DRD2基因多态性与冠状动脉旁路移植术后谵妄的关联研究
2017-06-09李晓晴刘水平姜霁雯郑海亮
李晓晴, 刘水平, 姜霁雯, 袁 鹏, 郑海亮
(1. 首都医科大学附属北京安贞医院, 北京, 100029; 2. 首都医科大学附属北京世纪坛医院 医学工程处, 北京, 100038)
DRD2基因多态性与冠状动脉旁路移植术后谵妄的关联研究
李晓晴1, 刘水平1, 姜霁雯1, 袁 鹏1, 郑海亮2
(1. 首都医科大学附属北京安贞医院, 北京, 100029; 2. 首都医科大学附属北京世纪坛医院 医学工程处, 北京, 100038)
目的 研究DRD2基因多态性与冠状动脉旁路移植术后谵妄的相关性及其危险因素。方法 以150例冠状动脉旁路移植手术住院患者为研究对象,以《谵妄分级量表-98修订版》作为谵妄诊断工具,分析术后谵妄的发生率和危险因素。采用基因测序法确定DRD2的多态性,分析rs6275、ts6277多态性与谵妄的相关性。结果 术后谵妄发生率为8.0%(12/150); 2. 组间单因素分析显示脑梗死(OR=0.784, 95%CI 0.631~0.975,P=0.024)、手术持续时间(OR=2.251, 95%CI 0.941~5.380,P=0.048)、体外循环时间(OR=1.057, 95%CI 0.703~1.590,P=0.029)、ICU病房时间(OR=1.890, 95%CI 1.201~2.973,P=0.005)差异有统计学意义(P<0.05); 2组间的rs6275基因型差异无统计学意义(OR=1.265, 95%CI 0.697~2.303,P=0.651); rs6277基因型在2组间的分布差异有统计学意义(OR=2.276, 95%CI 1.142~4.523,P=0.049); Logistic多因素回归分析显示,脑梗死(OR=1.861, 95%CI 1.082~3.163,P=0.024)、ICU持续时间(OR=6.757, 95%CI 2.376~19.267,P=0.001)、rs6277的CC基因型(OR=4.019, 95%CI 1.395~12.341,P=0.012)是术后谵妄的危险因素。 结论 对术前合并脑梗死的高危患者进行DRD2基因筛查,有助于评估谵妄发生的可能性。
冠状动脉旁路移植术; 术后谵妄发生率; 危险因素
术后谵妄(POD)是在手术、麻醉后出现的急性、波动性认知功能障碍,是在患者易感素质的基础上,由围术期的多种因素共同作用所促发[1-2]。尽管心脏手术和麻醉技术日益成熟, POD仍是冠状动脉旁路移植术(CABG)术后神经系统急性并发症之一, POD延长住院时间、增加医疗费用、延缓功能恢复。最新的研究[3-4]显示,术后谵妄还与术后持续认知功能障碍(POCD)、痴呆密切相关。POD的发病机制尚不十分清楚,基因易感性和生物标志物已成为谵妄研究的新热点[5]。多巴胺受体阻断剂能够有效控制谵妄症状,使得多巴胺能系统成为谵妄研究的候选基因之一[6]。本研究旨在探讨多巴胺D2受体(DRD2)与谵妄的相关性[7], 为早期预防提供依据。
1 资料与方法
1.1 一般资料
