激光针治疗乳腺癌相关淋巴水肿的临床研究
2017-08-26金明子周愉曹红平张海蒙
金明子++周愉+曹红平++张海蒙
[摘要] 目的 观察He-Ne激光针治疗乳腺癌相关淋巴水肿(BCRL)的临床效果及安全性。 方法 选择2014年11月~2016年3月上海复旦大学附属华山医院分院收治的BCRL患者32例,按随机数字表分为治疗组和对照组,每组各16例,治疗组在对照组常规治疗基础上,选取10个穴位,进行He-Ne激光针治疗,每次同时照射2个穴位,每个穴位照射5 min,单次治疗时间共25 min,每周治疗2次,连续治疗6周,共治疗12次。比较两组治疗前后、治疗结束后4周随访时,患肢臂围变化及患肢水肿改善率,观察患者不良反应情况。 结果 ①治疗组治疗后与治疗前比较,患肢臂围显著减小(症状减轻),差异有统计学意义(P < 0.05),治疗结束后4周随访时与治疗前比较,患肢臂围持续减小,差异有统计学意义(P < 0.05)。对照组入组6、10周后与入组前比较,患肢臂围有增大的趋势(症状加重),但差异无统计学意义(P > 0.05)。②治疗6周,治疗组患肢水肿改善率显著高于对照组,差异有统计学意义(P < 0.05);治疗结束后4周随访,治疗组患肢水肿改善率显著高于对照组,差异有统计学意义(P < 0.05)。③在治疗及随访期间无不良反应报告。 结论 He-Ne激光针可以有效改善BCRL患者的水肿程度,并具有良好的安全性。
[關键词] 乳腺癌;淋巴水肿;激光针;临床疗效
[中图分类号] R737.9 [文献标识码] A [文章编号] 1673-7210(2017)07(b)-0101-04
Clinical effects of laser acupuncture treatment on breast cancer-related lymphoedema
JIN Mingzi1 ZHOU Yu1 CAO Hongping2 ZHANG Haimeng2
1.International Education College, Shanghai University of Traditional Chinese Medicine, Shanghai 201203, China; 2.College of Acupuncture and Moxibustion, Shanghai University of Traditional Chinese Medicine, Shanghai 201203, China
[Abstract] Objective To observe the clinical effects and safety of laser acupuncture treatment on breast cancer-related lymphoedema (BCRL). Methods From November 2014 to March 2016, in Branch Courts of Huashan Hospital of Shanghai Fudan University, 32 BCRL patients were selected, according to random number table, they were divided into treatment group and control group, with 16 cases in each group. On the basis of conventional treatment (control group), the treatment group was given He-Ne laser acupuncture treatment on 10 selected acupuncture points. The 10 points were paired off and radiated for 25 min in a single treatment, 5 min per pair. The whole therapy lasted for six weeks, twice a week, adding up to a total of 12 times. The patients' affected arms were measured before treatment and after treatment, and also at 4th week follow-up after treatment finished. Data of two groups were compared and arm edema changes were recorded. Adverse reactions were observed all along. Results ①In treatment group, the patients' affected arm circumference before treatment was compared with after 6 weeks of treatment, their arm circumference decreased (symptoms relieved), the difference was statistically significant (P < 0.05), 4 weeks after the treatment ended, their arm circumference had kept decreasing, the differences were statistically significant (P < 0.05). In control group, the figures at baseline and 6th, 10th week after they joined were compared with before they joined, their arm circumference increasing tendency (symptoms aggravated), but the difference was not statistically significant (P > 0.05). ②After 6 weeks of treatment, the improvement rate in treatment group was more than control group, the difference was statistically significant (P < 0.05); 4 weeks after the treatment ended, the follow-up examination, the improvement rate in treatment group was more than control group, the difference was statistically significant (P < 0.05). ③ No adverse reaction reported during treatment and follow-up visits. Conclusion He-Ne laser acupuncture treatment is safe and reliable. And it has significant curative effect on BCRL.
