Tobacco cessation pharmacotherapy use among racial/ethnic minorities in the United States: Considerations for primary care
2017-12-21MonicaWebbHooperMichaelPayneKimberlyParkinson
Monica Webb Hooper, Michael Payne, Kimberly A. Parkinson
1. Case Comprehensive Cancer Center, Case Western Reserve University, Cleveland, OH, USA
Tobacco cessation pharmacotherapy use among racial/ethnic minorities in the United States: Considerations for primary care
Monica Webb Hooper1, Michael Payne1, Kimberly A. Parkinson1
1. Case Comprehensive Cancer Center, Case Western Reserve University, Cleveland, OH, USA
Pharmacotherapies for tobacco cessation are efficacious and recommended during quit attempts. Racial/ethnic minorities in the United States are less likely to use medication-based aids for tobacco cessation, despite greater difficulty achieving long-term abstinence. The reasons for this include, among others, provider- and patient-level considerations. Primary care clinicians play an important role in encouraging racial/ethnic minority tobacco users to use cessation pharmacotherapy. To better understand pharmacotherapy use, we conducted a narrative review of patient-level factors that may determine uptake and adherence. This review indicates that social and cultural factors impact pharmacotherapy use, including health care experiences, beliefs, perceptions, and norms. The proportion of individuals using pharmacotherapy during quit attempts and adhering to the full course of treatment may be enhanced with greater attention to the ethnocultural concerns of these groups. Culturally appropriate assessment and brief advice delivered by primary care providers could yield significant benefits in population health. Recommendations for treating racial/ethnic tobacco users with pharmacotherapy for cessation are offered.
Tobacco cessation; pharmacotherapy; racial/ethnic minorities; primary care;physician advice; nicotine replacement therapy; varenicline; bupropion
Introduction
Racial/ethnic minorities in the United States are at heightened risk of tobacco-related morbidity and death [1—4]. These populations are also less likely to quit smoking successfully[5—13]. Smoking cessation pharmacotherapy combined with behavioral intervention is the recommended standard of care [14, 15], and both are critical components of any quit attempt[16]. However, racial/ethnic minorities are less likely to use Food and Drug Administration(FDA)-approved cessation aids [17, 18], and have been underrepresented in pharmacotherapy clinical trials. Primary care providers play a key role in primary and secondary prevention of disease, and are on the front line of tobacco education and treatment. There has been minimal progress in addressing tobacco-related disparities; thus developing methods to encourage provider-patient communication and increase both access and use of treatments is important. Improving our understanding of patient-level concerns regarding pharmacotherapy for tobacco cessation has the potential to enhance provider responsiveness and outcomes. The purpose of this article is to summarize factors associated with tobacco cessation pharmacotherapy use among US racial/ethnic minority populations and to recommend strategies for increasing the uptake of evidence-based treatment.
Provider advice to quit and racial/ethnic minorities
More than 70% of tobacco users visit a primary care provider annually [19], and many of these patients desire to quit.However, fewer than 10% are successful in a given year [20].This represents a captive group with significant interest in cessation and who may be influenced by clinician advice [21].Provider-delivered tobacco cessation advice is an evidencebased intervention [14, 22] that is positively associated with quit attempts [23]. Despite improvement in the delivery of tobacco cessation messages by providers [24], the rates of advice, assistance, and follow-up remain less than 60% [20,25]. The reasons include time constraints, other medical priorities, and insufficient training on cessation methods.Moreover, evidence indicates limited provider compliance in recommending and prescribing pharmacotherapy [26].
Compared with white smokers, racial/ethnic minority smokers are historically less likely to receive provider advice to quit [27—29], even after socioeconomic status and health care access have been controlled for [30]. Tobacco use assessment and advice to quit appears to be particularly low among African Americans [31] and Hispanics [32]. However, some research has found no racial/ethnic differences in the receipt of provider advice [12]. Another concern is that providers may misperceive the subset of patients with low health literacy,those with limited English language fl uency, or those who do not understand self-care instructions (e.g., how and when to take medication) as nonadherent [33, 34]. Overall, there is a need to increase the delivery and effectiveness of provider assistance to racial/ethnic minority tobacco users interested in quitting.
Efficacy of pharmacologic tobacco cessation treatment among racial/ethnic minorities
Each of the FDA-approved pharmacologic cessation aids (nicotine patches, gum, lozenge, inhaler and nasal spray, bupropion,and varenicline) have demonstrated efficacy in multiple randomized clinical trials [35, 36]. Indeed, more than 150 therapeutic trials have tested the efficacy of nicotine replacement therapies (NRTs), and their use increases the likelihood of cessation by 50%—70% compared with control conditions [35].Systematic reviews have recommended pharmacotherapy for tobacco cessation among US racial/ethnic minority populations[37, 38]. However, the small number of studies examining pharmacotherapy effects in these populations may preclude firm conclusions. For instance, the Robles et al. [37] review included only one trial among Hispanics, one among Native Americans,and none among Asian Americans. When examined closely,the findings from the extant randomized clinical trials testing the efficacy of pharmacotherapies among racial/ethnic minority groups are equivocal. Some studies suggest that treatment with nicotine gum is no better than use of placebo [39], and that bupropion has a short-term impact on cessation among treatment-seeking African American smokers [40]. Initial evidence suggests that both NRT and varenicline may be less effective in lower socioeconomic status predominantly racial/ethnic minority primary care patients [41]. Other research, however, found no differences in NRT effectiveness by race/ethnicity [42]. Thus more research evaluating the effectiveness of pharmacotherapy among racial/ethnic minority tobacco users is warranted.