连续纳入2014年1—12月本院心脏外科CABG手术的住院患者150例为研究对象。男95例,女55例,平均年龄(62.8±7.1)岁。根据是否发生POD将研究对象分为研究组(谵妄组)12例和对照组(非谵妄组)138例。谵妄诊断标准:采用美国《精神疾病诊断与统计手册-第五版》[8](《DSM-V》)的诊断标准,以谵妄分级量表-98修订版(DRS-R-98)[9]作为谵妄的诊断和鉴别诊断工具,该量表内容分为2部分: ① 3个诊断项目,包括“症状发生时间”“症状波动性”和“躯体疾病”,鉴别诊断谵妄、痴呆、精神分裂症等; ② 13个严重程度项目,包括“睡眠觉醒周期紊乱” 、“感知障碍”、“妄想”、“情感易变性”、“言语”、“思维过程”、“精神运动性激越”、“精神运动性迟滞”、“注意力”、“短时记忆”、“定向障碍”、“长时记忆”和“视空间能力”。每个项目根据不同程度分为0~3分,累计积分, DRS-R-98≥12分则诊断谵妄。入选标准:冠状动脉旁路移植术后,包括体外循环下行冠状动脉旁路移植手术(On-CABG)和非体外循环下行冠状动脉旁路移植手术(Off-CABG); 符合谵妄的诊断标准, DRS-98≥12分; 术前无认知功能障碍,简易精神状态检查量表(MMSE)评分:文盲≥17 分; 小学≥20分; 中学及以上≥24 分; 术前无焦虑、抑郁,医院焦虑抑郁量表(HADS)评分≤7分; 同意参加试验并签署知情同意书。排除标准:术后发生脑卒中,包括缺血性及出血性脑卒中; 因其他因素引起术后意识障碍者; 严重视听障碍,无法配合神经系统查体、认知功能测试及其他神经系统功能评估; 同时进行两种及以上的心脏手术者。
1.2 多巴胺受体D2(DRD2)基因型测定方法
采用基因测序法确定研究对象的DRD2基因型。采用Promega DNA纯化试剂盒抽提全血DNA, 然后进行DRD2基因PCR扩增。
DRD2 rs6275设计引物,上游: 5′gccgactcaccgagaaca 3′; 下游5′ggctgatgcctgggaact 3′。25 μL PCR扩增反应体系包括10(PCR缓冲液2.5 μL+2.5 mmol/L的dNTP混合液2 μL+上游引物(10 μmol/L)0.5 μL+下游引物(10 μmol/L)0.5 μL+DNA(200 ng/μL)2 μL +Taq DNA聚合酶(5 μg/μL)0.2 μL+ddH2O 17.3 μL =25 μL。循环条件: 95 ℃ 5 min, (94 ℃ 30 s, 51.8 ℃ 30 s, 72 ℃ 30 s)共30个循环; 最后72 ℃ 5 min, 纯化PCR产物。
DRD2 rs6277设计引物,上游: 5′gccgactcaccgagaaca 3′; 下游5′ggctgatgcctgggaact 3′。25 μL PCR扩增反应体系包括10(PCR缓冲液2.5 μL+2.5 mmol/L的dNTP混合液2 μL+上游引物(10 μmol/L) 0.5 μL+下游引物(10 μmol/L) 0.5 μL+DNA(200 ng/μL) 2 μL +Taq DNA聚合酶(5 μg/μL) 0.2 μL+ddH2O 17.3 μL =25 μL。循环条件: 95 ℃ 5 min, 94 ℃ 30 s, 59.9 ℃ 30 s, 72 ℃ 30 s共30个循环; 最后72 ℃ 5 min, 纯化PCR产物。扩增产物进行直接测序,采用DNA Star软件比对, chromas软件判断基因型。
1.3 观察指标
将观察指标分为3大类,分别为术前因素(既往病史和一般资料),术中因素(手术过程),术后因素(术后监护室以及返回病房后)。术前因素包括年龄、性别、吸烟、饮酒、糖尿病、左室射血分数(LVEF)、高血压、房颤(AF)、脑梗死、脑出血。术中因素包括手术持续时间、麻醉持续时间、体外循环持续时间、术中平均动脉压(MAP)、手术方式(体外循环下手术和非体外循环下手术)。术后因素包括重症监护病房(ICU)持续时间、机械通气时间(CMV)、平均动脉压、血氧饱和度(SaO2)、发热、心率、血红蛋白(Hb)、术后视觉模拟疼痛评分法的疼痛(VAS)评分。
