颈内动脉假性闭塞手术治疗的单中心经验总结
2017-08-21符伟国史振宇王利新林长泼唐涵斐刘国伟郭大乔
严 栋 唐 骁 符伟国 史振宇 王利新 林长泼 唐涵斐 刘国伟 郭大乔
(复旦大学附属中山医院血管外科-复旦大学血管外科研究所 上海 200032)
颈内动脉假性闭塞手术治疗的单中心经验总结
严 栋 唐 骁 符伟国 史振宇 王利新 林长泼 唐涵斐 刘国伟 郭大乔△
(复旦大学附属中山医院血管外科-复旦大学血管外科研究所 上海 200032)
目的 评价颈内动脉假性闭塞(atheromatous pseudo-occlusion,APO)手术治疗的安全性及有效性。方法 对复旦大学附属中山医院2011年12月至2016年6月间接受颈动脉内膜切除术的颈动脉狭窄患者资料进行回顾性分析,其中研究组为APO患者32例,对照组为重度狭窄(70%~99%)患者124例。对两组围手术期各主要及次要并发症、随访中的同侧缺血性脑卒中复发率、再狭窄率及死亡率进行比较。结果 围手术期主要并发症:APO组发生心梗1例(3.1%),无缺血性脑卒中、脑出血及死亡病例;对照组发生缺血性脑卒中2例(1.4%),心肌梗死6例(4.2%),死亡1例(0.7%)。次要并发症:APO组发生切口渗血1例(3.1%),肺部感染2例(6.3%),高灌注综合征2例(6.3%);对照组发生切口渗血3例(2.1%),切口感染2例(1.4%),肺部感染4例(2.8%),颅神经损伤2例(1.4%),高灌注综合征2例(1.4%)。术后随访6~60个月,平均随访(35.3±17.5)个月。APO组1例(3.1%)同侧缺血性脑卒中复发,4例(12.5%)发生再狭窄,死亡3例(9.4%),死因均非神经系统疾病。对照组同侧缺血性脑卒中复发8例(5.6%),再狭窄9例(6.3%),死亡8例(5.6%)。两组间围手术期各主要及次要并发症,随访中的同侧缺血性脑卒中复发率、再狭窄率、死亡率的差异均无统计学意义。结论 对APO患者行颈动脉内膜切除术治疗安全有效,围手术期及随访结果满意。
动脉假性闭塞; 颈动脉内膜切除术; 缺血性脑卒中
颈内动脉假性闭塞(atheromatous pseudo-occlusion,APO)是指颈内动脉重度粥样硬化性狭窄伴有狭窄远端颈内动脉管腔变细[1](图1)。颈动脉内膜剥脱术(carotid endarterectomy,CEA)经过60余年的推广和发展,现已成为颅外颈动脉粥样硬化性狭窄的标准手术方法,近远期疗效满意[2]。然而APO病变不同于一般意义上的重度狭窄病变(70%~99%)及完全闭塞病变,有着自身的特点。对于APO患者行CEA治疗的效果目前尚存在争议[3]。本文研究目的即为探讨APO病变行CEA的安全性及有效性。
资 料 和 方 法
病例资料 对2011年12月至2016年6月因颈动脉狭窄于复旦大学附属中山医院行CEA治疗的患者资料进行回顾性分析。CEA治疗的适应证为:(1)症状性颈动脉狭窄直径狭窄率>50%,无症状性颈动脉狭窄直径狭窄率>70%[4];(2)年龄>18岁;(3)可耐受阿司匹林、氯吡格雷、肝素等药物,各项术前检查无明显手术禁忌。排除标准:(1)颈部放疗史;(2)颈部手术史;(3)3周内严重缺血性脑卒中发作;(4)全身情况差,不能耐受手术或麻醉。颈动脉直径狭窄率,颈动脉再狭窄率的计算方法参考北美症状性颈动脉内膜切除术试验(North American Symptomatic Carotid Endarterectomy Trial,NASCET)的标准[5]。颈动脉再狭窄定义为术后超过30天发生的颈动脉直径狭窄率>70%或完全闭塞[6]。所有患者治疗前签署知情同意书。
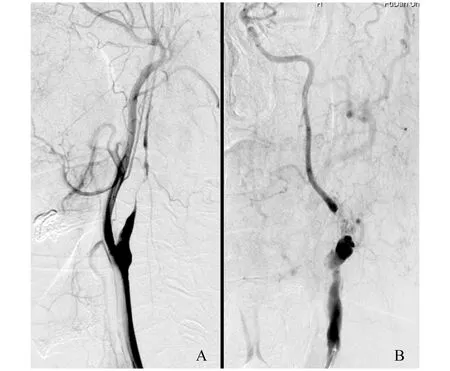
A:With distal lumen full collapse;B:Pseudo-occlusion of internal carotid artery without distal lumen full collapse.