[Key words] Breast cancer; Lymphoedema; Laser acupuncture; Clinical effects
乳腺癌相关淋巴水肿(BCRL)是乳腺癌患者手术及放疗后继发的慢性疾病,表现为上肢部持续性水肿、易受感染和上肢功能障碍等,严重影响乳腺癌患者的生活质量[1]。乳腺癌患者BCRL发生率3年内为15%~54%,5年内为42%,且发病风险终身存在[2-3]。
目前采用的治疗手段是以减轻水肿为主的综合物理疗法(如加压包扎)或口服利水消肿药物,并无彻底的根治方法[4-6]。近年来,传统针灸治疗BCRL有一定的疗效[7-9],但因针灸破皮治疗有引发感染的可能性,临床使用上受到一定限制。激光针灸是将低强度激光束照射在穴位上产生针刺作用的治疗方法,因其无痛和无创的特性,使其在国外被当做传统针灸的替代疗法而广泛运用[10-12]。而运用激光针治疗BCRL是一个全新领域,相较于传统针灸既可避免刺破皮肤造成感染的可能性,又能发挥低能量激光增加淋巴和免疫系统活力和激发细胞组织内生长因子的优势[13-16],若其治疗BCRL的临床效果能得到验证将会为其在临床治疗上的推广提供可靠的依据。本临床试验采用随机、对照设计方法观察632.8 nm He-Ne激光针对BCRL患者的临床疗效,现报道如下:
1 资料与方法
1.1 一般资料
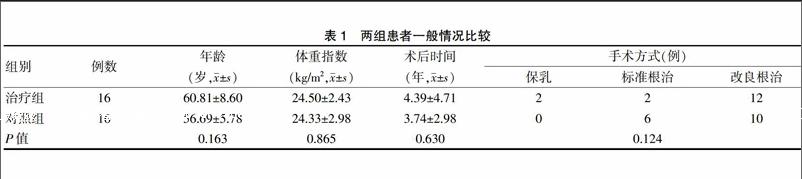
2014年11月~2016年3月,在上海复旦大学附属华山医院的乳腺癌专科门诊招募志愿者。临床试验方案经过医院的伦理委员会批准。告知参与的患者必须先签署书面的知情同意书后参加筛选和分组。患者均为女性,均为BCRL患者。共收治符合纳入标准的患者32例,根据随机数字分为两组。其中治疗组16例,完成治疗16例;对照组16例,第3周脱落3例,第6周脱落1例,脱落皆为个人原因无法继续参与试验。实际完成对照试验12例,其中除1例因个人原因只参加了1次补偿性治疗外,其余11例均完成了后期与治疗组相同的补偿性治疗。纳入标准:①单侧乳腺癌女性患者,18~75周岁,乳腺癌分期为Ⅰ、Ⅱ、Ⅲ期,诊断参照2003年WHO乳腺肿瘤的分类标准[17];②接受乳腺癌腋窝淋巴结扫除根治术;③上肢水肿分级为轻到中度:患侧上肢的平均周径比健侧粗8 cm以下,发生于上臂近端或影响至整个上肢部,包括前臂及手背。正式试验开始前,两组患者在年龄、体重指数、术后时间、手术方式等一般资料比较,差异无统计学意义(P > 0.05),具有可比性。见表1。
1.2 治疗方法
整个试验期间两组患者都维持原有常规治疗,如口服迈之灵(降低血管通透性,增加静脉回流功能)、手法按摩、抬高患肢等。
治疗组在常规治疗基础上,进行激光针治疗。仪器采用上海市激光技术研究所研制的LJL40-HA型He-Ne激光治疗仪,He-Ne激光波长为632.8 nm,最大激光输出功率为(40±5)mW。具体操作方法为激光输出端垂直照射在患者的极泉、肩髃、尺泽、曲泽、合谷、液门、气海、水分、阴陵泉、足三里等10个穴位(定位方法参考最新的腧穴名称与定位[18])上,但不与皮肤接触。每次同时照射2个穴位,每个穴位照射5 min,单次治疗时间共25 min,每周治疗2次,连续治疗6周,共治疗12次。治疗结束4周后,即第10周进行随访。对照组入组10周后开始接受与治疗组相同的补偿性治疗。