1.4 统计学处理
2 结 果
2.1 2组间单因素分析
将2组患者围术期指标分为3大类型,即术前、术中和术后危险因素,并对这3大类指标进行单因素分析。与POD发生有关的危险因素包括既往脑梗死 (OR=0.784, 95% CI 0.631~0.975,P=0.024); 手术持续时间(OR=2.251, 95% CI 0.941~5.380,P=0.048); 体外循环时间(OR=1.057, 95% CI 0.703~1.590,P=0.029); ICU病房时间(OR=1.890, 95% CI 1.201~2.973,P=0.005), 上述各因素对POD的影响差异有统计学意义(P<0.05)。见表1、2、3。

表1 POD的术前危险因素分析[n(%)]
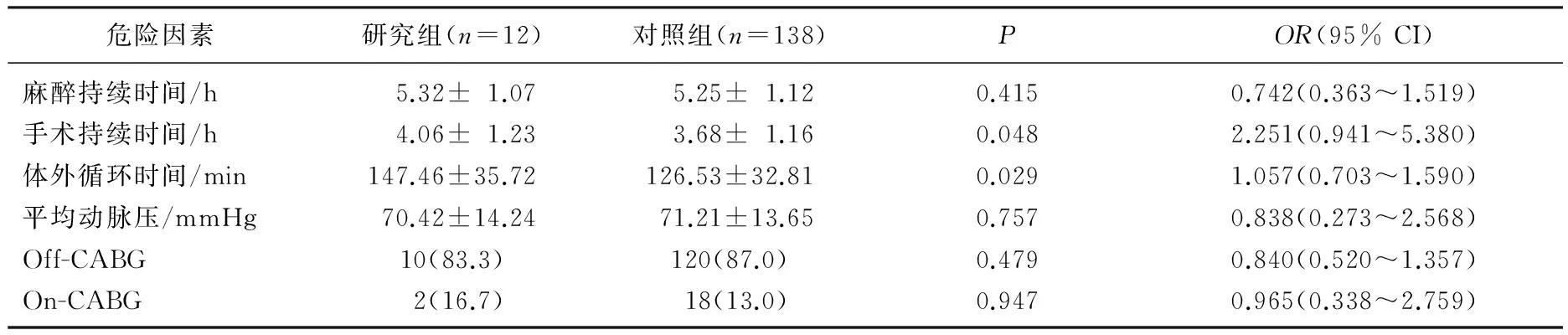
表2 POD的术中危险因素分析[n(%)]
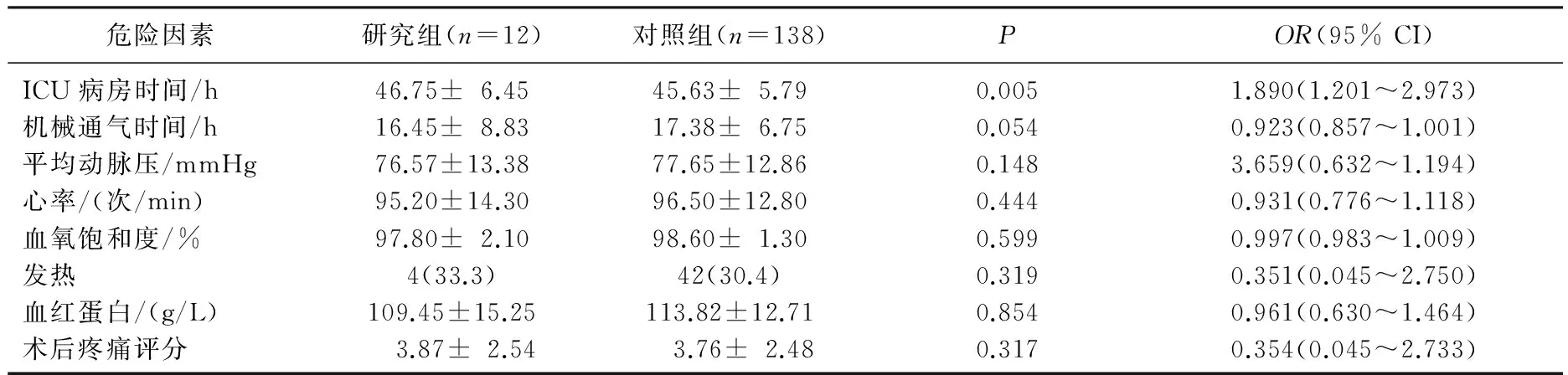
表3 POD的术后危险因素分析
2.2 DRD2基因多态性与POD的关联
2.2.1 rs6275和rs6277的基因频率和基因型以及Hardy-Weinberg遗传平衡检验: DRD2位于染色体11q23, 第7号外显子的2个位点即rs6275和rs6277分别存在同义突变即939T>C和957C>T, 见表4。rs6275等位基因C的频率为43.7%, 等位基因T的频率为56.3%。3种基因型CC、CT、TT的频率分别为15.3%、56.7%、28.0%。rs6277等位基因C的频率为88.0%, 等位基因T的频率为12.0%。3种基因型CC、CT、TT的频率分别为78.7%、18.7%、2.6%, 见表5。经Hardy-Weinberg平衡定律检验, rs6275和rs6277的基因型频率的分布符合遗传平衡(P>0.05), 样本来自同一孟德尔群体。

表4 rs6275和rs6277的基本特征
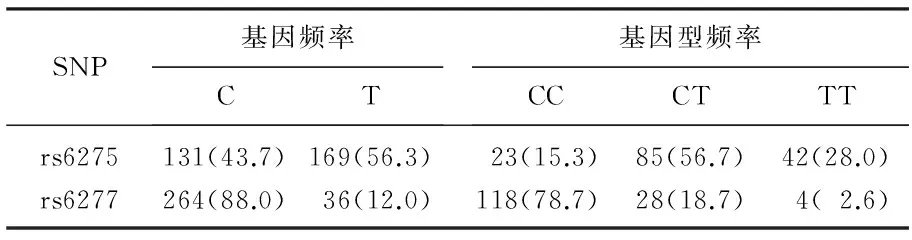
表5 rs6275和rs6277位点基因频率及基因型分布[n(%)]
2.2.2 2组中rs6275和rs6277基因和基因型频率的结果: 2组间的rs6275等位基因频率差异无统计学意义(OR=1.056, 95% CI 0.727~1.733,P=0.775); rs6275基因型在2组间的分布差异亦无统计学意义(OR=1.265, 95% CI 0.697~2.303,P=0.651)。2组间的rs6277等位基因频率差异显著(OR=3.857, 95% CI 1.727~8.663,P=0.001); rs6277基因型在2组间的分布差异有统计学意义(OR=2.276, 95% CI 1.142~4.523,P=0.049)。见表6。

表6 2组中rs6275和rs6277基因和基因型频率比较
2.2.3 多因素回归分析:多因素Logistic逐步回归分析结果显示,与POD发生有关的因素包括脑梗死、ICU持续时间、rs6277的CC基因型。见表7。

表7 POD的Logsistic多因素回归分析结果
3 讨 论
