人黑素瘤药物研究进展
2017-11-10付靖波张红霞朱海英
付靖波, 于 斌, 张红霞, 朱海英*
1. 海军军医大学基础部细胞生物学教研室,上海200433 2. 复旦大学生命科学院,上海200433
·综述·
人黑素瘤药物研究进展
付靖波1, 于 斌2, 张红霞1, 朱海英1*
1. 海军军医大学基础部细胞生物学教研室,上海200433 2. 复旦大学生命科学院,上海200433
黑素瘤患者死亡率较高。其治疗方法除了传统的手术切除和放射治疗外,化疗一度成为主要的治疗手段。近年来,随着人们对黑素瘤发生发展分子机制的深入研究,基于靶向治疗、生物免疫治疗的方法和药物不断涌现。目前,除了已经在临床治疗中使用的药物外,一些正在进行临床研究的待批准药物和正进行基础研究的潜在药物也表现出良好的应用前景。本文就目前治疗黑素瘤的代表性药物及潜在药物的分子机制及治疗效果作一综述。
黑素瘤;多药联合治疗;生物免疫治疗;靶向治疗
黑素瘤起源于皮肤、黏膜和色素膜的黑素细胞。虽然黑素瘤的发病率低于基底细胞癌和鳞状细胞癌,但由于其易发生淋巴和血行转移,且易转移到肺、脑等器官,因此患者死亡率高。据统计,皮肤癌患者中仅4%的人罹患黑素瘤,但因皮肤癌死亡的患者中有80%为黑素瘤患者[1]。近年来,虽然多种肿瘤的发病增长率开始下降,但黑素瘤的发病增长率仍以每年3%增长[2]。广泛切除联合选择性的淋巴清扫对于黑素瘤早期患者有较好的疗效[3];对于黑素瘤晚期患者,多采用放射性治疗及化疗,但这两种方法对患者伤害较大而且疗效欠佳、不良反应大且患者易产生抗药性。因此,需要寻找安全高效的黑素瘤治疗方法。随着人们对黑素瘤发病机制研究的深入,特别是相关突变基因的鉴定及关键免疫调节检查点的发现,黑素瘤化疗药物治疗、靶向治疗、生物免疫治疗及多药物联合治疗手段得到不同程度的发展,本文就此作一综述。
1 化疗药物
1975年,达卡巴嗪(dacarbazine, DITC)得到美国食品与药物监督管理局(FDA)批准,成为第1个被用于黑素瘤临床治疗的化疗药物。此后,多种化疗药物先后出现,化疗也一度成为黑素瘤临床治疗的主要手段,但各种化疗药物的治疗效果参差不齐,相关药物见表1。其中,替莫唑胺(temozolomide,TMZ)因有较好的穿透血脑屏障的能力而对治疗脑转移的黑素瘤显示出更好的效果[4];亚硝基脲类药物可作用于处于不同增殖期的黑素瘤细胞。然而,化疗不良反应大、患者易产生抗药性的缺陷使单一化疗药物难以成为黑素瘤治疗的长远选择[5]。而以紫杉醇及长春花碱为代表的天然类药物及新发现的天然药物(如Honokiol、Forsythiae Fructus及P-Hydroxycinnamaldehyde)在良好地抑制黑素瘤的同时具有更低的毒性[6-8]。近年来,天然药物与纳米技术结合也取得了较大成效,纳米材料荷载的天然药物在具有更好的细胞吸收与靶向性的同时,具有更低的毒性。已有研究[9]证明,顺铂蛋白纳米颗粒对黑素瘤细胞B16有明显的抑制效果,提示纳米分子与铂类化合物共同作用可用于治疗黑素瘤。白蛋白结合型紫杉醇已显示出较好的疗效,且与紫杉醇单药相比有更低的致过敏性[10]。研究[11]表明,缺氧诱导因子-1α(HIF-1α)在肿瘤组织中的积累可促进黑素瘤的进展,导致患者生存率降低,而抗坏血酸(AA)和磷酸抗坏血酸-2(A2P)等可用以调节HIF-1α的积累和活性。此外,甲基砜可以抑制HIF-1α及血管内皮生长因子(VEGF)、促血管生成蛋白和转铁蛋白等促肿瘤转移的调节因子的表达[12]。

