutritional counselling. Subjects received a diet overview handout in accordance with the guidelines set by the German Society of Nutrition and the German Society of Sports Medicine and Prevention. Here, the prescribed dietary program was a moderate fat, nutrient-balanced diet consisting of 1200 to 1500 kcal per day for women and 1500 to 1800 kcal per day for men. It contained approximately 50%-55%of the calories from carbohydrates, 25%-30% from fat, and 15%-20% from protein. The diet program was similar to the previous study by Königet al[31].
Physical exercise was performed as a group session once a week during the first six weeks and twice a week thereafter. The group-based exercise sessions were led by a sport physiologist. Each participant was instructed to walk mainly at a specific heart rate reflecting 60%-75% of the individual estimated VO2max.
Magnetic resonance imaging (MRI) and magnetic resonance spectroscopy (MRS)measurements were performed with a 3T whole-body MRI system (Magnetom Trio a TIM system, Siemens Healthcare, Erlangen, Germany) using two six-channel body array coils for signal reception. Radiologists were blinded for treatment allocation. For abdominal fat-water imaging a previously optimised breath-hold spoiled 2D gradient echo protocol with four different echo times and a monopolar readout gradient was used[32]. Liver fat content and composition were measured by MRS using a single voxel PRESS (Point RESolved Spectroscopy) sequence with an echo time of TE = 35 ms. A cubic volume of interest (8 mL) was placed in the lateral part of the liver avoiding inclusion of larger blood vessels and subcutaneous fat. The MRS measurement was triggered with a 2D PACE (Prospective Acquisition Correction)navigator to minimize respiratory motion effects[33]. It was performed once with water suppression for a more robust lipid peak resolution and once without water suppression for acquisition of a water reference signal.
Reconstruction of fat and water images was performed using the graph cuts algorithm[34]. Segmentation of subcutaneous and internal adipose tissue (AT),including visceral AT, muscular fat, and bone marrow was conducted in the abdominal region with an active contour algorithm[35]. The classification of adipose tissue topography proposed by Shenet al. was adopted[36]. Fat quantification was performed as previously described by Ludwiget al[37].
The liver spectra were fitted and quantified with LCModel[32]using a dedicated analysis protocol for lipid detection in the liver. The lipid signal was modelled with peaks at [0.9, 1.3, 1.6, 2.1, 2.3, 2.8, 4.1, 4.3, 5.2, 5.3] ppm by LCModel.
Lipid peak quantification was considered reliable if the quantification error estimated by LCModel was smaller than 10%. Subjects were only included in the analysis of MRS-based parameters if all lipid resonances could be quantified with an estimated error margin of less than 10%.
The total fat signal (FS) was quantified as the sum of the integrated lipid peaks at 0.9 ppm, 1.3 ppm and 1.6 ppm, the water signal (WS) as the integrated water peak in the non-water-suppressed spectra. The integrated signals were corrected with the relaxation constants reported by Hamiltonet al[38]using T2W= 23 ms for water and T2F= 62 ms for the lipid signal. Consequently, the intrahepatic lipid (IHL) content was calculated as: IHL = [FS*exp (TE/T2F)]/[FS*exp (TE/T2F) + WS*exp (TE/T2W)].
Lipid chain length, saturated lipid component, total unsaturated lipid component,and fraction of unsaturated lipids were determined as described by Yeet al[39,40].
For measuring body composition the technique of air displacement plethysmography (Bod Pod®device, Cosmed, Germany) was used[41,42]. Waist circumference was taken with a non-distensible tape measure following the anthropometric standardization guidelines[43].
The data collected upon enrolment and after 6 and 24 wk included the anthropometrics (i.e. body weight, waist and abdominal circumference), together with self-reported medical history, blood pressure, glucose, and serum lipids. Adipokines(i.e. leptin, adiponectin, resistin, vaspin, and fetuin A) were measured by commercially available ELISA tests (DSL Deutschland GmbH, Sinsheim, Germany).All other laboratory analyses were done in the central laboratory of the University of Freiburg Medical Center using clinical routine methods.
Statistical analysis
The primary study endpoint was the change in IHL content. Assuming an average IHL content of 23±7% based on the computations by Sullivanet al[44], detecting a change of 10% with a power of 0.95 and an error of 0.05 at least eight participants were necessary. Evaluations of efficacy variables were analyzed in an exploratory manner. Descriptive statistical methods were used to analyze the variables. Results were expressed as median (interquartilrange IQR). To test the absolute and relative change of the parameters, a signed-rank test was used. All P values were two-sided and a P value of 0.05 or less was considered statistically significant. Bivariate associations between variables of interest were assessed by Spearman’s rank correlations (ρ). To evaluate potentially predictive variables of IHL content a multivariate regression with backward elimination of variables was performed. All statistical analyses were calculated using SPSS software (version 25.0.0).