图1 APO病变血管造影图像
Fig 1 Angiographic image of APO lesions
2011年12月至2016年6月共232例颈动脉狭窄患者于我院接受CEA治疗,其中APO 32例作为研究组,重度狭窄(70%~99%)124例作为对照组。所有患者的术前资料见表1,两组患者的一般资料特征差异在治疗前无统计学意义。
影像学评估 所有患者在术前均行颈动脉超声,颈椎动脉CT血管造影(computed tomography angiography,CTA)明确狭窄程度及病变情况。颈动脉超声或CTA怀疑为APO则进一步行颈动脉及颅内动脉数字减影血管造影(digital subtraction angiography,DSA)。DSA下满足以下4条标准中2条即可诊断为APO:(1)患侧颈内动脉重度狭窄远端直径小于对侧颈内动脉远端直径;(2)患侧颈内动脉重度狭窄远端直径小于或者等于患侧颈外动脉直径;(3)颅内血管延迟显影;(4)患侧颅内血管显影浅淡或由对侧半球血供代偿[1]。术前及术后30天内行头颅磁共振检查明确有无新发缺血性脑卒中。

表1 两组患者术前一般资料比较
COPD:Chronic obstructive pulmonary disease.
手术方法 全组患者均在全身麻醉下接受CEA,具体手术方式可参照之前文献报道[7]。打开颈动脉鞘后显露颈内动脉远心端,至管腔相对正常段。予以肝素化并在术中检测激活全血凝固时间(activated clotting time of whole blood,ACT),控制于200~250 s,阻断颈内动脉前常规诱导性升高收缩压>150 mmHg (1 mmHg=0.133 kPa,下同)。如术前影像学提示对侧颈内动脉闭塞或Willis环不完整,则术中使用转流管[7]。如术中斑块处颈内动脉直径<5 mm或动脉切开长度大于4 cm,则考虑使用补片成形[7-8]。术毕开放颈动脉后予以甘露醇125 mL快速静滴。