表1 黑素瘤化疗药物的作用机制及疗效
PFS(progression-free-survival):无进展生存期;ORR(objective response rate):客观缓解率;OS(overall survival):总生存期;OR(odd ratio):比值比;OSR(overall survival rate):总存活率;DCR(disease control rate):疾病控制率
2 生物治疗
黑素瘤为免疫原性较强的肿瘤,但因其具有“掩藏”抗原的特性,故常显示出免疫逃逸性质。因此,通过激发机体的免疫系统以减少瘤体微环境中调节性T淋巴细胞数量、增加细胞毒性T淋巴细胞数量进而增强局部抗肿瘤免疫力在较长一段时间内是黑素瘤治疗的研究热点。1991年,特异细胞毒性T细胞识别的人类黑素瘤抗原被成功分离。近些年,T细胞活化模式日益清晰,随着T细胞活化的“双信号模式”的阐明、树突状细胞(DC)免疫生物学的进展和人类白细胞抗原(HLA)基因测序的完成,黑素瘤的生物治疗得到进一步发展[19],其主要包括基因治疗、细胞因子治疗、过继免疫治疗以及疫苗治疗。
2.1 细胞因子治疗 自IL-2作为治疗晚期/转移性黑素瘤的非特异性免疫调节剂而得到FDA批准后,干扰素(INF)、贝伐单抗等因其对免疫系统的调节功能而多用于黑素瘤的免疫治疗以及生物化学治疗。其中,贝伐单抗更是常与免疫抑制剂及化疗药物联合使用,且取得较好效果。而白细胞介素-2(IL-2)与IL-12除单药使用外,在基因治疗中也疗效较好。研究[20]使用体内电穿孔方法(EP)将IL-2与IL-12基因导入转移性黑素瘤细胞内,在19例患者中,2例完全缓解。进一步将IFN-γ与IL-2、IL-12在小鼠体内联用,CD8+的CTL细胞溶解酶活性增强[21],这一结果为EP/IL-2、IL-12疗法的进一步发展提供了参考(表2)。
2.2 免疫检查点 细胞因子治疗可在短期内增强体内的免疫效应,常效果不明显且持续时间较短。随着免疫检查点的发现,特异性靶向免疫检查点的单克隆抗体抑制了肿瘤免疫逃逸效应,从而弥补了细胞因子治疗的缺点(表3)。免疫检查点参与T细胞的负调控,其在肿瘤患者的T细胞中表达相对升高,是造成肿瘤免疫逃逸现象的主要原因。目前已有两大类免疫检查点抑制剂被美国FDA批准应用于黑素瘤的临床治疗,分别为抗CTLA-4和抗PD-1/PD-L1的抗体。然而,肿瘤免疫检查点抑制剂易产生较大的不良反应,可在抑制肿瘤达到的同时杀伤正常细胞。
近年来新发现的免疫检查点除CTLA-4和PD-1/L1外,还包括T细胞免疫球蛋白结构域-3(TIM-3)、杀伤细胞抑制性受体(KIRs)、B7-H3等。目前以TIM-3的研究最为深入。其主要表达于辅助性T细胞(Th1)表面,与癌胚抗原相关细胞黏附分子1(CEACAM1)相互作用而诱发肿瘤免疫逃逸。在对转移性的结肠癌细胞的TIM-3进行敲除及对其功能进行抑制后,调节性T细胞(Treg)与T细胞受到的抑制明显减弱[27],故TIM-3或可成为黑素瘤免疫治疗的潜在靶点。
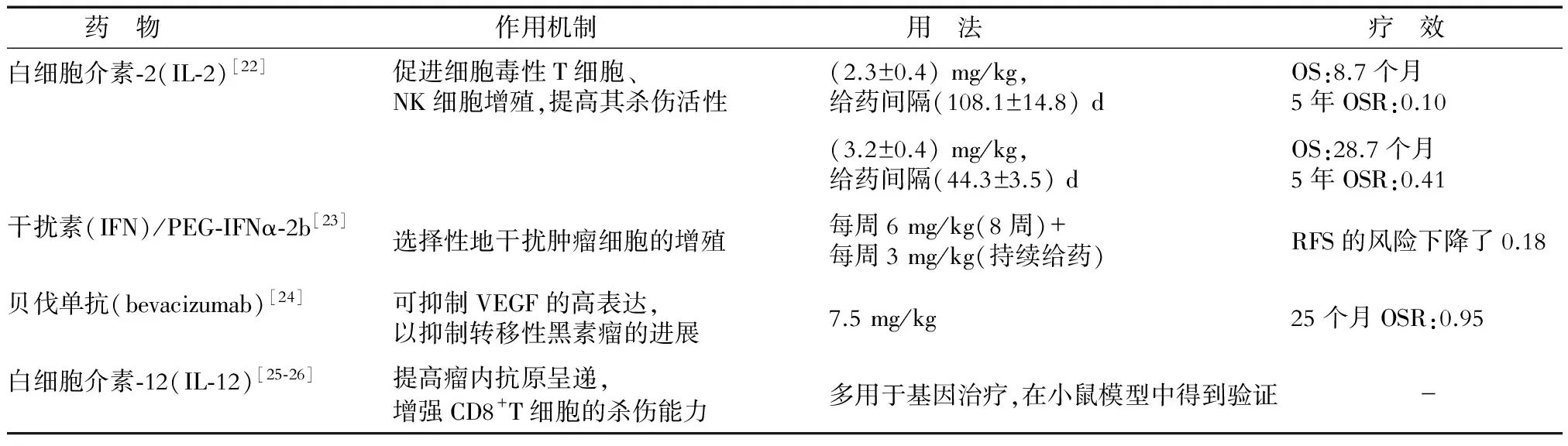
表2 黑素瘤细胞因子药物的作用机制和疗效