Perceptions of pharmacotherapy among racial/ethnic minorities
Consumer beliefs and risk perceptions are significant patientlevel variables that contribute to the underuse of tobacco cessation pharmacotherapy. Across racial/ethnic groups, evidence-based cessation aids are underused, and tobacco users report limited NRT knowledge [43, 44], which can result in erroneous beliefs regarding the effectiveness and perceived side effects, and can lead to safety concerns [45]. Tobacco smokers, in general, have also reported concerns about NRT addiction potential and possible interactions with other medications [43]. While there may be widespread concern and misperceptions regarding pharmacotherapy, white non-Hispanics remain more likely to have greater access to tobacco pharmacotherapies and thus use them more frequently and consistently. From the perspective of addressing tobacco cessation disparities, it is critical that we take a closer look at possible reasons for underuse among racial/ethnic minorities.
Relatively few studies have focused on perceptions of FDA-approved cessation aids in racial/ethnic minority populations.
However, because of the lower propensity of use compared with that in whites [12, 17, 28, 30, 38, 46—49], this warrants attention. Here, we summarize research examining attitudes and beliefs around pharmacologic tobacco cessation aids among African Americans, Hispanics, American Indians/Native Alaskans, and Asian Americans/Pacific Islanders. As can be seen in Table 1, most of the extant literature includes qualitative research. Qualitative studies allow the patients’ voices to be heard in rich, nuanced, and contextualized ways, thus facilitating theory development and hypothesis generation. Finally,it is important to note the inherent within-group heterogeneity of groups categorized by race/ethnicity. Ethnocultural groups share some common beliefs, traditions, and experiences, yet there are individual differences that must be considered to prevent stereotyping and overgeneralizing.
African Americans
Compared with white smokers, African American smokers are less likely to use pharmacologic aids during cessation attempts[12, 17, 30, 49]. Moreover, pharmacotherapy adherence among treatment-seeking African Americans is approximately 50%[57], and thus has significant room for improvement. Outcome expectancies are an important contributor to behavior and decision-making, and African Americans appear to have less confidence in the effectiveness of tobacco interventions relative to white smokers [50], which may, in part, provide a patient-level explanation. A cross-sectional survey of current smokers found that compared with whites, African Americans reported concern about pharmacotherapy addiction potential and were less likely to endorse the need for tobacco cessation treatment, which were predictive of pharmacotherapy uptake[49]. These findings are consistent with those of qualitative studies. For instance, a qualitative study, including a racially/ethnically diverse sample, found that compared with white and Hispanic smokers, African American smokers expressed suspicion of the pharmaceutical industry and government, and concerns regarding the “unknowns” about NRT [43]. Similar beliefs and concerns were described in a seminal qualitative study of African American smokers, which found that participants viewed NRT as unfamiliar and concerning, and reported concerns about NRT dosing, and the inability to control nicotine absorption into the body [51]. The hesitation to use pharmacotherapy may stem, in part, from negative experiences within the health care system and medical mistrust [52],which is rooted in a long history of mistreatment and denial of health care.
Hispanics/Latinos
Hispanic smokers are significantly less likely than white smokers to have used pharmacotherapy during quit attempts[17, 18, 46]. A few studies have attempted to unpack this consistent finding. A seminal qualitative study among Hispanic smokers who reported at least one previous-year quit attempt identified themes including the general avoidance of medication, tobacco cessation misconceptions, distrust, and rejection of pharmacotherapy [53]. Participants also conceptualized the act of smoking as a weakness, rather than an illness to be medicated. These findings may reflect an incongruence between pharmacotherapy use and cultural values, such as hard work and determination [27]. Hispanic smokers report confidence that NRT has the potential to reduce cravings, yet may have negative perceptions [53], and disbelieve that these products contain nicotine [43]. Relative to other racial/ethnic groups, Hispanic smokers may also believe that the use of NRT represents a personal vulnerability. That is, tobacco cessation can be accomplished by relying on willpower and self- determination [43]. The belief that willpower alone is sufficient to quit smoking among Hispanics is consistent with population-level quantitative findings [44]. Thus, seeking professional help or pharmacotherapy use may represent an individual weakness or a departure from this belief [27].
American Indians/Native Alaskans
A minority of American Indian or Native Alaskan tobacco smokers report using pharmacotherapy for cessation [29, 55,58]. Indeed, this group has the lowest pharmacotherapy use rates of all racial/ethnic categories in the United States [48]. A quantitative survey conducted among self-identified American Indians found low pharmacotherapy awareness among current smokers, particularly the nicotine lozenge, varenicline,and bupropion [54]. Few studies have examined perceptions regarding cessation pharmacotherapies in this population, yet the extant data suggest that cultural factors may offer some insight. A qualitative study among current and former smokersfound that while participants expressed a desire to quit, most did not use pharmacotherapy (or counseling) during quit attempts [29]. Important themes emerged, including overall concern about conventional medication, coupled with apprehension about pharmacotherapy side effects and effectiveness[29]. Participants also expressed distrust related to racism.These findings were consistent with those of another qualitative investigation including American Indians, specifically,reservations regarding pharmacotherapy being rooted in a history of negative experiences with the health care system [52],lack of awareness, and limited knowledge about these products [29]. Finally, Choi et al. [55] found that accessibility and cost may also present major barriers to use among American Indian adult smokers.