POD是CABG常见的并发症之一,与围术期的多种因素有关[10]。脑血管病是发生POD的高危因素。术前“认知正常”的患者,头部核磁检查可以发现脑白质疏松、腔隙性梗死等多种脑小血管病变(SVD)[11], 脑血管病变导致神经元损失、突触数目减少、神经环路受损、认知障碍发生阈值降低,在此基础上, CABG手术应激可诱发系统性炎症反应,增加血脑屏障通透性,炎症因子TNF等进一步诱发急性脑损伤,导致乙酰胆碱、五羟色胺、多巴胺等神经递质失衡,产生谵妄[12]。
POD与ICU病房观察时间延长有关。ICU时间长与手术时间长、创伤大、术后并发症等多种因素有关,对中枢神经系统等重要器官的影响亦增加。ICU也是一种特殊环境,常有机械辅助通气、肢体约束、留置胃管尿管、密切监测护理等,容易诱发谵妄[13]。
本研究首创性的观察了多巴胺受体基因多态性与术后谵妄的关联性。多巴胺是重要的神经递质,多巴胺与乙酰胆碱神经递质失衡是谵妄的发病机制之一[14]。脑内有3条主要的多巴胺能神经通路,分别是黑质纹状体通路、中脑边缘系统通路以及漏斗结节通路。多巴胺递质与多巴胺受体(DRs)结合,发挥调节运动、认知、学习、记忆、情感、内分泌功能的重要作用。多巴胺受体有5种亚型D1~D5。最近的荟萃分析、横断面流行病学研究以及基因多态性研究结果均提示多巴胺受体基因与谵妄、酒精依赖、精神分裂症、神经退行性疾病有关[15]。多巴胺D2受体(DRD2)编码基因位于染色体11q22-q24,其单核苷酸多态性(SNP)成为目前的研究热点。本研究首创性的观察了DRD2基因位于第7外显子的两种同义突变rs6275(C/T)和rs6277(C/T)[16-17]与术后谵妄的关系。经Hardy-Weinberg平衡定律检验, rs6275和rs6277的基因型频率的分布符合遗传平衡(P>0.05), 样本来自同一孟德尔群体,具有代表性。本研究发现, rs6277的C等位基因是术后谵妄的危险因素(P=0.001,OR=3.857, 95% CI 1.727~8.663)。虽然rs6277(C/T)是同义突变,表达的氨基酸相同,但是细胞研究[18-20]显示, C/T等位基因的差异显著影响DRD2的mRNA的稳定性和表达数量。健康志愿者的人体试验进一步显示纹状体、皮质、丘脑不同脑区域的多巴胺受体的亲和性和密度受rs6277(C/T)突变影响, C/C纯合子的DRD2亲和性最强, T/T纯合子的亲和性最弱。据此推测rs6277(C/T)突变通过增加多巴胺能神经活性,导致多巴胺与乙酰胆碱递质失衡,进而增加谵妄发生的易感性。国内外对于rs6277(C/T)与谵妄的相关性研究均为之甚少,因此需要更大规模的病例对照(case-control)研究以及更细化的表型分层,进一步确认rs6277与谵妄的相关性。
国外对rs6275(C/T)多态性的研究集中在精神分裂症[21]、偏头痛[22]、语言障碍[23]、药物滥用[24]等方面。在与谵妄的关联研究中,有关rs6275的阳性报道极少,本研究亦未发现rs6275(C/T)与术后谵妄相关。
本研究并未提示年龄是术后谵妄的独立危险因素,与国外研究结论不一致,究其原因与研究对象、手术方式、样本规模、诊断标准、评估工具等多种因素有关。本研究仅以70岁以下、既往无认知障碍的患者为研究对象。国外研究对象包含了不同年龄,特别是70岁以上的患者[25], 常合并认知功能障碍[26], 多重手术方式等。本研究采用以DRS-R-98作为谵妄的诊断工具,该量表是国际通用的谵妄筛查诊断“金标准”。 而重症监护谵妄筛查量表(ICDSC)[27]、器质性脑综合征量表[25]等亦常作为谵妄的评估量表。今后需要更细化、标准的大规模研究进一步明确谵妄的促发因素。