RESULTS
Patient population
One hundred seventy-eight patient records with a diagnosis of NASH were reviewed from the outpatient database of the Department of Sports Medicine and Department of Gastroenterology and Hepatology (Figure 1). Seventy-six eligible subjects were contacted and interviewed concerning the study’s exclusion criteria, in which 43 patients were invited for screening. Fifteen patients responded to the study announcement via Intranet and five of them were invited for initial screening.Overall, 48 prospective subjects were invited for screening and this led to 26 eligible participants who were randomized to the study groups. A total of 22 patients (LC-G =11, MR-G = 11) completed the study and attended at least 75% of the meetings/training sessions and consultation visits. All of these patients were evaluated at baseline (pre-intervention) and final visit (post-intervention). Four participants dropped out because of not having attended the necessary number of sessions. Baseline data showed that both groups were comparable in all parameters of interest (Table 1).
Anthropometric parameters
Within 6 wk both groups showed a significant reduction in body weight (MR-G: 101.1(30.5) to 94.8 (23.7) kg;P< 0.01; LC-G: 99.5 (11.1) kg to 83.3 (26.4) kg,P< 0.01). As shown in Table 2, after 24 wk the MR-G had reduced mean body weight of 6.4 (3.6) kg and the LC-G 9.1 (10.4) kg (P= ns between the groups). BMI was reduced from 32.2(3.4) to 29.6 (3.3) in the MR-G and from 32.4 (3.7) to 29.3 (4.5) in the LC-G. In the MR-G waist circumference was more reduced in comparison to the LC-G. Changes were comparable between both groups, resulting in statistically significant lower values at the final visit (P< 0.001). The BodPod analysis at baseline and final visit showed a stable lean body mass in both groups, whereas body fat mass was reduced significantly in both interventions (Figure 2A).
Biochemical laboratory parameters
ALT and AST values decreased in both treatment regimens, the change being more pronounced in the LC-G (Table 2). Both changes were significant within each group (P< 0.05) and no significant difference was found between the two groups. The relative change in ALT was correlated with the relative change in abdominal fat (ρ = 0.70;P<0.01), subcutaneous fat (ρ = 0.72,P< 0.01), internal fat (ρ = 0.65;P< 0.01), and change in AST (ρ = 0.96;P< 0.01). There was a weaker correlation to relative change in body fat mass (ρ = 0.52;P< 0.05) and to relative change in waist circumference (ρ = 0.48;P< 0.05).