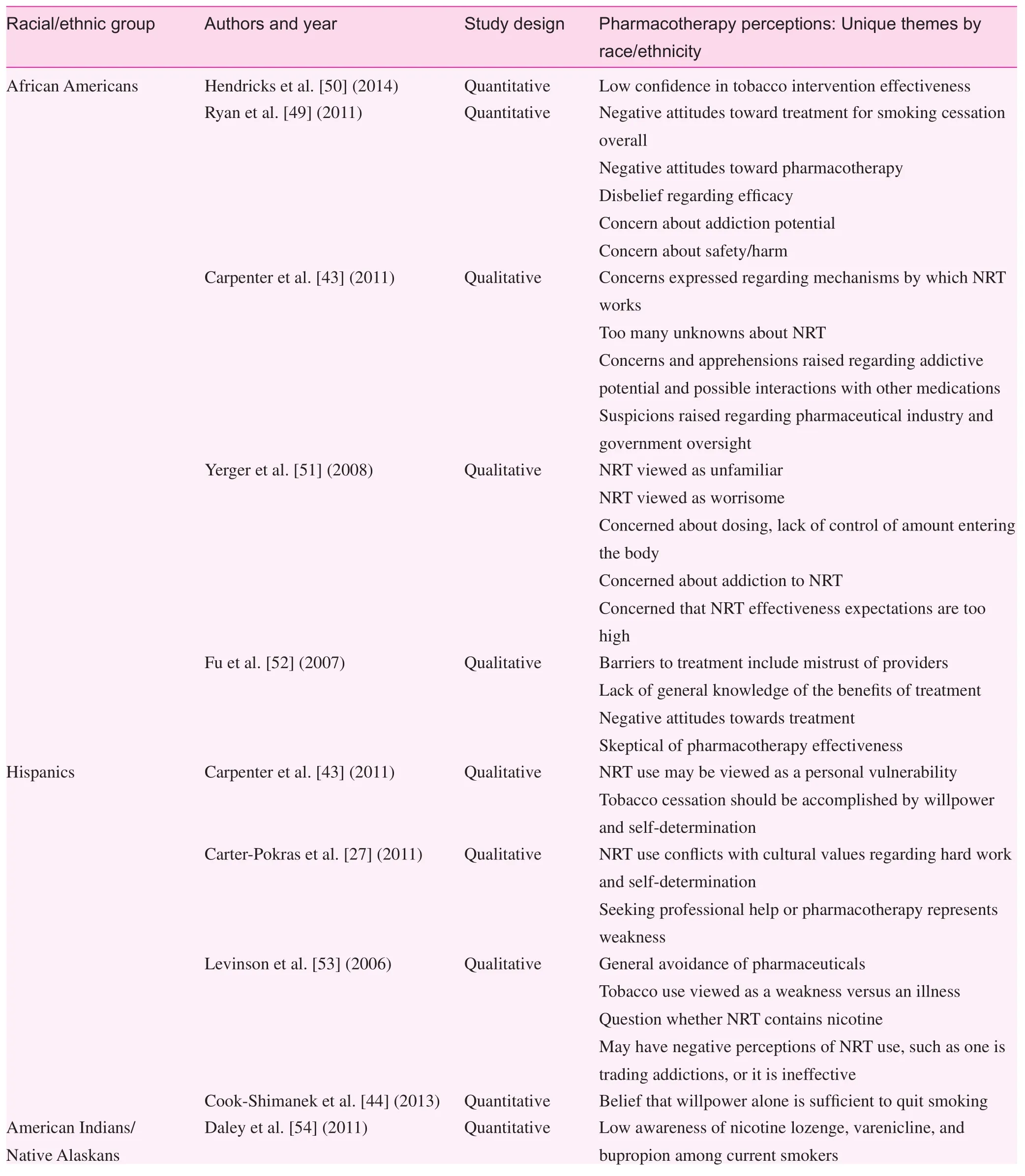
Table 1. Summary of research examining attitudes and beliefs around pharmacologic tobacco cessation aids among African Americans,Hispanics, American Indians/Native Alaskans, and Asian Americans/Pacific Islanders
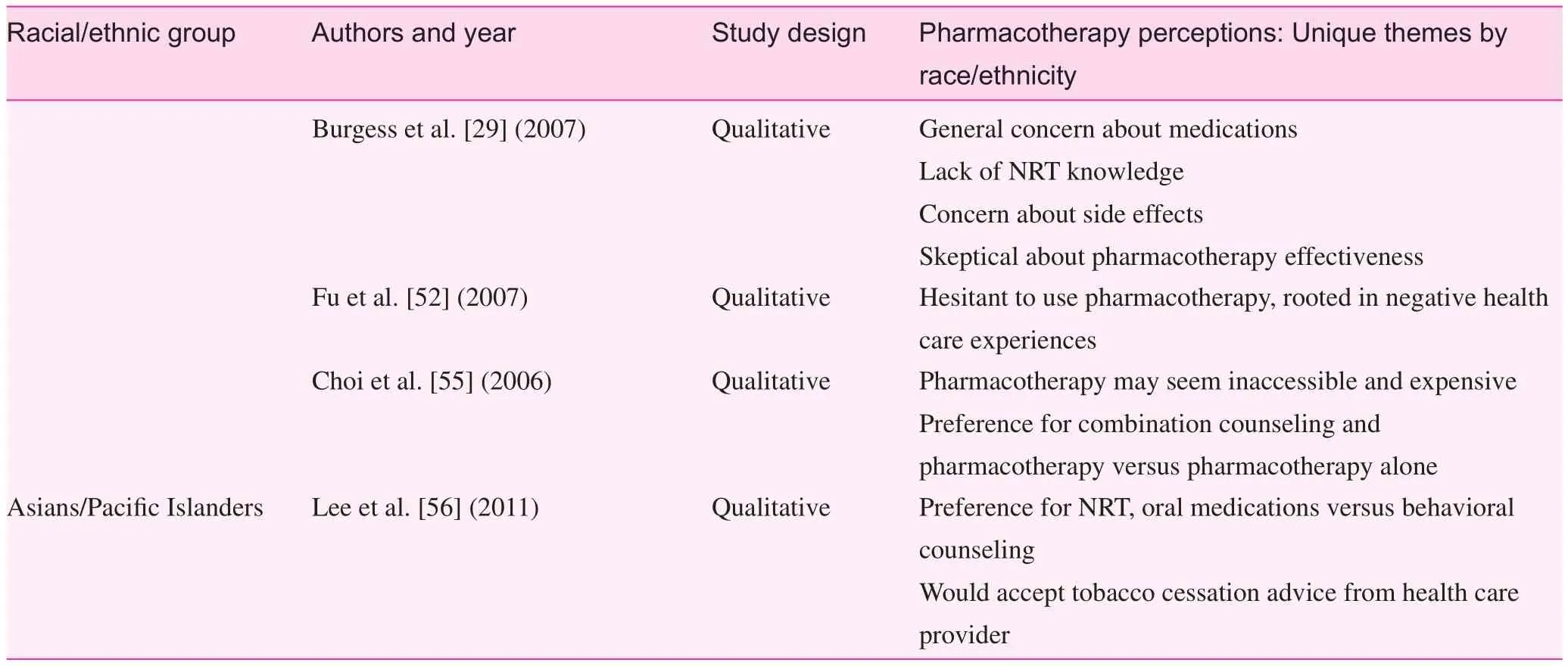
Table 1 (continued)
Asian Americans and Pacific Islanders
Asian Americans and Pacific Islanders are less likely to use tobacco cessation pharmacotherapy compared with whites[12], although this difference may be nonsignificant after adjustment for covariates [47]. The underuse of cessation aids among Asian Americans may be related to low rates of provider advice to quit [59]. There is a paucity of research examining perceptions of pharmacotherapy among Asian Americans or Pacific Islanders. Qualitative research among Vietnamese and Hmong smokers found that while medical providers were viewed positively, they were not perceived as resources for tobacco cessation [52]. The Vietnamese participants, in particular, discussed the cultural values of mental control and self-determination as important for quitting. We also found one focus group study of Asian or Pacific Islander adult smokers who lived with a hospitalized child [56]. The findings suggested that NRT and oral medications were preferred over behavioral counseling. In addition, smokers with high readiness to quit expressed a desire for clinician advice.Additional research seeking to understand pharmacotherapy use barriers among Asian Americans is needed.