OS(overall survival):总生存期;OSR(overall survival rate):总存活率;RFS(recurrence-free survival):无复发生存期
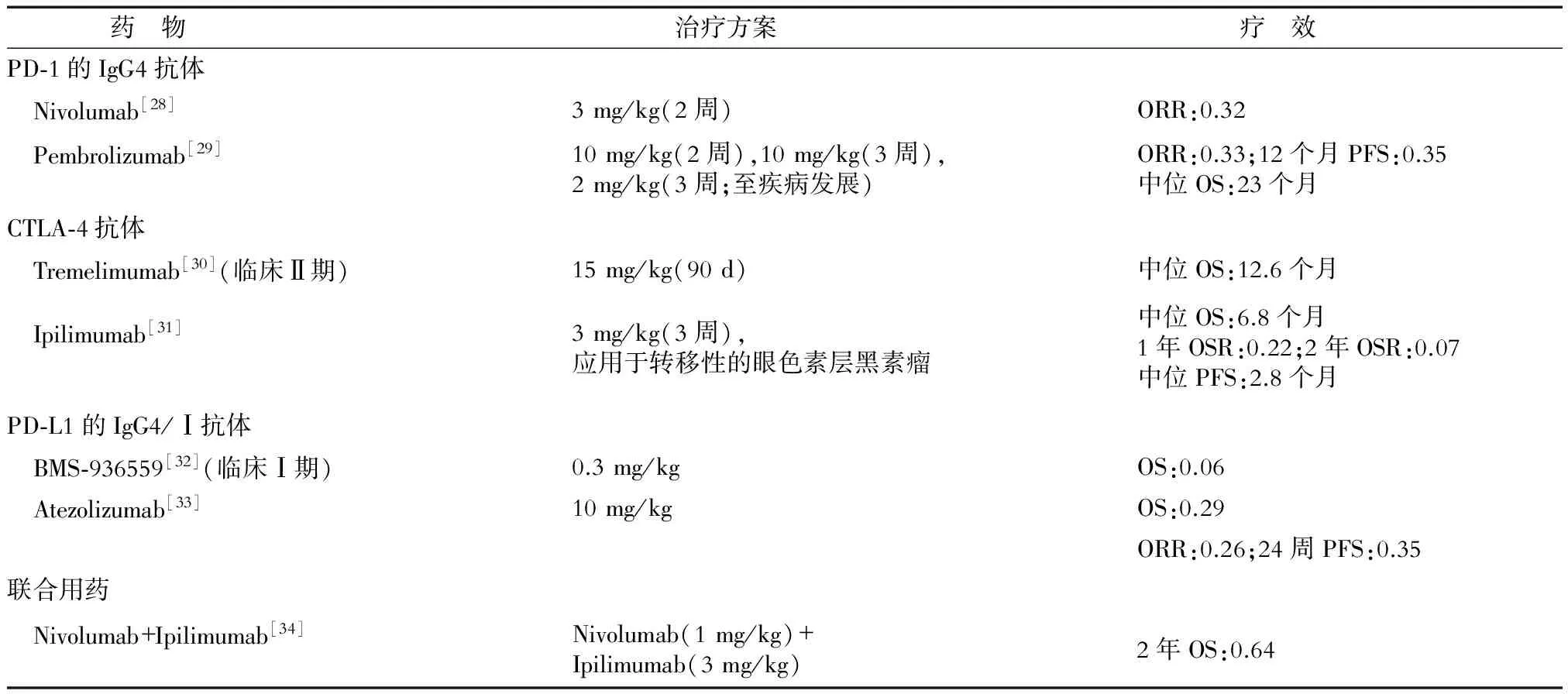
表3 免疫检查点抑制剂的作用机制及治疗效果
ORR(objective response rate):客观缓解率;OS(overall survival):总生存期;OSR(overall survival rate):总存活率;PFS(progression-free survival):无进展生存期
2.3 过继性免疫治疗(ACI) ACI中,肿瘤浸润淋巴细胞(tumor-infiltrating lymphocytes,TIL)与嵌合抗原受体淋巴细胞(chimeric antigen receptor lymphocyte, CAR-T)因具有比肿瘤疫苗更为直接的抗瘤效果,成为近年来肿瘤免疫治疗中的主力,在黑素瘤治疗中的应用也得到发展(表4)。TIL疗法已在临床试验中,而CAR-T疗法也先后在体外及小鼠体内证明了其有效性,曾被批准进行临床试验,但治疗效果因人、因病而异(表4)。虽然ACI在体表现出独特的肿瘤治疗效果,但易引起不良反应(患者常伴有持续发热),患者治疗后常反复发作,加之其在固体肿瘤中的疗效弱于对血液瘤的疗效,因此其在黑素瘤中的进一步应用受到阻碍。

表4 ACI的作用机制及治疗效果
ORR(objective response rate):客观缓解率
3 靶向治疗
黑素瘤的发展与细胞增殖、分化和细胞死亡的关键信号通路中分子的畸变有关。如表5所示,50%~60%的黑素瘤有RAS/RAF/MEK/ERK(MAPK)通路的改变,这使该途径成为主要治疗靶点。KIT的变异较不常见且主要发生在黏膜、肢端、皮肤以及MAPK抑制剂治疗后的抗药性黑素瘤中,约占黑素瘤总体突变种类的1%[40]。Buparlisib为PI3K-AKT通路的另一种抑制剂,最近有研究[41]表明,Buparlisib抑制PI3K-AKT通路在体内与体外均起到对黑素瘤脑转移的治疗效果,提示PI3K-AKT通路可作为黑素瘤脑转移的又一作用靶点。
细胞信号转导系统极其复杂,且黑素瘤中各种细胞处于不同的生长阶段。此外,转移起始细胞的存在使黑素瘤治疗后黑素瘤细胞仍会残留甚至转移。因此,针对某一单独途径的靶向治疗的前期效果明显,但治疗后常有黑素瘤的复发,且复发的黑素瘤多对该药物产生一定抗药性。因此,在黑素瘤治疗中,靶向药物的使用应当同时针对黑素瘤细胞的多个代谢途径,且应与其他种类药物联合使用,以达到更彻底的治疗效果。
此外,针对黑素瘤起始细胞的治疗近年来也逐步得到重视。已有研究[50]表明,人ATP-结合盒(ABC)转运蛋白在黑素瘤的多重耐药中起重要作用。相关蛋白ABCB5可被视为具有高致瘤能力的黑素瘤起始细胞的标志物[51],而解旋酶HAGE在ABCB5黑素瘤起始细胞介导的肿瘤发生中起关键作用[52],故HAGE可作为特异性靶点用于针对黑素瘤起始细胞的靶向治疗。

表5 靶向治疗的作用机制及治疗效果