Cholesterol did not significantly decrease in both groups, whereas there was a significant decrease in triglycerides only in the MR-G. HDL-cholesterol showed a slight but non-significant increase in both groups, while LDL-cholesterol was nearly unchanged (bothP= n.s.). Fasting glucose and HbA1c-values were reduced in both groups, this reduction was more pronounced in the LC-G. However, the decrease did not differ significantly between groups. Serum creatinine values were initially comparable and were unchanged in both groups.
In terms of adipokines, adiponectin showed a slight increase in both groups,whereas leptin showed a significant decrease over the 24-wk study period in both groups. Vaspin, resistin, and fetuin A did not show significant changes over the period of 24 wk (Figure 2B).
MRI and MRS measurements of abdominal fat and liver fat
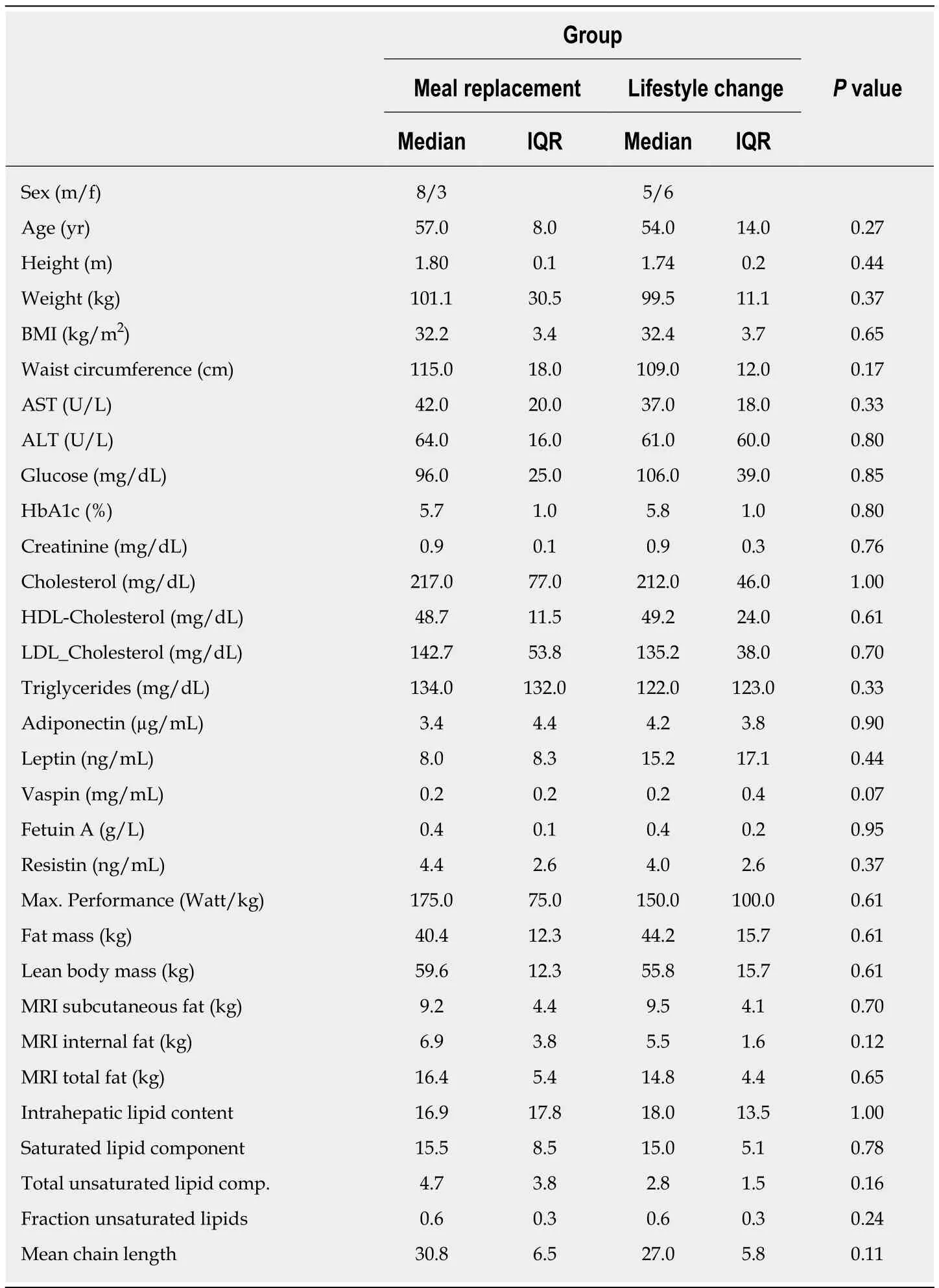
Table 1 Baseline characteristics
Both interventions reduced the total abdominal fat as estimated by MRI. However, it was significantly reduced only with lifestyle intervention (MR-G: 16.4 (5.4) kg to 15.0(5.4) kg;P= n.s., LC-G: 14.8 (4.4) kg to 13.4 (2.3) kg;P< 0.05; difference between groupsP= 0.06, Figure 2A). There was significant reduction of subcutaneous fat in both groups, being more pronounced in the lifestyle intervention group (P= 0.06 between groups). Furthermore, the LC-G lost more internal fat than the MR-G,however this difference was not statistically significant between the groups. The ratio of relative internal fat loss to subcutaneous fat loss was comparable in both groups(MR-G: 0.42, LC-G: 0.36;P= n.s.).
Adiponectin and leptin showed weak correlations to total abdominal fat mass as estimated by MRI (adiponectin: ρ = 0.24; leptin: ρ = 0.60) or Bodpod device(adiponectin: ρ = 0.58; Leptin: ρ = 0.88), waist circumference (adiponectin: ρ = -0.01;leptin: ρ = 0.06) or BMI (adiponectin: ρ = -0.09; leptin: ρ = 0.33). Furthermore, fetuin A,vaspin, and resistin showed no relevant correlations to such parameters (ρ < 0.2 for all). However, adiponectin changes were inversely related to changes in body weight(ρ = -0.25), fat mass (ρ = -0.30), reduction in waist circumference (ρ = -0.13) and total abdominal fat (ρ = -0.13). Leptin changes were correlated to changes in body weight(ρ = 0.65), fat mass (ρ = 0.63), waist circumference (ρ = 0.39) and total abdominal fat (ρ= 0.49).
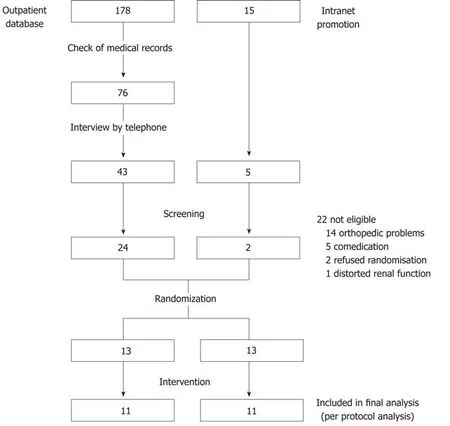
Figure 1 Flowchart of the study selection procedure.