Discussion and recommendations
Tobacco cessation disparities may be attributed to multiple variables, including health care system factors and individual factors — such as access to and use of evidence-based pharmacotherapies [60]. Provider advice to quit in the primary care setting may be more effective for population health than policy changes (e.g., increasing taxes and smoking bans) [22]. There is a tremendous opportunity for primary care providers to take a more active role in meeting the unique needs of racial/ethnic minority smokers. Recognizing racial/ethnic cultural factors and perspectives about pharmacotherapy is necessary for the development of successful strategies to improve both uptake and adherence. On the basis of the studies summarized above,we offer the following recommendations (Table 2).
Recommendation 1: Develop a working knowledge of possible pharmacotherapy barriers among racial/ethnic minorities
Patient-level barriers appear to be based in historical, current,and cultural factors that influence interest and uptake of these treatments. Across groups, lack of knowledge was consistently reported, and represents a barrier to the accessibility and use of these products. Health care providers have the opportunity to introduce pharmacotherapy options to tobacco users. In doing so, they also have the opportunity to address barriers and to dispel myths regarding use. Another trans-group similarity was the notion of medical distrust. Racial/ethnic minority experiences within the health care system and/or concern about the intentions of pharmaceutical companies may lead to reservations about medications for tobacco cessation.Overcoming these long-standing barriers will require health care professionals to employ more empathetic responses and expressions of concern for patients’ well-being.
There were also notable distinctions in pharmacotherapy perceptions across racial/ethnic minority groups. The current research suggested that skepticism about pharmacotherapy effectiveness was among the foremost concerns of African American smokers, followed by becoming addicted to NRT.In contrast, Hispanics were distinguished by a cultural conflict between the need for a cessation aid and personal weakness.American Indians/Native Alaskans seemed most concernedabout taking medications in general, and expressed a desire for behavioral support. Finally, the one study conducted in a sample of Asians/Pacific Islanders suggested that this population may be open to pharmacotherapy, particularly when prescribed by a health care professional. Additional research in each of these populations is needed to enhance our understanding of social and cognitive factors that serve as barriers to cessation treatment.
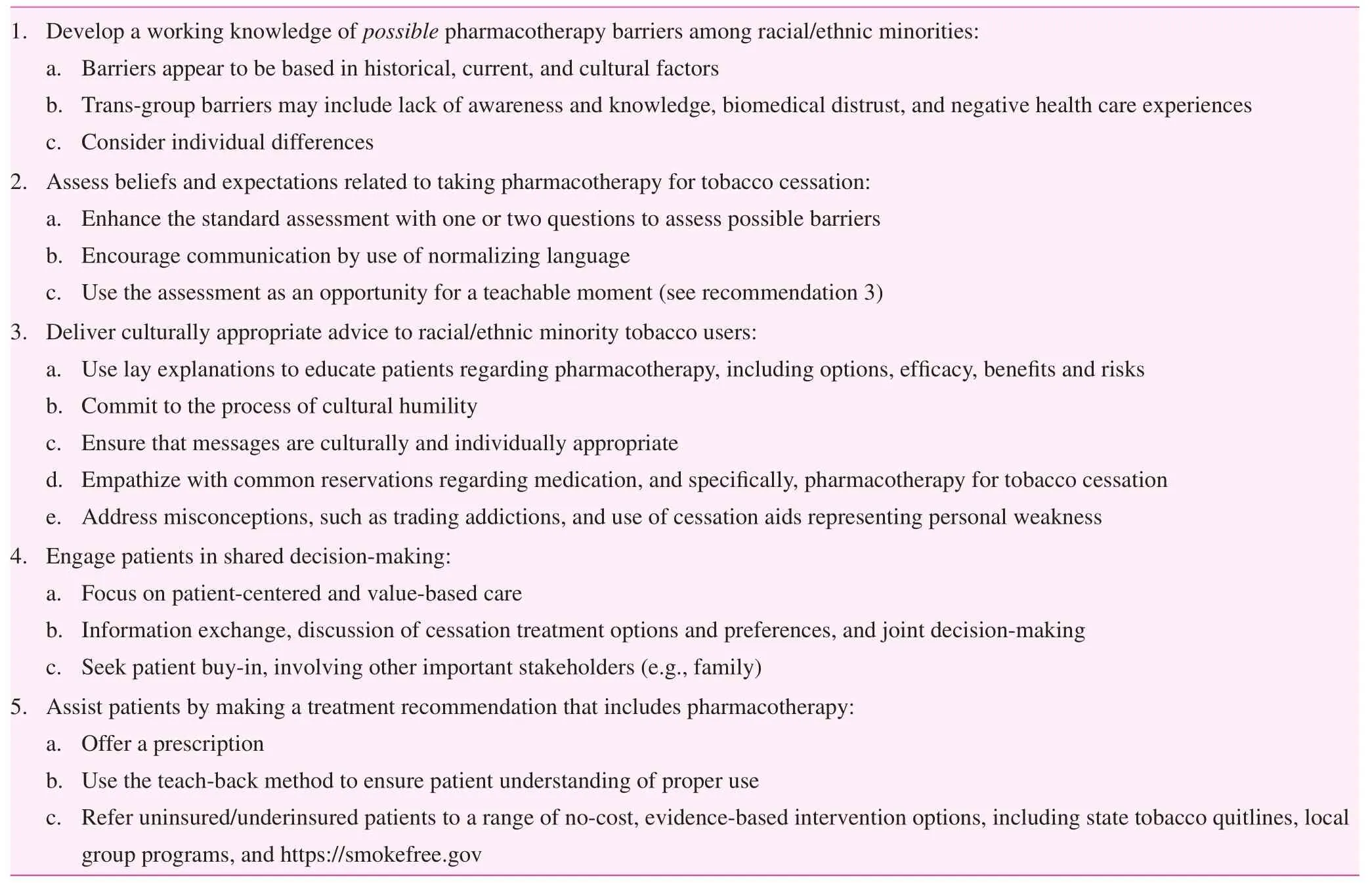
Table 2. Tobacco cessation pharmacotherapy among US racial/ethnic minorities: Provider recommendations
Knowledge of factors that may influence the care of racial/ethnic minority tobacco smokers is important for the delivery of culturally appropriate communication and for satisfactory clinical encounters [61]. However, racial/ethnic group cultural beliefs and practices are not monolithic; there is significant within-group heterogeneity (i.e., individual differences) that must be considered. Understanding the interrelatedness of race, ethnicity, socioeconomic status, cultural context, and geography will offer valuable insights to clinicians. Efforts to learn more about these variables represent an approach to addressing health care inequities.
Recommendation 2: Assess beliefs and expectations related to use of pharmacotherapy for tobacco cessation