PFS(progression-free survival):无进展生存期;OSR(overall survival rate):总存活率;OIRR(overall intracranial response rate ):颅内总体反应率;ORR(objective response rate):客观缓解率;DCR(disease control rate):疾病控制率;OS(overall survival):总生存期
4 多药联合治疗
多药联合治疗主要包括多种同类药物同时使用以及不同种类药物联合使用的治疗(表6)。将化疗药物和生物制剂联合应用以同时对黑素瘤中的多个代谢途径进行抑制,比单药治疗有更高的客观缓解率及更低的复发率。目前免疫检查点抑制剂与其他药物的联合使用仍未得到充分发展。

表6 多药物联合的治疗效果
RFS(recurrence-free survival):无复发生存期;OS(overall survival):总生存期;ORR(objective response rate):客观缓解率;PFS(progression-free survival):无进展生存期;OSR(overall survival rate):总存活率
5 国内黑素瘤治疗药物及研发
虽然黑素瘤在我国发病率较低,但是仍保持着较高的增长率,应引起临床工作者的重视。虽然近些年来我国在一些抗黑素瘤药物如淋巴毒素-α衍生物[59]、纳米氧化亚铜[60]、Aspartyl-chlorin p6 dimethylester(7b)[61]等的研发上取得了一定成效,但是我国对于黑素瘤的临床药物研究仍有所欠缺,尤其是抗黑素瘤药物针对中国人的效果以及不良反应的研究缺乏充足的数据支持[62](表7)。因此,针对中国人的黑素瘤药物的临床试验仍需进一步开展。

表7 部分药物在中国的临床应用效果
ORR(objective response rate):客观缓解率;DCR(disease control rate):疾病控制率;RFS(recurrence-free survival):无复发生存期
6 展 望
目前,随着人们对黑素瘤生物学特性认识的逐渐深入及新型生物材料的不断涌现,在黑素瘤的治疗方面,一些新型药物和疗法也展现出很好的发展前景。如纳米材料因其低毒性、高靶向性、高效性以及易溶解性而对黑素瘤有较好的疗效[60]。一些纳米材料如纳米氧化亚铜对黑素瘤治疗的效果较好[64]。但是,纳米材料在药物荷载能力及保存方面明显不足,加之缺乏完善的药物毒理评价体系,导致纳米类药物在临床的进一步应用受到阻碍[65]。而光敏剂在特定波长下产生的细胞毒性活性氧可引起肿瘤细胞的凋亡与坏死[66]。其中,卟吩姆钠(porfimer sodium)为经典的光敏剂,主要通过改变线粒体膜电位而诱导细胞凋亡,从而达到对黑素瘤的治疗效果[67];Aspartyl-chlorin p6 dimethylester (7b)为水溶性光敏剂,在小鼠体内取得良好的黑素瘤抑制效果且具有低毒性[61]。此外,由于黑素瘤恶性程度、表型以及病情发展在年龄分布上有一定差异[68],所以相关抗黑素瘤药物研发应当针对不同年龄的患者群体进行。
[ 1 ] SHAH D J, DRONCA R S. Latest advances in chemotherapeutic, targeted, and immune approaches in the treatment of metastatic melanoma[J]. Mayo Clin Proc, 2014,89(4):504-519.