The baseline saturated lipid component was correlated with waist circumference (ρ= 0.4;P= n.s.), as well as with subcutaneous fat (ρ = 0.44;P< 0.01), total abdominal fat(ρ = 0.54;P< 0.01) and body fat mass as estimated by the BodPod device (ρ = 0.57;P<0.01). It was not correlated with internal fat (ρ = 0.07;P= n.s.). By multivariate regression analysis IHL content was negatively correlated to total unsaturated lipid component and positively correlated to mean chain length. The fraction of unsaturated lipids and the total unsaturated lipid compound did not significantly predict IHL and were eliminated from the model. In a second model IHL content could not be predicted by total abdominal fat measured by MRI, waist to hip ratio, fat mass measured by BodPod, waist circumference or weight.
In both intervention groups there was a highly significant reduction of liver fat content (MR-G: -56.2 (30.5)%;P< 0.01; LC-G: -77.2 (57.8)%;P< 0.05 Figure 3), being correlated to weight change (ρ = 0.77 in MR-G and ρ = 0.88 in LS-G).
The IHL composition was not differentiable in all cases since in some spectra insufficient spectral quality did not allow for accurate quantification of all underlying resonances. Therefore, in a subgroup intrahepatic lipids were analyzed and characterized with regard to IHL component, saturated lipid component, and fraction of unsaturated lipids. Furthermore, the mean chain length of intrahepatic lipids was estimated. Changes of the saturated lipid component could be calculated in 15 participants and changes of the unsaturated lipid component in 16 participants,respectively.
The IHL content and the saturated lipid component decreased during the intervention in both groups (MR-G: IHL content: 16.9 (17.8) to 6.7 (10.2),P< 0.01; LCG: 18.0 (13.5) to 5.5 (10.2);P< 0.05; MR-G: saturated lipid component: 15.5 (8.5) to 14.3(2.6),P= n.s.; LC-G: 15.0 (5.2) to 13.0 (5.5),P< 0.05, Figure 3). The fraction of unsaturated lipids showed a decrease only in the meal replacement group (MR-G: 0.6(0.3) to 0.48 (0.38),P= n.s.; LS-G: 0.6 (0.3) to 0.6 (0.3),P= n.s.). Mean chain length was significantly reduced only in the meal-replacement group [MR-G: 30.8 (6.5) to 25.5(7.3),P< 0.05; LC-G: 27.0 (5.8) to 31.4 (13.3),P= n.s.] (Figure 3).