1.3 观察指标
1.3.1 安全性评估 每次治疗时都会询问患者是否有水肿部位意外伤害、红肿、起泡、肤色改变及腹泻、发热等全身性的不良反应发生,以跟踪激光治疗的安全性。
1.3.2 疗效评估 患者取仰卧位,手臂放松,置于身体的两侧,手肘伸直。使用卷尺分别测量患者上臂平腋窝处、尺骨鹰嘴上10 cm、尺骨鹰嘴下10 cm、腕关节和手掌中点,五个部位的双侧上肢周径值。将5个点的周径值相加得出总体周径值(臂围)。治疗前后患肢臂围变化及治疗后两组患肢水肿改善率为主要观察指标。患肢水肿改善率=(治疗前患肢臂围-治疗后患肢臂围)/(治疗前患肢臂围-治疗前健肢臂围)×100%
1.4 统计学方法
采用统计软件SPSS 19.0对数据进行分析,正态分布的计量资料以均数±标准差(x±s)表示,两组间比较采用t检验;计数资料以率表示,采用χ2检验。以P < 0.05为差异有统计学意义。
2 结果
2.1 两组患者不同时期患肢臂围变化比较
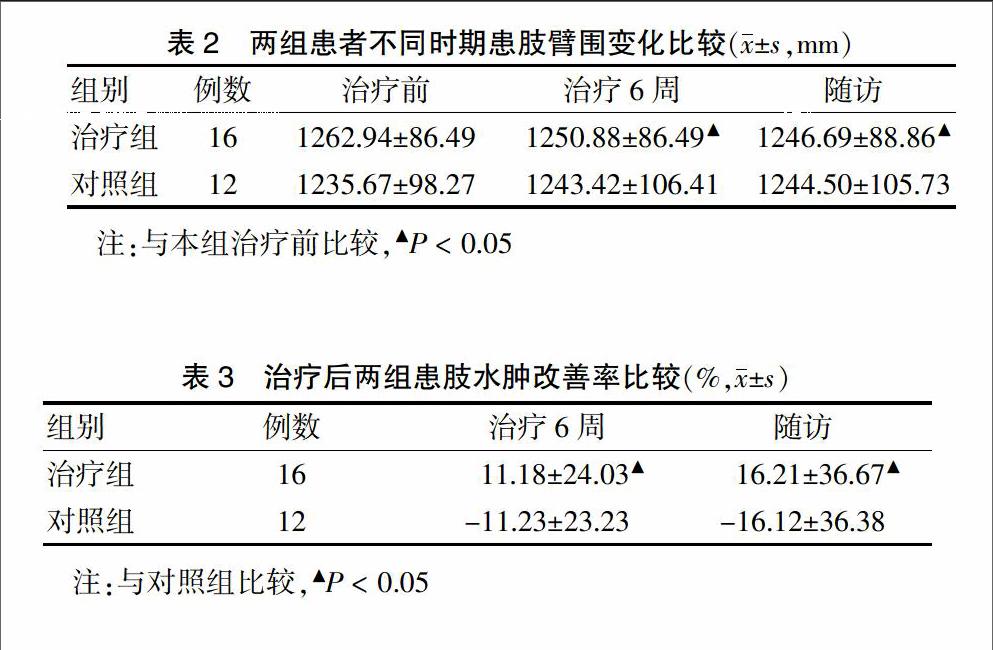
治疗组治疗后与治疗前比较,患肢臂围显著减小(症状减轻),差异有统计学意义(P < 0.05),治疗结束后4周随访时与治疗前比较,患肢臂围持续减小,差异有统计学意义(P < 0.05)。对照组入组6周后、入组10周后与入组前比较,患肢臂围有增大的趋势(症状加重),但差异无统计学意义(P > 0.05)。見表2。
2.2 治疗后两组患肢水肿改善率比较
治疗6周,治疗组患肢水肿改善率显著高于对照组,差异有统计学意义(P < 0.05);治疗结束后4周随访,治疗组患肢水肿改善率显著高于对照组,差异有统计学意义(P < 0.05)。见表3。
2.3 不良反应
在治疗及随访期间,无水肿部位意外伤害、红肿、起泡、肤色改变及腹泻、发热等全身性的不良反应报告。
3 讨论
乳腺癌,又名“乳岩”“奶岩”“石奶”[19],而BRCL在中医古籍中没有相关记载,相关论述散在于“水肿”“痹症”“瘀证”等多种病证范畴内。针灸治疗BCRL,尽管日本及美国的近期研究表明,严格遵守无菌操作,对患肢进行针刺治疗既不会引发感染又没有任何副作用[20-22],且有疗效。但针刺破皮引发感染的可能性仍不能被排除,故对其安全性和有效性的研究仍只能停留在小规模的临床试验。因此若有一种治疗手段既能发挥针刺治疗的优势,又能避免刺破皮肤而继发感染的可能性,将会是一种理想的选择。
1966 年匈牙利的Mester等[23-24]提出低強度激光具有生物刺激作用,此后,低强度激光被应用于临床治疗。目前临床应用的激光针灸大多采用波长为0.6~1.3 μm的红光和近红外光[25],此波段激光对皮肤的透过率较好,可达生物组织10~25 mm处形成“光针”效应,本试验采用激光针波长也在此范围内。
激光针治疗BCRL能发挥激光和针灸两种治疗手段的优势:首先,激光能通过影响线粒体提高ATP的生产和合成、优化氧合作用和巨噬细胞。生理上,激光产生的生物刺激会增加结缔组织、肌腱和软骨组织的细胞产生,从而增加胶原蛋白的生产。激光治疗能同时增加愈合组织的拉伸强度、减少水肿、增加血流量和淋巴活性、减少炎症、增加细胞代谢和加速修复过程[26]。其次,中医理论认为术中创伤,损伤脉络,血瘀气滞,为肿为痛,术后放化疗损血耗气,局部气血瘀滞逐渐加重,故治疗上除在局部淋巴结积聚的部位取穴外,还配合远道取穴,选足三里补气养血,阴陵泉利水消肿,气海温阳,水分通调水道,诸穴合用强化脏腑气化功能,达到益气利水消肿,活血化瘀止痛的目的。