In addition to the standard assessment and documentation of tobacco use [14], providers treating racial/ethnic minority tobacco smokers are encouraged to assess patients’ treatment preferences and barriers to uptake and adherence. Previous research among African American light smokers found inadequate treatment adherence to bupropion therapy in a sample of treatment-seekers [62]. The use of pharmacotherapy for tobacco cessation may be incongruent with the cultural orientation (i.e., norms, beliefs, and practices) of patients. For example, a 50-year-old Hispanic male and current smoker who presents in a primary care clinic may believe that smoking is a just bad habit and a sign of vulnerability. He may also be generally avoidant of medication. A brief assessment of beliefs regarding NRT as a cessation aid would allow a“teachable moment”; that is, an opportunity for patient education regarding the neurobiology of nicotine dependence and the benefits of NRT for withdrawal management after cessation. Assessment items might include: “What would you think about using the nicotine patch or gum to help you quit smoking?” or “What would you expect from a medication to help you quit?” Normalizing language designed to elicit barriers can also be used, including “Some people have concerns (or worries) about using NRT or a pill to help them quit smoking. What are your thoughts?” Such questions can enhance the standard assessment and inform providers about whether the issues identified in this review (and others) are relevant for the individual patient.
Recommendation 3: Deliver culturally appropriate advice to racial/ethnic minority tobacco users
Patient education about the many health risks of persistent smoking is important for primary and secondary prevention as well as for reducing tobacco-related disparities. When racial/ethnic minority patients are being treated, information about pharmacologic aids is needed regarding efficacy and safety,and also development and regulation. Health care professionals have a particularly important role in promoting wider use of evidence-based cessation strategies [43]. Indeed, there are positive associations between quality provider-patient communication and medication adherence and treatment satisfaction [63].There is long-standing evidence that compared with whites, racial/ethnic minorities perceive health care system—wide biases, including provider bias [64]. Compared with whites, racial/ethnic minority patients may experience lower self-efficacy for medical decision-making and lower quality of care [65]. Many racial/ethnic minority smokers who desire to quit would be open to pharmacotherapy use, if it is accessible and discussed by providers [29, 46, 66]. Provider communication should be based directly on the enhanced assessment of tobacco use, and tailored to patients’ unique barriers and concerns. Concerns regarding proper dosing[12, 37, 51], NRT addiction [53], and side effects [29] should be discussed proactively with patients. In doing so, providers should normalize and validate concerns (e.g., suspicion of the pharmaceutical industry), but need not identify potential barriers as being common among racial/ethnic minorities. Language such as the following should be used: “It is common to have concerns about the motives of drug companies. Fortunately, varenicline has been tested in many studies outside of the pharmaceutical industry and has helped more patients quit compared with a placebo (or a pill without medication).”
Recommendation 4: Engage patients in shared decision-making
Established models of provider-patient communication, such as the shared decision-making model [67], emphasize patientcentered care and value-based care. Evidence suggests that unmet provider communication needs may be magnified among racial/ethnic minority patients [68]. In the current context, providers would facilitate an information exchange,followed by a discussion of cessation treatment options and preferences, and a joint decision. Indeed, shared decisionmaking is positively associated with treatment adherence and timely care [69]. A systematic review found that the shared decision-making process for racial/ethnic minorities should be extended beyond patients and providers to include other important stakeholders, such as family members [68].