The relative change in IHL content was correlated to relative weight change in both groups (MR-G: ρ = 0.77, LC-G: ρ = 0.88), as well as to relative changes in internal fat(MR-G: ρ = 0.67, LC-G: ρ = 0.81), fat mass (MR-G: ρ = 0.77, LC-G: ρ = 0.71), and waist circumference (MR-G: ρ = 0.46, LC-G: ρ = 0.83). The relative change in IHL content as a function of relative weight loss was slightly more pronounced in the MR-G (Figure 4).
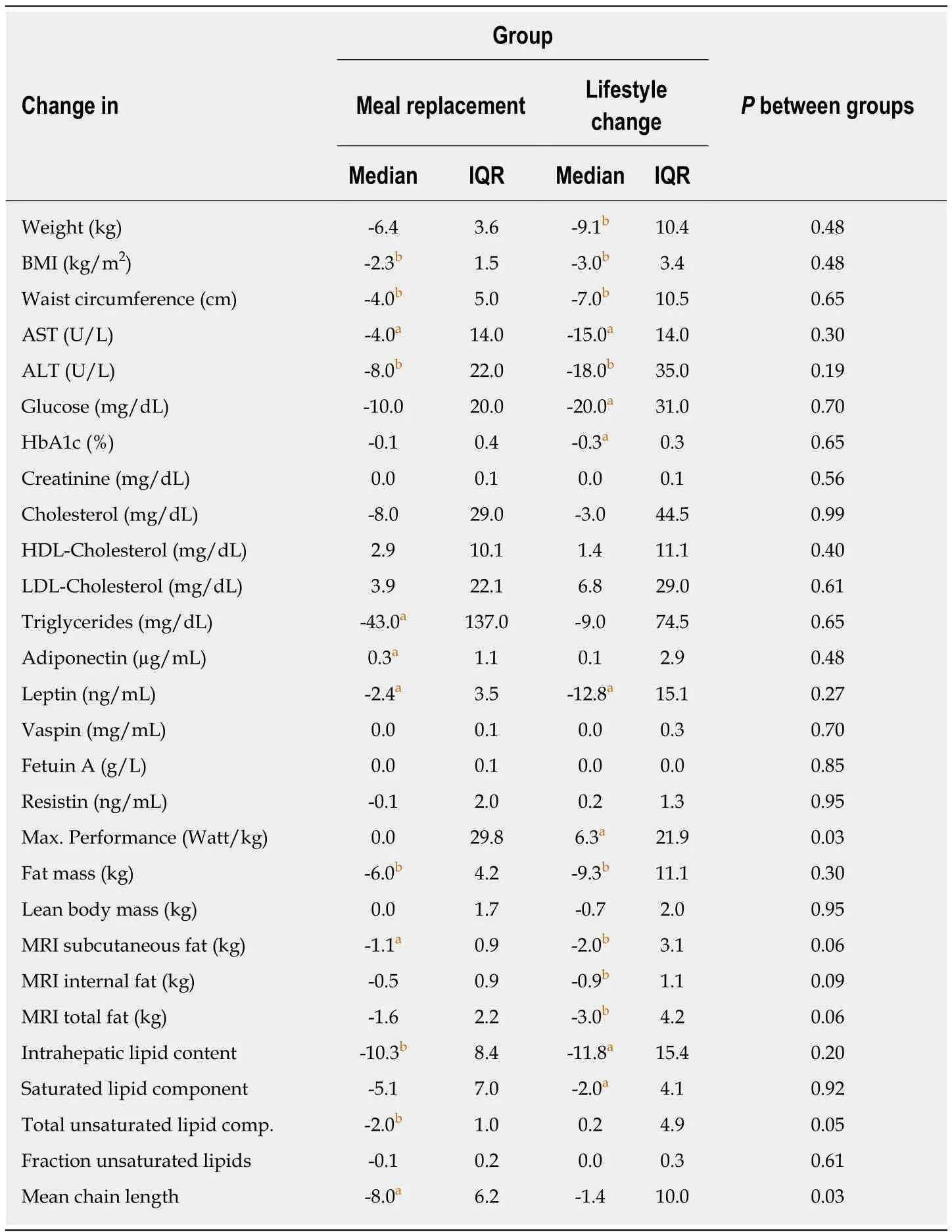
Table 2 Comparison of changes in parameters
The changes in the IHL were studied in relation to changes in adipokines. The latter correlate to the change in IHL content, being more apparent in the LC-G. Adiponectin rose as IHL content decreased, while leptin declined with a reduction of IHL content.Resistin, vaspin and fetuin A showed only weak correlations to adipokines.
Physical performance
Maximum performance in ergometer testing was improved only in the LC-G, with an increase of maximum cycling power. In terms of the measured muscle mass (fat free mass, ffm) by Bodpod®, only the LC-G showed a significant increase in performance(MR-G: 2.9 (0.6) W/kg ffm to 2.7 (0.4) W/kg ffM,P= n.s.; LC-G: 2.8 (0.9) W/kg ffm to 3.2 (0.8) W/kg ffm;P< 0.05).
DISCUSSION
This study aimed to compare a meal replacement regimen with lifestyle change as intervention for patients with NASH. The results showed that based on the parameters of interest (i.e., IHL content, body composition, metabolic/biochemical parameters, and anthropometrics) both interventions yielded comparable results specifically in terms of reducing body fat mass, IHL content, and hepatic inflammation.
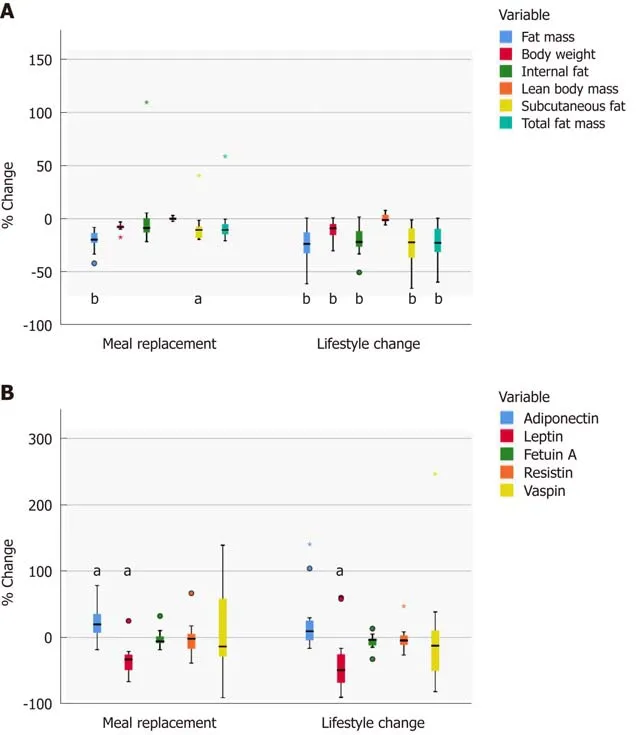
Figure 2 Relative changes in fat components (A) and adipokines (B). A: Relative changes (boxplots) in body fat mass and lean body mass after the 24-wk intervention estimated by the BodPod device. Relative changes in intraabdominal fat, internal and subcutaneous abdominal fat measured by MRI. Significant differences from baseline are marked with for aP < 0.05 and bP < 0.01. B: Relative changes in adipokines (boxplot). Significant changes from baseline are marked with aP < 0.05.