术后处理 术后严格监测血压及神经系统变化。如无禁忌,术后常规使用双联抗血小板治疗,口服拜阿司匹林100 mg/d及氯吡格雷75 mg/d,双联抗血小板治疗,以及他汀类降脂药物。如收缩压高于140 mmHg,则使用乌拉地尔等降压药物,甘露醇预防脑水肿等。出院后常规双联抗血小板治疗6个月,以后终身服用拜阿司匹林100 mg/d。
随访 出院后第1、3、6、12个月行超声颈动脉超声检查和神经系统评估,以后每年随访1次。如怀疑颈动脉再狭窄,则行颈椎动脉CTA或血管造影等进一步检查明确。
安全性及有效性评价 安全性评价以围手术期各主要并发症(缺血性脑卒中、心梗、死亡)及次要并发症[切口渗血、切口感染、肺部感染、颅神经损伤、高灌注综合征(cerebral hyperperfusion syndrome,CHS)等]的发生率为标准。有效性评价以随访中的同侧缺血性脑卒中复发率,再狭窄率及死亡率为标准。

结 果
APO组手术情况 颈动脉内膜切除术成功率为100% (32/32)。使用补片血管成形18例(56.25%,18/32),直接缝合14例(43.75%,14/32)。术中使用转流管8例,转流管组的颈动脉阻断时间3~7min,平均(4.6±1.4)min;无转流管组24例,颈动脉阻断时间19~60min,平均(33.8±9.8)min。
围手术期并发症情况 主要并发症:APO组发生心梗1例(3.1%),无缺血性脑卒中及死亡病例;对照组发生缺血性脑卒中2例(1.4%),心梗6例(4.3%),死亡1例(0.7%),死亡原因为急性心梗。次要并发症:APO组发生切口渗血1例(3.1%),肺部感染2例(6.3%),CHS2例(6.3%);对照组发生切口渗血3例(2.1%),切口感染2例(1.4%),肺部感染4例(2.8%),颅神经损伤2例(1.4%),CHS2例(1.4%)。两组之间围手术期各主要并发症及次要并发症发生率差异无统计学意义(表2)。
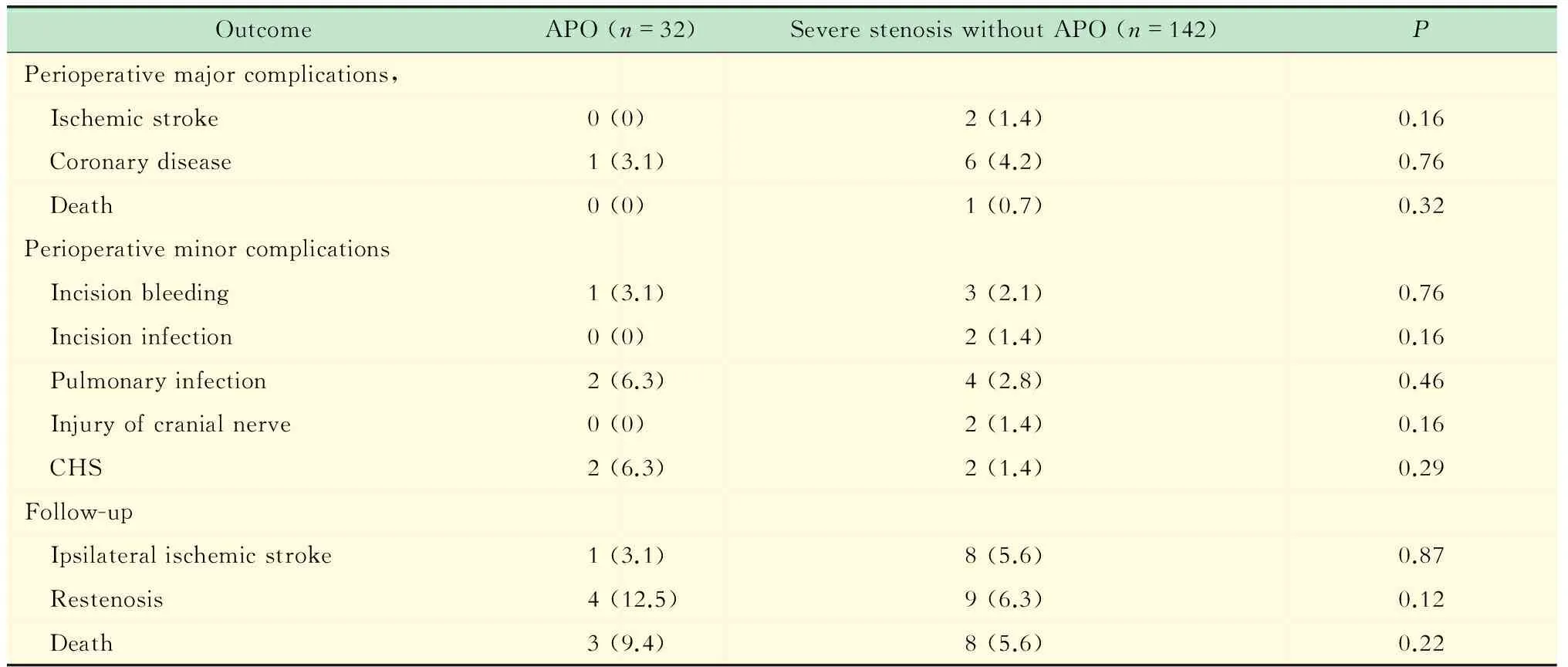
表2 两组患者围手术期和随访结果比较
CHS:Cerebral hyperperfnsion syndrome.