[ 2 ] TRIPP M K, WATSON M, BALK S J, et al. State of the science on prevention and screening to reduce melanoma incidence and mortality: The time is now[J]. CA Cancer J Clin, 2016.
[ 3 ] 向 阳,朱 凯.腹股沟淋巴结清扫范围对下肢恶性黑色素瘤患者预后的影响[J].中国临床医学, 2009,16(4):634-635.
[ 4 ] MIDDLETON M R, GROB J J, AARONSON N, et al. Randomized phase Ⅲ study of temozolomide versus dacarbazine in the treatment of patients with advanced metastatic malignant melanoma[J]. J Clin Oncol, 2000, 18(1):158-166.
[ 5 ] KALIKI S, SHIELDS C L. Uveal melanoma: relatively rare but deadly cancer[J]. Eye (Lond), 2017,31(2):241-257.
[ 6 ] GUILLERMO-LAGAE R, SANTHA S, THOMAS M, et al. Antineoplastic effects of honokiol on melanoma[J]. Biomed Res Int, 2017,2017:5496398.
[ 7 ] ZHAO L M, SUN G G, HAN L N, et al. P-Hydroxycinnamaldehyde induces B16-F1 melanoma cell differentiationviathe RhoA-MAPK signaling pathway[J]. Cell Physiol Biochem, 2016,38(6):2247-2260.
[ 8 ] BAO J, DING R, ZOU L, et al. Forsythiae fructus inhibits B16 melanoma growth involving MAPKs/Nrf2/HO-1 mediated anti-oxidation and anti-inflammation[J]. Am J Chin Med, 2016, 44(5):1043-1061.
[ 9 ] SHRIKHANDE S S, JAIN D S, ATHAWALE R B, et al. Evaluation of anti-metastatic potential of cisplatin polymeric nanocarriers on B16F10 melanoma cells[J]. Saudi Pharm J, 2015,23(4):341-351.
[10] KOTTSCHADE L A, SUMAN V J, AMATRUDA T 3rd, et al. A phase Ⅱ trial of nab-paclitaxel (ABI-007) and carboplatin in patients with unresectable stage Ⅳ melanoma : a North Central Cancer Treatment Group Study, N057E(1)[J]. Cancer, 2011,117(8):1704-1710.
[11] FISCHER A P, MILES S L. Ascorbic acid, but not dehydroascorbic acid increases intracellular vitamin C content to decrease hypoxia inducible factor -1 alpha activity and reduce malignant potential in human melanoma[J]. Biomed Pharmacother, 2017,86:502-513.
[12] CARON J M, CARON J M. Methyl sulfone blocked multiple hypoxia- and non-hypoxia-induced metastatic targets in breast cancer cells and melanoma cells[J]. PLoS One, 2015,10(11):e0141565.
[13] ZHU W, ZHOU L, QIAN J Q, et al. Temozolomide for treatment of brain metastases: a review of 21 clinical trials[J]. World J Clin Oncol, 2014,5(1):19-27.
[14] AVRIL M F, AAMDAL S, GROB J J, et al. Fotemustine compared with dacarbazine in patients with disseminated malignant melanoma: a phase Ⅲ study[J]. J Clin Oncol, 2004, 22(6):1118-1125.
[15] EVANS L M, CASPER E S, ROSENBLUTH R. PhaseⅡ trial of carboplatin in advanced malignant melanoma[J]. Cancer Treat Rep, 1987,71(2):171-172.
[16] GLOVER D, GLICK J H, WEILER C, et al. WR-2721 and high-dose cisplatin: an active combination in the treatment of metastatic melanoma[J]. J Clin Oncol, 1987,5(4):574-578.
[17] RAO R D, HOLTAN S G, INGLE J N, et al. Combination of paclitaxel and carboplatin as second-line therapy for patients with metastatic melanoma[J]. Cancer, 2006,106(2):375-382.