Recommendation 5: Assist patients by making a treatment recommendation that includes pharmacotherapy
Increasing access to tobacco cessation treatment is important for reducing tobacco-related disparities. Patients with health insurance are more likely to receive provider advice to quit[59], an association that may contribute to health care inequities. Providers should be aware of publicly available, evidencebased, tobacco cessation options that are available at no cost.These resources include state tobacco quitlines, group cessation programs in the community or hospitals, mobile applications, and text messaging programs. Many state quitlines and hospital-based programs also offer NRT.
Conclusion
In conclusion, racial/ethnic minorities suffer disproportionately from tobacco use, and access to cessation aids is sorely needed.At both the health system level and the provider level, equity in treatment access, education, and advice to quit is needed to increase use. There are modifiable patient-level reasons for underuse that we need to better understand and address. Providers are encouraged to embrace multiculturalism through the process of cultural humility. In the care of patients from diverse backgrounds, cultural humility is a multifaceted learning process of openness, self-awareness, and self-critique, which can result in mutual empowerment, partnerships, and optimal clinical care[70]. In primary care settings, providing culturally appropriate advice and making a pharmacotherapy recommendation are vital. When pharmacotherapy is prescribed as an adjunct to behavioral counseling, uptake among racial/ethnic minorities can be high. With greater attention to the ethnocultural concerns of these groups, providers can encourage pharmacotherapy use and adherence, and play an integral role in reducing and eliminating racial/ethnic tobacco-related disparities.
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
1. Centers for Disease Control and Prevention. CDC health disparities and inequalities report — United States, 2011. MMWR Morb Mortal Wkly Rep 2011;60(Suppl):1—114.
2. Margerison-Zilko C, Cubbin C. Socioeconomic disparities in tobacco-related health outcomes across racial/ethnic groups in the United States: national health interview survey 2010. Nicotine Tob Res 2013;15(6):1161—5.
3. Green PM, Guerrier-Adams S, Okunji PO, Schiavone D, Smith JE. African American health disparities in lung cancer. Clin J Oncol Nurs 2013;17(2):180—6.
4. Henley SJ, Thomas CC, Sharapova SR, Momin B, Massetti GM,Winn DM, et al. Vital signs: disparities in tobacco-related cancer incidence and mortality — United States, 2004—2013. MMWR Morb Mortal Wkly Rep 2016;65(44):1212—8.
5. Delnevo CD, Gundersen DA, Hrywna M, Echeverria SE,Steinberg MB. Smoking-cessation prevalence among US smokers of menthol versus non-menthol cigarettes. Am J Prev Med 2011;41(4):357—65.
6. Giovino GA, Villanti AC, Mowery PD, Sevilimedu V, Niaura RS,Vallone DM, et al. Differential trends in cigarette smoking in the USA: is menthol slowing progress? Tob Control 2015;24(1):28—37.
7. Sheffer CE, Stitzer M, Landes R, Brackman SL, Munn T, Moore P. Socioeconomic disparities in community-based treatment of tobacco dependence. Am J Public Health 2012;102(3):e8—16.
8. Covey LS, Botello-Harbaum M, Glassman AH, Masmela J,LoDuca C, Salzman V, et al. Smokers’ response to combination bupropion, nicotine patch, and counseling treatment by race/ethnicity. Ethnic Dis 2008;18(1):59—64.
9. Honda K. Psychosocial correlates of smoking cessation among elderly ever-smokers in the United States. Addict Behav 2005;30(2):375—81.
10. Holford TR, Levy DT, Meza R. Comparison of smoking history patterns among African American and white cohorts in the United States born 1890 to 1990. Nicotine Tob Res 2016;18:S16—29.
11. Kulak J, Cornelius ME, Fong GT, Giovino GA. Differences in quit attempts and cigarette smoking abstinence between whites and African Americans in the United States: literature review and results from the International Tobacco Control US Survey. Nicotine Tob Res 2016;18:S79—87.
12. Trinidad DR, Perez-Stable EJ, White MM, Emery SL, Messer K.A nationwide analysis of US racial/ethnic disparities in smoking behaviors, smoking cessation, and cessation-related factors. Am J Public Health 2011;101(4):699—706.
13. Gohdes D, Harwell TS, Cummings S, Moore KR, Smilie JG,Helgerson SD. Smoking cessation and prevention: an urgent public health priority for American Indians in the Northern Plains.Public Health Rep 2002;117(3):281—90.
14. Fiore MC, Jaen CR, Baker TB, Bailey WC, Bennett G, Benowitz NL, et al. A clinical practice guideline for treating tobacco use and dependence: 2008 Update — a US Public Health Service report. Am J Prev Med 2008:35(2):158—76.
15. Fiore MC, Baker TB. Treating smokers in the health care setting.New Engl J Med 2011;365(13):1222—31.
16. Stead LF, Koilpillai P, Fanshawe TR, Lancaster T. Combined pharmacotherapy and behavioural interventions for smoking cessation. Cochrane Database Syst Rev 2016;(3):CD008286. DOI:10.1002/14651858.CD008286.pub3.
17. Fu SS, Sherman SE, Yano EM, van Ryn M, Lanto AB, Joseph AM. Ethnic disparities in the use of nicotine replacement therapy for smoking cessation in an equal access health care system. Am J Health Promot 2005:20(2):108—16.
18. Sias JJ, Urquidi UJ, Bristow ZM, Rodriguez JC, Ortiz M. Evaluation of smoking cessation behaviors and interventions among Latino smokers at low-income clinics in a US-Mexico border county. Addict Behav 2008;33(2):373—80.
19. Jamal A, Dube SR, Malarcher AM, Shaw L, Engstrom MC.Tobacco use screening and counseling during physician office visits among adults — National Ambulatory Medical Care Survey and National Health Interview Survey, United States, 2005—2009.MMWR Morb Mortal Wkly Rep 2012;61 Suppl:38—45.