随访结果 术后随访6~60个月,平均随访(35.3±17.5)个月。随访中,APO组中1例(3.1%)于术后30个月同侧缺血性脑卒中复发,经过保守治疗1个月后恢复;4例(12.5%)患者发生无症状性再狭窄,2例分别于术后12个月、36个月经超声诊断为重度狭窄,后经DSA证实为再次APO;1例术后24个月超声诊断为70%直径狭窄;1例术后24个月超声诊断为完全闭塞,后经DSA证实;死亡3例(9.4%),均非神经系统原因,1例术后24个月死于急性心梗,1例术后28个月死于慢性肾功能不全并发高钾血症,1例术后36个月死于结肠癌复发。对照组同侧缺血性脑卒中复发8例(5.6%),再狭窄9例(6.3%),死亡8例(5.6%)。生存分析显示,APO行CEA治疗的5年生存率及靶血管通畅率是83.5%和80.8%,颈动脉重度狭窄行CEA治疗的5年生存率及靶血管通畅率为83.1%和89.8% (图2,3)。两组随访中的同侧缺血性脑卒中复发率、再狭窄率、死亡率的差异均无统计学意义(表2)。APO组除了再狭窄的4例,均可从血管超声或颈动脉CTA观察到远端颈内动脉不同程度的管腔直径扩张(图4)。APO组中,直接缝合的14例患者再狭窄率(28.6%,4/4)高于使用补片血管成形的18例患者(0%,0/18),差异有统计学意义(图5)。
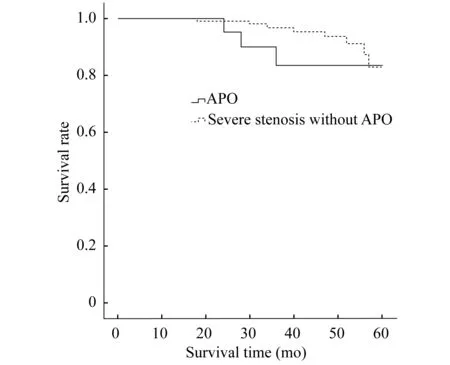
Kaplan-Meier curve analysis revealed that the five-year survival rate of the study group and control group was 83.5% and 83.1%respectively (P=0.22).
图2 两组患者生存分析
Fig 2 Analysis on survival time of the two groups
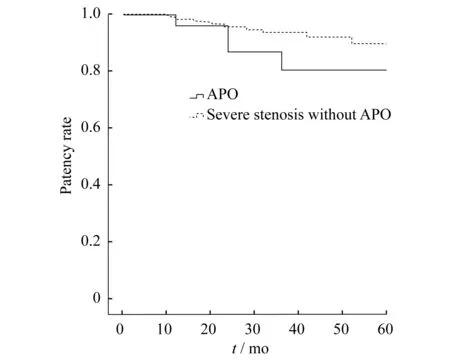
Kaplan-Meier curve analysis revealed that the five-year carotid artery patency rate of the study group and control group was 80.8% and 89.8%,respectively (P=0.12).
图3 两组患者颈动脉通畅率分析
Fig 3 Analysis on carotid artery pantency rate of the two groups

A:Preoperative DSA showed severe stenosis of internal carotid artery with the distal lumen diameter reducing;B:CTA reexamination after 1 years of operation showed that internal carotid artery patency,distal lumen diameter recovery.