[18] HERSH E M, DEL VECCHIO M, BROWN M P, et al. A randomized, controlled phase Ⅲ trial of nab-paclitaxel versus dacarbazine in chemotherapy-naïve patients with metastatic melanoma[J]. Ann Oncol, 2015,26(11):2267-2274.
[19] 汪文君, 刘向辉. 恶性黑色素瘤的生物治疗研究进展[J]. 口腔医学, 2014,34(3):225-227.
[20] DAUD A I, DECONTI R C, ANDREWS S, et al. PhaseⅠtrial of interleukin-12 plasmid electroporation in patients with metastatic melanoma[J]. J Clin Oncol, 2008,26(36):5896-5903.
[21] SIN J I, PARK J B, LEE I H, et al. Intratumoral electroporation of IL-12 cDNA eradicates established melanomas by Trp2(180-188)-specific CD8+CTLs in a perforin/granzyme-mediated and IFN-γ-dependent manner: application of Trp2(180-188) peptides[J]. Cancer Immunol Immunother, 2012,61(10):1671-1682.
[22] GREENE J M, SCHNEBLE E J, JACKSON D O, et al. A phase Ⅰ/Ⅱa clinical trial in stage Ⅳ melanoma of an autologous tumor-dendritic cell fusion (dendritoma) vaccine with low dose interleukin-2[J]. Cancer Immunol Immunother, 2016,65(4):383-392.
[23] BOTTOMLEY A, COENS C, SUCIU S, et al. Adjuvant therapy with pegylated interferon alfa-2b versus observation in resected stage Ⅲ melanoma: a phase Ⅲ randomized controlled trial of health-related quality of life and symptoms by the European Organisation for Research and Treatment of Cancer Melanoma Group[J]. J Clin Oncol, 2009,27(18):2916-2923.
[24] CORRIE P G, MARSHALL A, DUNN J A, et al. Adjuvant bevacizumab in patients with melanoma at high risk of recurrence (AVAST-M): preplanned interim results from a multicentre, open-label, randomised controlled phase 3 study[J]. Lancet Oncol, 2014,15(6):620-630.
[25] GALVAN D L, O’NEIL R T, FOSTER A E, et al. Anti-tumor effects after adoptive transfer of IL-12 transposon-modified murine splenocytes in the OT-I-melanoma mouse model[J]. PLoS One, 2015,10(10):e0140744.
[26] ANDRIJAUSKAITE K, SURIANO S, CLOUD C A, et al. IL-12 conditioning improves retrovirally mediated transduction efficiency of CD8+T cells[J]. Cancer Gene Ther, 2015,22(7):360-367.
[27] HUANG Y H, ZHU C, KONDO Y, et al. CEACAM1 regulates TIM-3-mediated tolerance and exhaustion[J]. Nature, 2015,517(7534):386-390.
[28] U.S. Food and Drug Administration. Opdivo (nivolumab) prescribing information[R].U.S. Food and Drug Administration, 2016.
[29] RIBAS A, HAMID O, DAUD A, et al. Association of pembrolizumab with tumor response and survival among patients with advanced melanoma[J]. JAMA, 2016,315(15):1600-1609.
[30] RIBAS A, KEFFORD R, MARSHALL M A, et al. Phase Ⅲrandomized clinical trial comparing tremelimumab with standard-of-care chemotherapy in patients with advanced melanoma[J]. J Clin Oncol, 2013,31(5):616-622.
[31] ZIMMER L, VAUBEL J, MOHR P, et al. PhaseⅡDeCOG-study of ipilimumab in pretreated and treatment-naïve patients with metastatic uveal melanoma[J]. PLoS One, 2015,10(3):e0118564.
[32] BRAHMER J R, TYKODI S S, CHOW L Q, et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer[J]. N Engl J Med, 2012,366(26):2455-2465.
[33] HAMID O, SOSMAN J A, LAWRENCE D P, et al. Clinical activity, safety, and biomarkers of MPDL3280A, an engineered PD-L1 antibody in patients with locally advanced or metastatic melanoma (mM)[J]. J Clin Oncol, 2013,31(15).
[34] HODI F S, CHESNEY J, PAVLICK A C, et al. Combined nivolumab and ipilimumab versus ipilimumab alone in patients with advanced melanoma: 2-year overall survival outcomes in a multicentre, randomised, controlled, phase 2 trial[J]. Lancet Oncol, 2016,17(11):1558-1568.
[35] ZIKICH D, SCHACHTER J, BESSER M J. Predictors of tumor-infiltrating lymphocyte efficacy in melanoma[J]. Immunotherapy, 2016,8(1):35-43.
[36] KHAMMARI A, KNOL A C, NGUYEN J M, et al. Adoptive TIL transfer in the adjuvant setting for melanoma: long-term patient survival[J]. J Immunol Res, 2014,2014:186212.