本研究结果显示激光针具有良好的安全性,同时,治疗组经治疗患肢臂围显著减小(症状减轻),治疗结束后4周随访时,患肢臂围持续减小,差异有统计学意义(P < 0.05),而对照组患肢臂有增大的趋势(症状加重),但差异无统计学意义(P > 0.05),此结果与BCRL疾病本身是一种不能根治的、易复发、终生的慢性疾病,其发病机制中存在持续性、进行性加重的恶性循环,具有随着时间的推移,发病率亦会不断上升的特性相符。治疗组经治疗患肢水肿改善率显著高于对照组,差异有统计学意义(P < 0.05);治疗结束后4周随访时,患肢水肿改善率显著高于对照组,差异有统计学意义(P < 0.05),说明He-Ne激光针对BCRL有明显治疗效应,且其治疗效应可维持至治疗结束后4周随访时,有较高临床应用价值。无创伤和更安全是传统针灸的改革方向,特别对于BCRL等易感染的疾病的治疗,激光针的优势显而易见。课题组下一步的研究目标是进一步扩大样本量,更大范围上去论证激光针治疗BCRL的安全性与有效性。
[参考文献]
[1] Hayes SC,Janda M,Cornish B,et al. Lymphedema after breast cancel:incidence,risk factors,and effect on upper body function [J]. J Clin Oncol,2008,26(21):3536-3542.
[2] Norman SA,Localio AR,Potashnik SL,et al. Lymphedema in breast cancer survivors:incidence,degree,time course,treatment,and symptoms [J]. J Clin Oncol,2009,27(3):390-397.
[3] Fu MR,Ridner SH,Armer J. Post breast cancer Lymphedema:part1 [J]. Am J Nurs,2009,109(7):48-54.
[4] Gurdal SO,Kostanoglu A,Cavdar I,et al. Comparison of intermittent pneumatic compression with manual lymphatic drainage for treatment of breast cancer-related lymphedema [J]. Lymphat Res Biol,2012,10(3):129-135.
[5] Schaverien MV,Munro KJ,Baker PA,et al. Liposuction for chronic lymphoedema of the upper limb:5 years of experience [J]. J Plast Reconstr Aesthet Surg,2012,65(7):935-942.