药物遗传学研究[28-32]显示, DRD2基因多态性可能与药物治疗的副反应相关,因此,对术前合并脑梗死的高危患者,进行DRD2基因筛查,有助于评估谵妄发生的可能性,对指导药物治疗,提高术后管理水平具有一定的应用价值。
[1] Hirsch J, DePalma G, Tsai T T, et al. Impact of intraoperative hypotension and blood pressure fluctuations on early postoperative delirium after non-cardiac surgery[J]. Br J Anaesth, 2015, 115(3): 418-426.
[2] Sanders R D, Pandharipande P P, Davidson A J, et al. Anticipating and managing postoperative delirium and cognitive decline in adults[J]. BMJ, 2011, 20 (343): d4331.
[3] Liang C K, Chu C L, Chou M Y, et al. Interrelationship of postoperative delirium and cognitive impairment and their impact on the functional status inolder patients undergoing orthopaedic surgery: a prospective cohort study[J]. PLoS One, 2014, 9(11): e110339.
[4] Wang W, Wang Y, Wu H, et al. Postoperative cognitive dysfunction: current developments in mechanism and prevention[J]. Med Sci Monit, 2014, 12, 20: 1908-1912.
[5] Androsova G, Krause R, Winterer G, et al. Biomarkers of postoperative delirium and cognitive dysfunction[J]. Front Aging Neurosci. 2015, 9(7): 112-115.
[6] Page V J, Ely E W, Gates S, et al. Effect of intravenous haloperidol on the duration of delirium and coma in critically ill patients (Hope-ICU): a randomised, double-blind, placebo-controlled trial[J]. Lancet Respir Med, 2013, 1(7): 515-523.
[7] van Munster B C, de Rooij S E, Yazdanpanah M, et al. The association of the dopamine transporter gene and the dopamine receptor 2 gene with delirium, a meta-analysis[J]. Am J Med Genet B Neuropsychiatr Genet, 2010, 153B(2): 648-655.