The reduction of IHL content in this study was more pronounced than in another intervention study using mainly aerobic training programs, with a mobilization of liver fat of 30.2% in the exercise only group and 49.8% in the diet and exercise group[44]. A recent systematic review suggested that an exercise program at 70%VO2maxis ideal for mobilizing fat from liver among NAFLD patients[45]. The exercise program used in this study was in accordance with such recommendation and was well tolerated by all of the participants. Studies comparing different exercise programs additive to a dietary intervention demonstrated that the effect of physical activity was minor compared to that of a reduction of caloric intake or change in macronutrients[46-49]. The lifestyle education program used in this study aimed to motivate participants to perform at least 150 min (but preferably 300 min) of moderate-intensity physical activity per week. Participants had to attend two exercise sessions per week, doing sports at an intensity based on the suggested heart rate reflecting 60%-65% VO2maxwhich had been tested individually.
The nutritional counselling encouraged participants to reduce caloric intake and motivated them to engage in sports. Due to this intensive program the reduction in body weight was more pronounced in the LC-G than among the participants of the MR-G. However, metabolic changes and changes in IHL content were comparable.
Participants of the MR-G received instructions on the meal replacement regimen in a group session at the beginning of the study and were further advised individually after 6 wk. Both treatment strategies led to a loss of fat mass while preserving muscle mass, a desirable goal of weight reduction interventions that had been previously described[19]. The increased mean metabolic turnover in the LC-G was about 5.7 MET/wk, corresponding to a caloric increment of 430 kcal/wk. Increasing physical activity is indispensable in a long-term weight control program[50]. In a period of one year these behavioral changes may result in a 3.4 kg loss in body weight. However, it has been shown that a dietary intervention has long-term effects in liver fat and metabolism despite body weight regain[51].
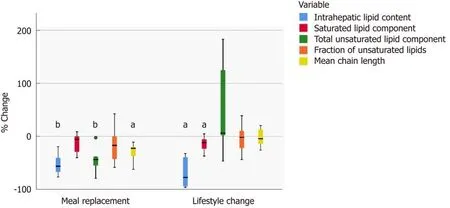
Figure 3 Relative changes in hepatic lipid characteristics. Relative changes in hepatic lipid characteristics (boxplot). Significant changes from baseline are marked with aP < 0.05 or bP < 0.01.
Both groups showed a reduction in cholesterol and triglycerides, as well as an increase in HDL-cholesterol - however, only the decrease in triglycerides in the MR-G was significant. Soy protein with intact isoflavones may decrease total cholesterol,LDL-cholesterol and triacylglycerols and increase HDL-cholesterol[52,53], mimicking the effects of exercise on lipid parameters. The protein content of the nutrition appeared to have a distinct effect on liver fat. An isocaloric protein rich diet, high in animal or plant protein, is able to reduce liver fat by 36%-48%[54]. In terms of body weight change, the MR-G lost more IHL content per loss of body weight than the LC-G.Furthermore, the main weight reduction in the LC-G was initiated through caloric restriction, thus this might have influenced the results. However, physical exercise may lead to a decrease in the intramyocellular lipid content that has been linked to insulin sensitivity[49].
In this study, fasting glucose levels and HbA1c levels decreased similarly in both groups, thus both interventions seemed to be equally effective in improving insulin sensitivity. As NASH is associated with cardiovascular morbidity and mortality[55-58],in addition to an improved glucose tolerance, an improvement in physical fitness and muscular performance is supposed to be beneficial. Expectedly, physical fitness was improved only in the LC-G.
The IHL content was quantified by MRS. With this technique not only the amount of hepatic lipids can be determined with high accuracy[59]but also the mean chain length and percentage of saturated as well as unsaturated lipids may be estimated.However, it should be noted that the calculation of these lipid composition parameters is subject to systematic errors mainly arising from different T2 relaxation of the underlying resonances which cannot be corrected. Therefore, the values calculated in this study should not be regarded as absolute quantities but rather as correlates of the corresponding parameters. With both interventions the IHL content was reduced by more than 50%. The higher reduction in the LC-G was due to a higher extent in body weight reduction in this group. The quality of IHL was more influenced by the meal replacement. In this group the total unsaturated lipid component decreased significantly as did the mean chain length.
A comparable reduction in liver fat was seen in a subgroup of adults with type 2 diabetes examined in the Look AHEAD trial (-50,8% in the lifestyle intervention group)[60]and in patients with NAFLD after gastric banding surgery (-50%)[61]. An exercise intervention in patients with NAFLD led to a weight reduction of -2.5 kg and a change in intrahepatic triglyceride content of 48%[62]. Other interventions have not reduced liver fat content by a similar percentage[7,44,48,55]. An aerobic exercise training that did not lead to a change in BMI led to a decrease in the IHL content of 10.3% ±4.6%[44], while the combination of aerobic exercise and resistance training led to a reduction of IHL content of 16% ± 24%[63]. Four weeks of aerobic cycling exercise program which significantly reduced visceral adipose tissue volume by 12% without changing BMI was able to decrease IHL by 21%[7].