20. Babb S, Malarcher A, Schauer G, Asman K, Jamal A. Quitting smoking among adults — United States, 2000—2015. MMWR Morb Mortal Wkly Rep 2017;65(52):1457—64.
21. Kreuter MW, Chheda SG, Bull FC. How does physician advice influence patient behavior? Evidence for a priming effect. Arch Fam Med 2000;9(5):426—33.
22. Bao Y, Duan N, Fox SA. Is some provider advice on smoking cessation better than no advice? An instrumental variable analysis of the 2001 National Health Interview Survey. Health Serv Res 2006;41(6):2114—35.
23. Davila EP, Zhao W, Byrne M, Webb M, Huang Y, Arheart K,et al. Correlates of smoking quit attempts: Florida Tobacco Callback Survey, 2007. Tob Induc Dis 2009;5:10.
24. Schmittdiel JA, Barrow JC, Wiley D, Ma L, Sam D, Chau CV,et al. Improvements in access and care through the Affordable Care Act. Am J Manag Care 2017;23(3):e95—7.
25. Schauer GL, Wheaton AG, Malarcher AM, Croft JB. Healthcare provider screening and advice for smoking cessation among smokers with and without COPD: 2009—2010 National Adult Tobacco Survey. Chest 2016;149(3):676—84.
26. Balls JE, Price JH, Dake JA, Jordan TR, Khuder S. African American primary care physicians’ perceptions and practices regarding smoking cessation therapy. J Natl Med Assoc 2010;102(7):579—89.27. Carter-Pokras OD, Feldman RH, Kanamori M, Rivera I, Chen L, Baezconde-Garbanati L, et al. Barriers and facilitators to smoking cessation among Latino adults. J Natl Med Assoc 2011;103(5):423—31.
28. Levinson AH, Perez-Stable EJ, Espinoza P, Flores ET, Byers TE.Latinos report less use of pharmaceutical aids when trying to quit smoking. Am J Prev Med 2004;26(2):105—11.
29. Burgess D, Fu SS, Joseph AM, Hatsukami DK, Solomon J,van Ryn M. Beliefs and experiences regarding smoking cessation among American Indians. Nicotine Tob Res 2007;9(Suppl 1):S19—28.
30. Cokkinides VE, Halpern MT, Barbeau EM, Ward E, Thun MJ.Racial and ethnic disparities in smoking-cessation interventions:analysis of the 2005 National Health Interview Survey. Am J Prev Med 2008;34(5):404—12.
31. Palmer RC, McKinney S. Health care provider tobacco cessation counseling among current African American tobacco users.J Natl Med Assoc 2011;103(8):660—7.
32. Danesh D, Paskett ED, Ferketich AK. Disparities in receipt of advice to quit smoking from health care providers: 2010 National Health Interview Survey. Prev Chronic Dis 2014;11:E131.
33. Graham S, Brookey J. Do patients understand? Permanente J 2008;12(3):67—9.
34. Taylor SP, Nicolle C, Maguire M. Cross-cultural communication barriers in health care. Nurs Stand 2013:27(31):35—43.
35. Stead LF, Perera R, Bullen C, Mant D, Hartmann-Boyce J,Cahill K, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev 2012;(11):CD000146. DOI:10.1002/14651858.CD000146.pub4.
36. Garrison GD, Dugan SE. Varenicline: a first-line treatment option for smoking cessation. Clin Ther 2009;31(3):463—91.
37. Robles GI, Singh-Franco D, Ghin HL. A review of the efficacy of smoking-cessation pharmacotherapies in nonwhite populations.Clin Ther 2008;30(5):800—12.
38. Cox LS, Okuyemi K, Choi WS, Ahluwalia JS. A review of tobacco use treatments in US ethnic minority populations. Am J Health Promot 2011;25(5):S11—30.
39. Ahluwalia JS, Okuyemi K, Nollen N, Choi WS, Kaur H, Pulvers K, et al. The effects of nicotine gum and counseling among African American light smokers: a 2×2 factorial design. Addiction 2006;101(6):883—91.
40. Faseru B, Nollen NL, Mayo MS, Krebill R, Choi WS, Benowitz NL, et al. Predictors of cessation in African American light smokers enrolled in a bupropion clinical trial. Addict Behav 2013;38(3):1796—803.
41. Dhelaria RK, Friderici J, Wu K, Gupta E, Khan C, Rothberg MB.Effectiveness of varenicline for smoking cessation at 2 urban academic health centers. Eur J Intern Med 2012;23(5):461—4.
42. Fu SS, Burgess DJ, Hatsukami DK, Noorbaloochi S, Clothier BA, Nugent S, et al. Race and nicotine replacement treatment outcomes among low-income smokers. Am J Prev Med 2008;35(6 Suppl):S442—8.
43. Carpenter MJ, Ford ME, Cartmell K, Alberg AJ. Misperceptions of nicotine replacement therapy within racially and ethnically diverse smokers. J Natl Med Assoc 2011;103(9—10):885—94.
44. Cook-Shimanek M, Burns EK, Levinson AH. Medicinal nicotine nonuse: smokers’ rationales for past behavior and intentions to try medicinal nicotine in a future quit attempt. Nicotine Tob Res 2013;15(11):1926—33.
45. Amodei N, Lamb RJ. Over-the-counter nicotine replacement therapy: can its impact on smoking cessation be enhanced? Psychol Addict Behav 2008;22(4):472—85.
46. Sedjo RL, Li Y, Levinson AH. Smoking-cessation treatment: use trends among non-Hispanic white and English-speaking Hispanic/Latino smokers, Colorado 2001—2012. Am J Prev Med 2016;51(2):232—9.
47. Fu SS, Kodl MM, Joseph AM, Hatsukami DK, Johnson EO,Breslau N, et al. Racial/ethnic disparities in the use of nicotine replacement therapy and quit ratios in lifetime smokers ages 25 to 44 years. Cancer Epidemiol Biomarkers Prev 2008;17(7):1640—7.