[8] Regier D A, Kuhl E A, Kupfer D J. The DSM-5: Classification and criteria changes[J]. World Psychiatry, 2013, 12(2): 92-98.
[9] Meagher D J, Morandi A, Inouye S K, et al. Concordance between DSM-Ⅳ and DSM-5 criteria for delirium diagnosis in a pooled database of 768 prospectively evaluated patients using the delirium rating scale-revised-98[J]. BMC Med, 2014, 30(12): 164-168.
[10] Gosselt A N, Slooter A J, Boere P R. Risk factors for delirium after on-pump cardiac surgery: a systematic review[J]. Crit Care, 2015, 19(1): 346-348.
[11] Gustavsson A M, Stomrud E, AbuL-Kasim K, et al. Cerebral Microbleeds and White Matter Hyperintensities in Cognitively Healthy Elderly: A Cross-Sectional Cohort Study Evaluating the Effect of Arterial Stiffness [J]. Cerebrovasc Dis Extra, 2015, 5(2): 41-51.
[12] Cerejeira J, Nogueira V, Luís P, et al. The cholinergic system and inflammation: common pathways in delirium pathophysiology[J]. J Am Geriatr Soc, 2012, 60(4): 669-675.
[13] Kwizera A, Nakibuuka J, Ssemogerere L, et al. Incidence and Risk Factors for Delirium among Mechanically Ventilated Patients in an African Intensive Care Setting: An Observational MuLticenter Study[J]. Crit Care Res Pract, 2015, 2015: 491780.
[14] Hshieh T T, Fong T G, Marcantonio E R, et al. Cholinergic deficiency hypothesis in delirium: a synthesis of current evidence[J]. J Gerontol A Biol Sci Med Sci, 2008, 63(7): 764-772.
[15] Rangel-Barajas C, Coronel I, Florán B. Dopamine Receptors and Neurodegeneration[J]. Aging Dis, 2015, 6(5): 349-368.
[16] Swagell C D, Lawford B R, Hughes I P, et al. DRD2 C957T and TaqIA genotyping reveals gender effects and unique low-risk and high-risk genotypes in alcohol dependence[J]. Alcohol Alcohol, 2012, 47(4): 397-403.
[17] Villalba K, Devieux J G, Rosenberg R, et al. DRD2 and DRD4 genes related to cognitive deficits in HIV-infected adults who abuse alcohol[J]. Behav Brain Funct, 2015, 11: 25-27.
[18] Bali V, Bebok Z. Decoding mechanisms by which silent codon changes influence protein biogenesis and function[J]. Int J Biochem Cell Biol, 2015, 64: 58-74.
[19] Stoicea N, McVicker S, Quinones A, et al. Delirium-biomarkers and genetic variance[J]. Front Pharmacol, 2014, 5: 75-78.
[20] Hirvonen M M, Lumme V, Hirvonen J, et al. C957T polymorphism of the human dopamine D2 receptor gene predicts extrastriatal dopamine receptor availability in vivo[J]. Prog Neuropsychopharmacol Biol Psychiatry, 2009, 33(4): 630-636.
[21] Liu L, Fan D, Ding N, et al. The relationship between DRD2 gene polymorphisms (C957T and C939T) and schizophrenia: a meta-analysis[J]. Neurosci Lett, 2014, 583: 43-48.
[22] Ghosh J, Pradhan S, Mittal B. Role of dopaminergic gene polymorphisms (DBH 19 bp indel and DRD2 Nco I) in genetic susceptibility to migraine in North Indian population[J]. Pain Med, 2011, 12(7): 1109-1111.
[23] Lan J, Song M, Pan C, et al. Association between dopaminergic genes (SLC6A3 and DRD2) and stuttering among Han Chinese[J]. J Hum Genet, 2009, 54(8): 457-460.
[24] Onaya T, Ishii M, Katoh H, et al. Predictive index for the onset of medication overuse headache in migraine patients[J]. Neurol Sci, 2013, 34(1): 85-92.
[25] SmuLter N, Lingehall H C, Gustafson Y, et al. Delirium after cardiac surgery: incidence and risk factors [J]. Interact Cardiovasc Thorac Surg, 2013, 17(5): 790-796.