图4 APO典型病例随访情况
Fig 4 Follow-up of a typical APO patient
讨 论
APO又称为“颈内动脉接近闭塞”、“颈内动脉不完全闭塞”和“颈内动脉次全闭塞”等[9],可分为伴远端管腔完全塌陷和不伴有远端管腔完全塌陷两种类型[10](图1)。两种APO类型的差异并无绝对标准。APO在国内鲜有相关报道[11],国外文献报道APO在颈动脉狭窄中的发生率为0.5%~10%[9]。因此,APO病变并不罕见,其病变特点值得临床医师关注。
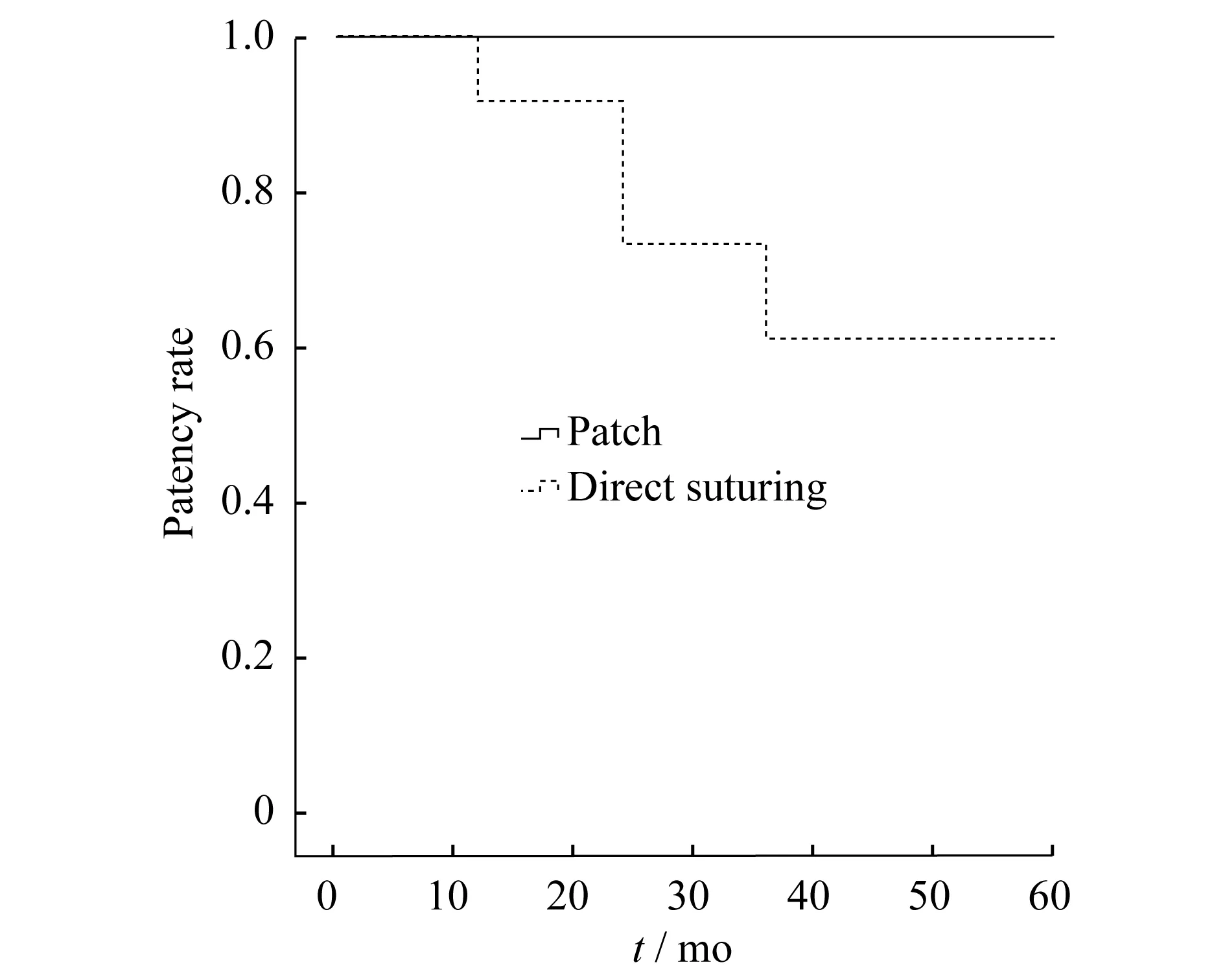
Kaplan-Meier curve analysis revealed that the five-year carotid artery patency rate of the patch group and direct suturing group was 100.0% and 61.1%,respectively (P=0.028).