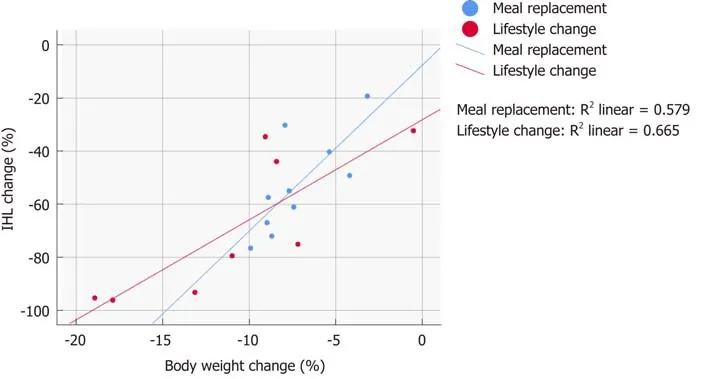
Figure 4 Change in intrahepatic lipid in relation to weight loss. The relationship between change in body weight and change in intrahepatic lipid content. IHL: Intrahepatic lipid component.
The adipokines showed comparable changes in both groups. There was a marked decrease in leptin with both interventions while adiponectin, vaspin, resistin, and fetuin A showed no significant changes over the 24-wk period. Leptin correlates with severity of steatosis and BMI[64], while fetuin A expression is more prominent in NASH[65]. Both showed no significant changes in both interventions. However, the relative changes in leptin and fetuin A were correlated to the changes in saturated lipid component in the LC-G. Likewise, the study demonstrated no significant changes in the levels of resistin, which is linked to abdominal adiposity and elevated triglycerides[29]. Vaspin which is associated to obesity and insulin resistance[28]also showed no significant changes. In contrast, there is a weak correlation to changes in saturated and unsaturated lipid components. It can be concluded that not only the IHL component is of importance, but also the proportion of saturated and unsaturated lipids since these correlate to adipokines. This may explain why some authors report similar levels among NASH patients and controls in contrast to others reporting higher levels among NAFLD patients[66].
The intervention-induced mobilization of intrahepatic fat was different in both groups. With a soy-based meal replacement, saturated and unsaturated lipids were reduced in a comparable amount, whereas lifestyle intervention preferentially led to a loss of saturated liver fat. Furthermore, the mean chain length was markedly reduced only in the MR-G. The changes in the adipokines adiponectin and leptin were correlated to changes in saturated and unsaturated intrahepatic fats, both in the opposite manner. The alterations of liver fat quality were different between both groups, as shown in Figure 3. The results of this study demonstrate that interventions may not only lead to a reduction of liver fat, but also to a change of liver fat quality.Several studies proved a beneficial effect of a dietary approach to an increase in intrahepatic unsaturated fat in NASH. In a model of rats with NASH the administration of omega-3 polyunsaturated fatty acids improved the spectrum of adipokines significantly[67]. In patients with fatty liver disease the hepatic fat content was associated with high energy, high fat, and high saturated fat intake[68]. By a modulation of fat consumption with increased intake of omega-3 polyunsaturated fatty acids in NASH adipokines and markers of hepatic inflammation were changed positively[69]. On the other hand, hepatic n-3 polyunsaturated fatty acid depletion promotes steatosis and insulin resistance in mice and humans[70]. Therefore, a noninvasive analysis of hepatic fat quality may identify a group of NASH patients which could benefit most from supplementation.
In terms of study limitations, the gold standard of assessing hepatic inflammation and fibrosis, as well as lipid content is still histopathological analysis. Presently,1HMRI analysis is a standard method to quantify hepatic steatosis. However, it is not able to assess inflammation or fibrosis. For evaluating fibrosis the non-invasive Fibroscan is conventionally used. In the present study, the focus was on changes in body composition and related IHL changes. Moreover, it was not possible to ascertain whether the caloric restriction in the MR-Group or a specific effect of the soy-yogurthoney preparation led to the different composition of liver fat. However, our study once more confirmed, that with a supplementation of high quality proteins a significant weight reduction without loss of muscle mass is achievable. Finally, the study sample was not large enough to analyze study participant subgroups (i.e., sex and age groups). The small sample size of the study was partly determined by the exclusion criteria, ruling out patients taking hormonal replacement/substitution, antidiabetic drugs or lipid-lowering drugs.