[6] Oremus M,Dayes I,Walker K,et al. Systematic review:conservative treatments for secondary lymphedema [J]. BMC Cancer,2012,12:6.
[7] Kanakura Y,Niwa K,Kometani K,et al. Effectiveness of acupuncture and moxibustion treatment for lymphedema following intrapelvic lymph node dissection:a preliminary report [J]. Am J Chin Med,2002,30(1):37-43.
[8] Matecki A,Mercado-Poe C,Chen J,et al. Safety of acupuncture in the setting of extreme lymphedema——a retrospective study [C]//Soceity of Integrative Oncology Conference,Atlanta,GA,November 20-21,2008.
[9] Cassileth BR,Van Zee KJ,Chan Y,et al. A safety and efficacy pilot study of acupuncture for the treatment of chronic lymphoedema [J]. Acupunct Med,2011,29(3):170-172.
[10] Cohen M. Exploring the other side of acupuncture [J]. J Altern Complement Med,2006,12(8):707-708.
[11] Litscher G,Wang L,Wiesner-Zechmeister M. Specific effects of laser puncture on the cerebral circulation [J]. Lasers Med Sci,2000,15(1):57-62.
[12] Litscher G. High-tech laser acupuncture is Chinese medicine [J]. Acupunct Med,2008,20(4):245-254.
[13] Piller N,Thelander A. Treating chronic post mastectomy lymphoedema with low level laser therapy:a cost effective strategy to reduce lymphoedema severity and improve the quality of patient life [J]. Lymphology,1998,31(6):74-86.
[14] Moseley AL,Carati CJ,Piller NB. A systematic review of comon conservative therapies for arm lymphoedema secondary to breast cancer treatment [J]. Ann Oncol,2007, 18:639-646.
[15] Lau RW,Cheing GL. Managing postmastectomy lymphedema with low-level laser therapy [J]. Photomed Laser Surg,2009,27(5):763-769.
[16] Van Leeuwen RL,Dekker SK,Byers HR,et al. Modulation of alpha 4 beta 1 and alpha 5 beta 1 integrin expression:heterogeneous effects of Q-switched ruby,Nd:YAG,and alexandrite lasers on melanoma cells in vitro [J]. Lasers Surg Med,1996,18(1):63-71.
[17] Tavassoli FA,Devilee P. WHO Pathology & Genetics tumours of the breast and femal genital organ [M]. Lyon:IARC Press,2003:10.
[18] 中華人民共和国国家质量监督检验检疫总局,中国国家标准化管理委员会.GB/T12346-2006.腧穴名称与定位[S].北京:中国标准出版社,2006.
[19] 董敏,潘文,王晓萍,等.乳腺增生症与乳腺癌中医病因病机探析[J].中国中医基础医学杂志,2013,19(1):18-19.
[20] Kanakura Y,Niwa K,Kometani K,et al. Effectiveness of acupuncture and moxibustion treatment for lymphedema following intrapelvic lymph node dissection.a preliminary report [J]. Am J Chin Med,2002,30(1):37-43.
[21] 赵光,李珺,杨捷,等.中药砂仁、虎杖及桂枝萃取液对乳腺癌细胞MCF-7增殖的抑制作用[J].中国医学装备,2016,13(6):94-98.
[22] Cassileth BR,Van Zee KJ,Chan Y,et al. A safety and efficacy pilot study of acupuncture for the treatment of chronic lymphoedema [J]. Acupunct Med,2011,29(3):170-172.
[23] Mester E. The use of the laser beam in therapy [J]. Orv Hetil,1966,107(22):1012-1016.
[24] Brosseau L,Welch V,Wells G,et al. Low level laser therapy (Classes Ⅰ,Ⅱand Ⅲ) for treating osteoarthritis [J]. Cochrane Database Syst Rev,2004,12(3):CD002046.
[25] Whittaker P. Laser acupuncture:past,present,and future osteoarthritis [J]. Lasers Med Sci,2004,19(2):69-80.
[26] Chung H,Dai T,Sharma SK,et al. The nuts and bolts of low-level laser (light) therapy [J]. Ann Biomed Eng,2012, 40(2):516-533.
(收稿日期:2017-03-13 本文编辑:苏 畅)