图5 APO组中补片的使用与通畅率的关系
Fig 5 Relationship between patch and patency rate in APO group
APO病变的诊断需要与传统重度狭窄病变(70%~99%)、完全闭塞病变相鉴别。不同于传统重度狭窄病变,APO病变由于远端管腔塌陷,如采用NASCET法,狭窄度将被低估。而且APO病变的狭窄度也无法用具体数值来估计,因此遇到一个重度狭窄病变,应该首先评估是否为APO。DSA是诊断APO病变的金标准。如果DSA造影时没有足够时间的延迟相,APO常常会被诊断为颈内动脉完全闭塞。临床中也常常发现一些被诊断为完全闭塞的有症状的患者往往是APO。造影时还需要注意将颈外动脉分支(如咽升动脉)与管腔塌陷的颈内动脉相鉴别。但DSA因其有创且费时费力,临床上对颈动脉狭窄患者施行颈动脉内膜切除术,术前往往只行超声或CTA检查,这也会明显降低APO病变的诊出率。有文献报道时间分辨的四维CTA这项无创检查的使用可以准确识别APO病变[12],可能在未来的临床中有一定的应用价值。
NASCET及欧洲颈动脉外科试验(European Carotid Surgery Trail,ECST)中入组了246例APO不伴有远端管腔完全塌陷病例,16例APO伴有远端管腔塌陷病例[1]。有学者对这一亚组的研究发现,如仅行药物治疗APO,3年内同侧缺血性脑卒中的发生率达15.1%[1]。Johansson等[13]报道症状性颈动脉狭窄患者90天内脑卒中复发率,颈动脉狭窄率50%~99%的患者为18%,而APO伴远端颈内动脉完全塌陷的患者则高达43%。APO病变中远端管腔完全塌陷的病变具有更高的缺血性脑卒中复发率,可能因为血流量严重降低而导致局部血液潴留,增加血栓形成和栓塞风险[14]。另外,APO病变中40%的患者将在12个月内发展为完全闭塞,100%的患者将在34个月内发展为完全闭塞[15-16]。因此对于假性闭塞病变应尽早手术,以免发展为完全闭塞后而错失手术机会。
APO病变颈动脉远端血栓形成风险较一般颈动脉重度狭窄病变高。因此在准备手术期间,如无禁忌可予以低分子肝素4 000 U/q 12 h抗凝至手术前一天。手术探查颈内动脉时应该尽量更远,以防止远端合并血栓病变。如有条件可配合术中超声进行探查。另外,APO病变远端由于长期血流量不足,多已建立良好的侧支循环,因术中临时阻断而导致脑缺血的可能性较小,很少需作转流。
与颈动脉重度狭窄患者相比,APO患者行CEA治疗的风险并未明显升高[17]。我中心对于APO病变施行CEA治疗的32例患者中,围手术期仅1例发生心肌梗死,该患者予以硝酸甘油等保守治疗后症状好转,无症状性缺血性脑卒中或死亡等其他严重并发症的发生。2例发生颅脑高CHS,表现为烦躁、瞻望等精神症状,头颅CT检查未发现脑出血,予以镇静药物后均好转。严密的血压监测和控制是预防CHS的基础[18]。术后如无禁忌证使用脱水药物及小剂量激素可能对于CHS的预防亦有帮助。我们还发现切口渗血1例,清创缝合后愈合良好,肺部感染2例,均经过对症保守治疗后好转。APO组与对照组相比,围手术期主要及次要并发症的发生无统计学意义,因此CEA治疗APO病变是安全的。
32例APO患者CEA术后随访仅1例同侧缺血性脑卒中复发。因此CEA对于预防APO病变再发缺血性脑卒中的疗效令人满意。本组病例随访中发现4例再狭窄,值得注意的是这4例患者均未使用补片成形。因为补片会增加感染风险和操作时间,所以我中心实施选择性补片成形策略,即术中斑块处颈内动脉直径<5 mm或动脉切开长度>4 cm时使用补片成形[7-8]。但是对于APO病变,远端颈内动脉都有不同程度的变细,补片的使用可能会有利于远端颈内动脉重塑,降低术后再狭窄率。因此,我们认为APO病变行CEA治疗时,应更积极地使用血管补片。
APO病变行手术治疗是安全有效的。选择合适的病例,进行个性化治疗,早中期随访结果满意。但本研究病例数量有限,且为单中心回顾性分析,所以本研究的结论尚需要进一步的大宗病例研究以及长期随访予以证实。
[1] FOX AJ,ELIASZIW M,ROTHWELL PM,etal.Identification,prognosis,and management of patients with carotid artery near occlusion[J].AJNRAmJNeuroradiol,2005,26(8):2086-2094.