The comparability of both intervention strategies suggests the need for further studies to evaluate the course of hepatic fibrosis in patients with NASH succeeding in a weight reduction program. For physicians managing NASH patients, this study suggests that a soy protein-based meal replacement therapy may be an alternative to a therapeutic lifestyle change, considering the patient’s demands and circumstances.The different changes in hepatic lipid characteristics in each intervention need to be further evaluated.
In conclusion, comprehensive lifestyle intervention and meal replacement regimen had comparable effects in terms of weight reduction, body and liver fat content, and markers of hepatic inflammation among patients with NASH. Lifestyle change may be the ideal approach associated with improved physical fitness and muscular performance, while meal replacement could be an alternative intervention depending on patient’s characteristics, level of motivation, and other life circumstances. The two described approaches changed the amount and quality of IHL content with regard to fatty acid chain length and ratio of saturated/unsaturated lipids. The impact of these findings needs further investigation.
ARTICLE HIGHLIGHTS
Research background
Non-alcoholic steatohepatitis (NASH) is one of the leading causes of chronic liver disease in western countries. The ideal approach to reduce hepatic inflammation and liver fat content is not found yet. Dietary restrictions and physical activity have been shown to be effective, however there is no gold standard established so far.
Research motivation
Many different dietary approaches may be effective in weight reduction. We have shown that by meal replacement therapy with a high-quality soy protein supplementation as well as by comprehensive lifestyle change a weight reduction without loss of muscle mass is achievable.Both interventions can reduce fat mass and liver fat mass. However, blood lipids are changed in different ways with these two interventions. Now we wanted to study whether liver fat quality is differently affected with either intervention.
Research objectives
The main questions of this study were: is there a correlation between loss of liver fat and reduction in body fat, and is one intervention superior to the other in this respect? Is it possible to analyze liver fat quality, and is there a difference in changes in liver fat quality between the two therapeutic interventions?
Research methods
For body composition analysis a Bod pod device was used. Liver fat content was measured by magnetic resonance imaging. For analysis of liver fat quality a magnetic resonance spectroscopy protocol was adapted to quantify the mean chain length and grade of saturation of liver fat. For meal replacement therapy we used a commercially available product based on a soy-yogurthoney preparation. The lifestyle intervention program consisted of guided exercise sessions orientated on individual exercise capacity and dietary counselling.
Research results
Both groups significantly reduced body mass index, fat mass and liver fat content. The lifestyle intervention group showed a tendency for greater weight loss. In both groups ALT and AST declined significantly. Triglycerides significantly decreased only in meal replacement group.With respect to liver fat quality the grade of saturation and mean chain length of hepatic fatty acids were quantifiable in a subset of participants. Total unsaturated lipids and mean chain length were significantly reduced only by meal replacement.
Research conclusions
With both interventions body fat and liver fat content were significantly reduced. Though the participants tended to lose more weight by lifestyle intervention the reduction of liver fat was comparable in both groups. Thus, for the reduction in liver fat a meal replacement strategy could be more effective in relation to body weight loss than a lifestyle intervention. This study confirms the finding of preserving muscle mass during a weight reduction period once high quality protein supplementation or physical activity is added in a guided and supervised manner. The pronounced reduction of serum triglycerides is attributed to specific soy properties.Given the study protocol further analysis of liver fat in humans by magnetic resonance spectroscopy was possible. Both interventions had different effects on liver fat quality.
In conclusion, with both approaches a significant weight loss and loss of intrahepatic fat content is achievable. Reduction in fat content is accompanied by a decline in hepatic inflammation, reflected in reduction of aminotransferases. In patients with NASH both therapeutic interventions can be advocated in order to reduce liver fat content and hepatic inflammation.
Research perspectives
Both interventions had distinct effects on liver fat quality. The reduction of serum triglycerides is a known effect of soy protein supplementation thus, we hypothesize that the different changes in liver fat quality were also related to soy protein intake. However, the physiologic consequence of a shortened chain length or of a different grade of saturation in hepatic lipids is not clear yet.This has to be addressed in future investigations. Furthermore, our research results demonstrated the practicability of magnetic resonance spectroscopy to analyze liver fat quality.The validity has to be confirmed by further studies.
杂志排行

World Journal of Gastroenterology的其它文章
- Liver stem cells: Plasticity of the liver epithelium
- Reaction of antibodies to Campylobacter jejuni and cytolethal distending toxin B with tissues and food antigens
- Integrated network analysis of transcriptomic and protein-protein interaction data in taurine-treated hepatic stellate cells
- Computed tomography scan imaging in diagnosing acute uncomplicated pancreatitis: Usefulness vs cost
- Targeted puncture of left branch of intrahepatic portal vein in transjugular intrahepatic portosystemic shunt to reduce hepatic encephalopathy
- Optimized protocol of multiple post-processing techniques improves diagnostic accuracy of multidetector computed tomography in assessment of small bowel obstruction compared with conventional axial and coronal reformations