[26] Otomo S, Maekawa K, Goto T, et al. Preexisting cerebral infarcts as a risk factor for delirium after coronary artery bypass graft surgery [J]. Interact Cardiovasc Thorac Surg, 2013, 17(5): 799-804.
[27] Norkien I, Ringaitien D, Kuzminskait V, et al. Incidence and risk factors of early delirium after cardiac surgery [J]. Biomed Res Int, 2013, 2013: 323491.
[28] Llerena A, Berecz R, Pe as-Lledó E, et al. Pharmacogenetics of clinical response to risperidone[J]. Pharmacogenomics, 2013, 14(2): 177-194.
[29] López-Rodríguez R, Cabaleiro T, Ochoa D, et al. Pharmacodynamic genetic variants related to antipsychotic adverse reactions in healthy volunteers[J]. Pharmacogenomics, 2013, 14(10): 1203-1214.
[30] Zivkovi M, Mihaljevi -Peles A, Bozina N, et al. The association study of polymorphisms in DAT, DRD2, and COMT genes and acute extrapyramidal adverse effects in male schizophrenic patients treated with haloperidol[J]. J Clin Psychopharmacol, 2013, 33(5): 593-599.
[31] 陈大球, 高允锁, 郭敏, 等. 海南汉族人群创伤后应激障碍患者与5-HTTLPR基因多态性的相关性[J]. 南方医科大学学报, 2015, 35(9): 1366-1368.
[32] 张凡凡, 樊明强, 柳茵, 等. 青海地区冠心病患者载脂蛋白E基因多态性与血脂的研究[J]. 海南医学院学报, 2012, 18(9): 1256-1258.
Association ation study of dopamine D2 receptor gene polymorphism with postoperative delirium in the patients underwent coronary artery bypass grafting
LI Xiaoqing1, LIU Shuiping1, JIANG Jiwen1, YUAN Peng1, ZHENG Hailiang2
(1.DepartmentofNeurology,BeijingAnzhenHospitalAffiliatedtoCapitalMedicalUniversity,Beijing, 100029; 2.DepartmentofMedicalEngineer,ShijitanHospitalAffiliatedtoCapitalMedicalUniversity,Beijing, 100038)
Objective To investigate the assoCI ation between DRD2 gene polymorphism and postoperative delirium in the patients undergoing coronary artery bypass grafting (CABG) and to analyze the risks of postoperative delirium. Methods A total 150 patients after coronary artery bypass grafting were enrolled. And delirium rating scale-revised-98 was used as diagnosis tool for the analysis of morbidity and risks of postoperative delirium. DRD2 genotypes were determined by sequenCI ng analysis. The assoCI ation of rs6275 and rs6277 with delirium was studied. Results Delirium occurred in 12 patients and morbidity of postoperative delirium was 8.0%. Univariate logistic regression analysis results showed that delirium was assoCI ated with previous cerebral infarction (OR=0.784, 95% CI 0.631 to 0.975,P=0.024), extracorporeal CI rculation time(OR=1.057, 95% CI 0.703 to 1.590,P=0.029), surgery time (OR=2.251, 95% CI 0.941 to 5.380,P=0.048) and intensive care unit time (OR=1.890, 95% CI 1.201 to 2.973,P=0.005).There were no significant differences in frequencies of genotype and alleles of rs6275 polymorphism between patients with delirium and controls(OR=1.265, 95% CI 0.697 to 2.303,P=0.651). There were significant differences on frequencies of genotype and alleles of rs6277 polymorphism between patients with delirium and controls(OR=2.276, 95% CI 1.142 to 4.523,P=0.049). The multiple logisticstepwise regression analysis indicated that the perioperative risk factors of delirium included cerebral infarction (OR=1.861, 95% CI 1.082 to 3.163,P=0.024), ICU duration time (OR=6.757, 95% CI 2.376 to 19.267,P=0.001)and CC genotype of rs6277 (OR=4.019, 95% CI 1.395 to 12.341,P=0.012). Conclusion DRD2 gene testing in patients with high risks may be helpful for the prevention of postoperative delirium.
coronary artery bypass grafting; incidence of postoperative delirium; risk factors
2016-12-05
北京市自然科学基金项目(1152003)
郑海亮, E-mail: 15811197824@163.com
R 541
A
1672-2353(2017)09-006-06
10.7619/jcmp.201709002