[2] North American Symptomatic Carotid Endarterectomy Trial C.Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis[J].NEnglJMed,1991,325(7):445-453.
[3] DESOLE A,CAMPANILE F,TOSATO F,etal.Surgical treatment for pseudo-occlusion of the internal carotid artery[J].InteractCardiovascThoracSurg,2015,20(5):636-640.
[4] BROTT TG,HALPERIN JL,ABBARA S,etal.2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS guideline on the management of patients with extracranial carotid and vertebral artery disease:executive summary[J].Stroke,2011,42(8):e420-463.
[5] NJEMANZE P,BECK O,GOMEZ C,etal.North american symptomatic carotid endarterectomy trial.Methods,patient characteristics,and progress[J].Stroke,1991,22(6):711-720.
[6] LAL BK,BEACH KW,ROUBIN GS,etal.Restenosis after carotid artery stenting and endarterectomy:a secondary analysis of CREST,a randomised controlled trial[J].LancetNeurol,2012,11(9):755-763.
[7] 郭大乔,符伟国,陈斌,等.颈动脉内膜切除术治疗颅外颈动脉重度硬化性狭窄 59 例分析[J].中国实用外科杂志,2004,24(4):217-218.
[8] MUTO A,NISHIBE T,DARDIK H,etal.Patches for carotid artery endarterectomy:current materials and prospects[J].JVascSurg,2009,50(1):206-213.
[9] JOHANSSON E,FOX AJ.Carotid near-occlusion:A comprehensive review,part 1——definition,terminology,and diagnosis[J].AJNRAmJNeuroradiol,2016,37(1):2-10.
[10] GIANNOUKAS AD,LABROPOULOS N,SMITH FC,etal.Management of the near total internal carotid artery occlusion[J].EurJVascEndovascSurg,2005,29(3):250-255.
[11] 周定标,许百男,余新光,等.颈动脉极度狭窄的诊断和手术[J].中华外科杂志,2010,48(12):908-910.
[12] NG FC,DATTA M,CHOI PM.Time-Resolved 4-Dimensional Computed-Tomography Angiography Can Correctly Identify Carotid Pseudo-Occlusion[J].JStrokeCerebrovascDis,2016,25(4):1005-1006.
[13] JOHANSSON E,ÖHMAN K,WESTER P.Symptomatic carotid near‐occlusion with full collapse might cause a very high risk of stroke[J].JInternMed,2015,277(5):615-623.
[14] OKA F,ISHIHARA H,KATO S,etal.Cerebral hemodynamic benefits after carotid artery stenting in patients with near occlusion[J].JVascSurg,2013,58(6):1512-1517.