[37] YVON E, DEL VECCHIO M, SAVOLDO B, et al. Immunotherapy of metastatic melanoma using genetically engineered GD2-specific T cells[J]. Clin Cancer Res, 2009,15(18):5852-5860.
[38] GARGETT T, YU W, DOTTI G, et al. GD2-specific CAR T cells undergo potent activation and deletion following antigen encounter but can be protected from activation-induced cell death by PD-1 blockade[J]. Mol Ther, 2016,24(6):1135-1149.
[39] GELDRES C, SAVOLDO B, HOYOS V, et al. T lymphocytes redirected against the chondroitin sulfate proteoglycan-4 control the growth of multiple solid tumors bothinvitroandinvivo[J]. Clin Cancer Res, 2014,20(4):962-971.
[40] SHTIVELMAN E, DAVIES M Q, HWU P, et al. Pathways and therapeutic targets in melanoma[J]. Oncotarget, 2014,5(7):1701-1752.
[41] NIESSNER H, SCHMITZ J, TABATABAI G, et al. PI3K pathway inhibition achieves potent antitumor activity in melanoma brain metastasesinvitroandinvivo[J]. Clin Cancer Res, 2016,22(23):5818-5828.
[42] CHAPMAN P B, HAUSCHILD A, ROBERT C, et al. Improved survival with vemurafenib in melanoma with BRAF V600E mutation[J]. N Engl J Med, 2011,364(26):2507-2516.
[43] HAUSCHILD A, GROB J J, DEMIDOV L V, et al. Dabrafenib in BRAF-mutated metastatic melanoma: a multicentre, open-label, phase 3 randomised controlled trial[J]. Lancet, 2012,380(9839):358-365.
[44] LONG G V, TREFZER U, DAVIES M A, et al. Dabrafenib in patients with Val600Glu or Val600Lys BRAF-mutant melanoma metastatic to the brain (BREAK-MB): a multicentre, open-label, phase 2 trial[J]. Lancet Oncol, 2012,13(11):1087-1095.
[45] FLAHERTY K T, ROBERT C, HERSEY P, et al. Improved survival with MEK inhibition in BRAF-mutated melanoma[J]. N Engl J Med, 2012,367(2):107-114.
[46] LONG G V, STROYAKOVSKIY D, GOGAS H, et al. Combined BRAF and MEK inhibition versus BRAF inhibition alone in melanoma[J]. N Engl J Med, 2014,371(20):1877-1888.
[47] LEE S J, KIM T M, KIM Y J, et al. PhaseⅡtrial of nilotinib in patients with metastatic malignant melanoma harboring KIT gene aberration: a multicenter trial of Korean Cancer Study Group (UN10-06)[J]. Oncologist, 2015,20(11):1312-1319.
[48] SLINGLUFF C L JR, PETRONI G R, MOLHOEK K R, et al. Clinical activity and safety of combination therapy with temsirolimus and bevacizumab for advanced melanoma: a phaseⅡtrial (CTEP 7190/Mel47)[J]. Clin Cancer Res, 2013,19(13):3611-3620.
[49] DRONCA R S, ALLRED J B, PEREZ D G, et al. PhaseⅡstudy of temozolomide (TMZ) and everolimus (RAD001) therapy for metastatic melanoma: a North Central Cancer Treatment Group study, N0675[J]. Am J ClinOncol, 2014,37(4):369-376.
[50] 徐文博, 张江安, 于建斌,等. ABC转运蛋白ABCG2在皮肤黑素瘤中的表达[J]. 中国皮肤性病学杂志, 2010,24(5):395-397.
[51] SCHATTON T, MURPHY G F, FRANK N Y, et al. Identification of cells initiating human melanomas[J]. Nature, 2008,451(7176):345-349.
[52] LINLEY A J, MATHIEU M G, MILES A K, et al. The helicase HAGE expressed by malignant melanoma-initiating cells is required for tumor cell proliferationinvivo[J]. J Biol Chem, 2012,287(17):13633-13643.
[53] FLAHERTY L E, OTHUS M, ATKINS M B, et al. Southwest Oncology Group S0008: a phase Ⅲ trial of high-dose interferon alfa-2b versus cisplatin, vinblastine, and dacarbazine, plus interleukin-2 and interferon in patients with high-risk melanoma--an intergroup study of cancer and leukemia Group B, Children’s Oncology Group, Eastern Cooperative Oncology Group, and Southwest Oncology Group[J]. J ClinOncol, 2014,32(33):3771-3778.
[54] ALRWAS A, PAPADOPOULOS N E, CAIN S, et al. PhaseⅠtrial of biochemotherapy with cisplatin, temozolomide, and dose escalation of nab-paclitaxel combined with interleukin-2 and interferon-α in patients with metastatic melanoma[J]. Melanoma Res, 2014,24(4):342-348.