48. Stahre M, Okuyemi KS, Joseph AM, Fu SS. Racial/ethnic differences in menthol cigarette smoking, population quit ratios and utilization of evidence-based tobacco cessation treatments.Addiction 2010;105:75—83.
49. Ryan KK, Garrett-Mayer E, Alberg AJ, Cartmell KB, Carpenter MJ. Predictors of cessation pharmacotherapy use among black and non-Hispanic white smokers. Nicotine Tob Res 2011;13(8):646—52.
50. Hendricks PS, Westmaas JL, Park VMT, Thorne CB, Wood SB, Baker MR, et al. Smoking abstinence-related expectancies among American Indians, African Americans, and women:potential mechanisms of tobacco-related disparities. Psychol Addict Behav 2014;28(1):193—205.
51. Yerger VB, Wertz M, McGruder C, Froelicher ES, Malone RE.Nicotine replacement therapy: perceptions of African-American smokers seeking to quit. J Natl Med Assoc 2008;100(2):230—6.
52. Fu SS, Burgess D, van Ryn M, Hatsukami DK, Solomon J,Joseph AM. Views on smoking cessation methods in ethnic minority communities: a qualitative investigation. Prev Med 2007;44(3):235—40.
53. Levinson AH, Borrayo EA, Espinoza P, Flores ET, Perez-Stable EJ. An exploration of Latino smokers and the use of pharmaceutical aids. Am J Prev Med 2006;31(2):167—71.
54. Daley CM, Faseru B, Nazir N, Solomon C, Greiner KA, Ahluwalia JS, et al. Influence of traditional tobacco use on smoking cessation among American Indians. Addiction 2011;106(5):1003—9.
55. Choi WS, Daley CM, James A, Thomas J, Schupbach R,Segraves M, et al. Beliefs and attitudes regarding smoking cessation among American Indians: a pilot study. Ethn Dis 2006;16(1):35—40.
56. Lee MT, Bracamontes J, Mosier E, Davis J, Maddock JE. Preferred smoking cessation methods for Asian or Pacific Islander household smokers who live with hospitalized children. Hawaii Med J 2011;70(3):48—51.
57. King A, Sachez-Johnsen L, Van Orman S, Cao D, Matthews A. A pilot community-based intensive smoking cessation intervention in African Americans: feasibility, acceptability and early outcome indicators. J Natl Med Assoc 2008;100(2):208—17.
58. Hodge FS, Casken J. Characteristics of American Indian women cigarette smokers: prevalence and cessation status. Health Care Women Int 1999;20:455—69.
59. Tong EK, Tang H, Chen MS Jr, McPhee SJ. Provider smoking cessation advice among California Asian-American smokers.Am J Health Promot 2011;25(5 Suppl):S70—4.
60. Barnoya J, Jin L, Hudmon KS, Schootman M. Nicotine replacement therapy, tobacco products, and electronic cigarettes in pharmacies in St. Louis, Missouri. J Am Pharm Assoc 2015;55(4):405—12.
61. Eiser AR, Ellis G. Viewpoint: cultural competence and the African American experience with health care: the case for specific content in cross-cultural education. Acad Med 2007;82(2):176—83.
62. Nollen NL, Mayo MS, Ahluwalia JS, Tyndale RF, Benowitz NL,Faseru B, et al. Factors associated with discontinuation of bupropion and counseling among African American light smokers in a randomized clinical trial. Ann Behav Med 2013;46(3):336—48.
63. White RO, Eden S, Wallston KA, Kripalani S, Barto S, Shintani A, et al. Health communication, self-care, and treatment satisfaction among low-income diabetes patients in a public health setting. Patient Educ Couns 2015;98(2):144—9.
64. Johnson RL, Saha S, Arbelaez JJ, Beach MC, Cooper LA.Racial and ethnic differences in patient perceptions of bias and cultural competence in health care. J Gen Intern Med 2004;19(2):101—10.
65. Palmer NRA, Kent EE, Forsythe LP, Arora NK, Rowland JH, Aziz NM, et al. Racial and ethnic disparities in patient-provider communication, quality-of-care ratings, and patient activation among long-term cancer survivors. J Clin Oncol 2014;32(36):4087—94.
66. D’Silva J, Schillo BA, Sandman NR, Leonard TL, Boyle RG.Evaluation of a tailored approach for tobacco dependence treatment for American Indians. Am J Health Promot 2011;25(5 Suppl):S66—9.
67. Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango). Soc Sci Med 1997;44(5):681—92.
68. Mead EL, Doorenbos AZ, Javid SH, Haozous EA, Alvord LA,Flum DR, et al. Shared decision-making for cancer care among racial and ethnic minorities: a systematic review. Am J Public Health 2013;103(12):e15—29.
69. Arora NK. Interacting with cancer patients: the signifi-cance of physicians’ communication behavior. Soc Sci Med 2003;57(5):791—806.
70. Foronda C, Baptiste DL, Reinholdt MM, Ousman K. Cultural humility: a concept analysis. J Transcult Nurs 2016;27(3):210—7.
Monica Webb Hooper
Case Comprehensive Cancer Center, Case Western Reserve University School of Medicine,Cleveland, OH 44106, USA
Tel.: +1-216-3686895
E-mail: mwh54@case.edu
19 April 2017;
Accepted 31 July 2017
杂志排行

Family Medicine and Community Health的其它文章
- Health is primary
- Assessing the accuracy of patient report of the 5As (ask, assess,advise, assist, and arrange) for smoking cessation counseling
- Mental health problems due to community violence exposure in a small urban setting
- Burden of road traffic accidents in Nepal by calculating disability- adjusted life years
- Effect of an educational intervention and parental vaccine refusal forms on childhood vaccination rates in a clinic with a large Somali population
- Understanding cultures beyond medicine