[15] RINGELSTEIN EB,BERG-DAMMER E,ZEUMER H.The so-called atheromatous pseudoocclusion of the internal carotid artery.A diagnostic and therapeutical challenge[J].Neuroradiology,1983,25(3):147-155.
[16] RADAK DJ,TANASKOVIC S,ILIJEVSKI NS,etal.Eversion carotid endarterectomy versus best medical treatment in symptomatic patients with near total internal carotid occlusion:a prospective nonrandomized trial[J].AnnVascSurg,2010,24(2):185-189.
[17] MORGENSTERN LB,FOX AJ,SHARPE BL,etal.The risks and benefits of carotid endarterectomy in patients with near occlusion of the carotid artery.North American Symptomatic Carotid Endarterectomy Trial (NASCET) Group[J].Neurology,1997,48(4):911-915.
[18] STONEHAM M,THOMPSON J.Arterial pressure management and carotid endarterectomy[J].BrJAnaesth,2009,102(4):442-452.
Surgical treatment for atheromatous pseudo-occlusion of the internal carotid artery:a single center experience
YAN Dong, TANG Xiao, FU Wei-guo, SHI Zhen-yu, WANG Li-xin,LIN Chang-po, TANG Han-fei, LIU Guo-wei, GUO Da-qiao△
(DepartmentofVascularSurgery,ZhongshanHospital-InstituteofVascularSurgery,FudanUniversity,Shanghai200032,China)
Objective To investigate the efficacy and safety of surgical treatment for internal carotid artery atheromatous pseudo-occlusion (APO). Methods Clinical data of patients with carotid artery stenosis treated by carotid endarterectomy from Dec.,2011 to Jun.,2016 in Zhongshan Hospital Affiliated to Fudan University were analyzed retrospectively.Carotid endarterectomy were performed in 32 patients with pseudo-occlusion of the internal carotid artery (APO group).And 124 patients with traditional severe stenosis (70%-99%) served as control group.Perioperative major and minor complications,recurrence rate of ipsilateral ischemic stroke,restenosisrate and mortality in follow-up were compared between the two groups. Results Perioperative major complications:one patient (3.1%) developed myocardial infarction in the APO group,no ischemic stroke,cerebral hemorrhage and death cases;2 (1.4%) ischemic stroke cases,6 (4.2%) myocardial infarction cases and 1 (0.7%) death case was found in control group.Perioperative minor complications:1 (3.1%) incision bleeding case,2 (6.3%) pulmonary infection cases,2 (6.3%) cerebral hyperperfusion syndrome cases were found in APO group;3 (2.1%) incision bleeding cases,2 (1.4%) incision infection cases,4 (2.8%) pulmonary infection cases,2 (1.4%) cranial nerve injury cases,2 (1.4%) cerebral hyperperfusion syndrome cases were found in control group.Patients were followed up for 6-60 months,with mean follow-up period of (35.3±17.5) months.During follow-up,1 (3.1%) ipsilateral ischemic stroke recurrence case,4 (12.5%) restenosis cases,and 3 (9.4%) death cases were found in the APO group.And 8 (5.6%) ipsilateral ischemic stroke recurrence cases,9 (6.3%) restenosis cases,8 (5.6%) death cases were found in control group.There were no significant differences in perioperative major and minor complications,recurrence rate of ipsilateral ischemic stroke,restenosis rate and mortality between the two groups. Conclusions Surgical treatment for atheromatous pseudo-occlusion of the internal carotid artery is safe and effective.Perioperative and follow-up results are satisfactory.
atheromatous pseudo-occlusion; carotid endarterectomy; cerebral ischemic stroke
国家自然科学基金(81570433);上海市科委基金(14411962300)
R622+.4
A
10.3969/j.issn.1672-8467.2017.04.011
2016-12-30;编辑:沈玲)
△Corresponding author E-mail:guo.daqiao@zs-hospital.sh.cn
*This work was supported by the National Natural Science Foundation of China (81570433) and the Foundation of Science and Technology Commission of Shanghai Municipality (14411962300).