[55] PAPADOPOULOS N E, BEDIKIAN A, RING S, et al. Phase Ⅰ/Ⅱ study of a cisplatin-taxol-dacarbazine regimen in metastatic melanoma[J]. Am J ClinOncol, 2009,32(5):509-514.
[56] FERRUCCI P F, MINCHELLA I, MOSCONI M, et al. Dacarbazine in combination with bevacizumab for the treatment of unresectable/metastatic melanoma: a phaseⅡstudy[J]. Melanoma Res, 2015,25(3):239-245.
[57] FLAHERTY K T, HAMILTON B K, ROSEN M A, et al. PhaseⅠ/Ⅱtrial of imatinib and bevacizumab in patients with advanced melanoma and other advanced cancers[J]. Oncologist, 2015,20(8):952-959.
[58] SPITLER L E, BOASBERG P, O’DAY S, et al. PhaseⅡstudy of nab-paclitaxel and bevacizumab as first-line therapy for patients with unresectable stage Ⅲ and Ⅳmelanoma[J]. Am J ClinOncol, 2015,38(1):61-67.
[59] WANG F H, LI Y H, LI S, et.al. Phase I clinical trial of intravenous recombinant human lymphotoxin-alpha derivative[J]. Ai Zheng, 2006,25(4):501-504.
[60] 于 斌, 连海燕, 王 野, 等. 纳米材料应用于肿瘤治疗的研究进展[J]. 中国细胞生物学学报, 2015,(4):594-598.
[61] MENG Z, ZHANG B, LIU B, et al. High carotenoids content can enhance resistance of selected Pinctadafucata families to high temperature stress[J]. Fish Shellfish Immunol, 2017,61:211-218.
[62] GUO Y Q, DING Y, LI D D, et.al. Efficacy and safety of nab-paclitaxel combined with carboplatin in Chinese patients with melanoma[J]. Med Oncol, 2015,32(9):234.
[63] MAO L, SI L, CHI Z, et.al. A randomised phaseⅡtrial of 1 monthversus1 year of adjuvant high-dose interferon α-2b in high-risk acral melanoma patients[J]. Eur J Cancer, 2011,47(10):1498-1503.
[64] WANG Y, YANG F, ZHANG H X, et al. Cuprous oxide nanoparticles inhibit the growth and metastasis of melanoma by targeting mitochondria[J]. Cell Death Dis, 2013,4:e783.
[65] RIGON R B, OYAFUSO M H, FUJIMURA A T, et al. Nanotechnology-Based Drug Delivery Systems for melanoma antitumoral therapy: a review[J]. Biomed Res Int, 2015,2015:841817.
[66] ROGERS L, SERGEEVA N N, PASZKO E, et al. Lead structures for applications in photodynamic therapy. 6. temoporfin anti-inflammatory conjugates to target the tumor microenvironment forinvitroPDT[J]. PLoS One, 2015,10(5):e0125372.
[67] CHOROMAN'SKA A, SACZKO J, KULBACKA J, et al. The potential role of photodynamic therapy in the treatment of malignant melanoma--an in vitro study[J]. Adv Clin Exp Med, 2012,21(2):179-185.
[68] 马阳阳, 许建芳, 陈 莲, 等.儿童黑色素瘤的病理分析:附4例报告[J].中国临床医学,2014,21(2):192-195.
Clinical treatment of human melanoma: recent progress
FU Jing-bo1, YU Bin2, ZHANG Hong-xia1, ZHU Hai-ying1*
1. Department of Cell Biology, College of Basic Medicine Sciences, Navy Military Medical University, Shanghai 200433, China 2. Department of Life Science, Fudan University, Shanghai 200433, China
The mortality rate of melanoma is high. Chemotherapy became the main treatment during the past years besides traditional surgical excision and radiotherapy.In recent years, with the in-depth study of the molecular mechanism of the occurrence and development of melanoma, new treatment methods and medicines basing on the target therapy and immune therapy have emerged constantly. At present, in addition to the drugs that have been used in clinical treatment, some of the drugs that are being approved for clinical research and the potential drugs which are still in basic research show good application prospects. In this paper, the molecular mechanism and therapeutic effect of the representative drugs or potential drugs in the treatment of melanoma were reviewed.
melanoma; multi-drug combination therapy; biological immunotherapy; targeted therapy
2017-03-17接受日期2017-06-08
国家自然科学基金(31471284). Supported by National Natural Science Foundation of China(31471284).
付靖波,海军军医大学2015级临床医学专业本科学员. E-mail: fujingboi@163.com
*通信作者(Corresponding author). Tel: 021-81870944(0), E-mail: zinnia69@163.com
10.12025/j.issn.1008-6358.2017.20170223
R 739.5
A
[本文编辑] 廖晓瑜, 贾泽军
