高磷血症与糖尿病肾病患者肾小球滤过率及远期预后的相关性分析
2017-05-18钱勇广东省信宜市人民医院肾内科广东茂名525300
钱勇(广东省信宜市人民医院肾内科,广东茂名525300)
高磷血症与糖尿病肾病患者肾小球滤过率及远期预后的相关性分析
钱勇
(广东省信宜市人民医院肾内科,广东茂名525300)
目的研究高磷血症与糖尿病肾病患者肾小球滤过率及远期预后的相关性。方法收集2011年3月至2015年9月期间收治的109例确诊为2型糖尿病肾病患者作为研究对象,观察患者的高磷血症发生率、血磷水平和肾小球滤过率的相关性,以及血磷水平对糖尿病肾病患者远期预后的预测价值。结果本组109例患者,共24例发生高磷血症,发生率为22.0%。其中,肾小球滤过率<60 mL/(min·1.73m2),患者高磷血症发生率为32.1%,肾小球滤过率为60~90 mL/(min·1.73m2),患者高磷血症发生率为16.7%,肾小球滤过率>90 mL/(min·1.73m2),患者高磷血症发生率为10.5%。高磷血症的发生率随着肾小球滤过率的降低而增高。高磷血症患者女性比例增加,尿蛋白升高,血钙降低,总胆固醇升高,血浆总蛋白降低,肾小球滤过率降低。随着肾小球滤过率的降低,血磷水平越高,患者发生终末型肾病的风险也越高。结论糖尿病肾病患者高磷血症的发生率较高,高磷血症同时和肾脏的受损程度显著相关,并且是影响患者发生终末型肾病的独立危险因素,对预测患者的远期预后有一定价值。
高磷血症;糖尿病肾病;终末期肾病;慢性肾脉病
磷是人体必不可少的元素之一,它参与了人体中多种细胞活动,诸如新陈代谢、骨骼发育、能量传递、信号传导以及蛋白质功能调节等[1]。正常人血磷稳态的维持主要依靠多种脏器的调节协同,包括骨骼系统、消化系统、泌尿系统和内分泌系统。此外,血磷的调节也会受到一些分子调控,比如甲状旁腺素、1.25-二羟维生素D、成纤维细胞生长因子-23等,而血磷、血糖、尿量、甲状旁腺素、1.25-二羟维生素D、成纤维细胞生长因子-23和肾脏的排泄磷的能力亦密切相关[2]。在慢性肾脏病(CKD)中,高磷血症是其特征之一,CKD早期,肾脏会代偿性的增加对磷的排泄以确保机体的血磷水平保持在正常范围之内,但是这种代偿性的排泄又会加快CKD的进程,造成肾脏损伤,肾脏的损伤又影响到机体对磷的转运和重吸收,形成一个恶性循环[3]。本文将糖尿病肾病患者作为研究对象,探讨高磷血症与糖尿病肾病患者肾小球滤过率及远期预后的相关性,现报告如下。
1 资料与方法
1.1 一般资料:研究对象为本院2011年3月至2015年9月期间收治入院的109例确诊为2型糖尿病肾病患者。
1.2 观察指标:收集患者的临床资料包括性别、年龄、体重、身高、血压、空腹血糖、糖化血红蛋白、24 h尿蛋白定量、肾小球滤过率、总胆固醇、血清钙、血清磷、血浆总蛋白等[4]。根据肾小球滤过率将患者分为<60 mL/(min·1.73m2)、60~90 mL/(min·1.73m2)>90 mL/(min·1.73m2)三组,记录不同CKD患者发生高磷血症的情况。随访至少12个月,观察终点为终末期肾病。如果患者出现终末期肾病,则最后一次的随访数据作为该患者的最终数据。
1.3 统计学处理:采用SPSS18.0软件进行统计分析,计量资料采用方差分析,计数资料采用χ2检验,P<0.05为差异有统计学意义。
2 结果
2.1 一般情况:109例糖尿病肾病患者的平均年龄为(41.8±9.2)岁,肾小球滤过率平均为(73.15±30.61)mL/(min·1.73m2),高磷血症患者的年龄偏低,女性比例增加,尿蛋白升高,血钙降低,总胆固醇升高,血浆总蛋白降低,肾小球滤过率降低,差异有统计学意义(P<0.05)。本组109例患者,共24例发生高磷血症,发生率为22.0%。其中,肾小球滤过率<60 mL/(min·1.73m2)的患者有53例,高磷血症的有17例,发生率为32.1%;肾小球滤过率为60~90 mL/(min· 1.73m2)的患者共有18例,高磷血症的有3例,发生率为16.7%;肾小球滤过率>90 mL/(min·1.73m2)的患者共有38例,高磷血症的有4例,发生率为10.5%。高磷血症的发生率随着肾小球滤过率的降低而增高,详见表1。
2.2 血磷水平对糖尿病肾病患者远期预后的预测价值:在肾小球滤过率>90 mL/(min·1.73m2)的患者组中,血磷水平>1.45 mmol/L将增加患者发生终末期肾病的风险(HR=1.24,95%CI:0.98~1.56,P= 0.004),但是血磷水平为1.17~1.45 mmol/L的患者发生终末型肾病的风险不会增加。在肾小球滤过率为60~90 mL/(min·1.73m2)的患者,不仅血磷水平>1.45 mmol/L将增加患者发生终末型肾病的风险(HR=1.58,95%CI:1.10~2.28,P<0.001),而且血磷水平为1.17~1.45 mmol/L的患者也会增加发生终末型肾病的风险(HR=1.43,95%CI:1.17~1.75,P<0.001)。说明随着肾小球滤过率的降低,血磷水平越高,患者发生终末期肾病的风险也越高。
3 讨论
已有较多研究证实高磷血症可以增加CKD的心血管风险[5-6],CKD早期的患者肾小球滤过率处在60~90 mL/(min·1.73m2)之间,临床上对于此类患者高磷血症的发生率、血磷水平和肾脏损伤的相关性以及对于肾脏损伤的远期预后的预测价值尚未引起足够的重视。
本研究发现,在2型糖尿病患者中,肾小球滤过率为60~90 mL/(min·1.73m2)患者的高磷血症发生率为16.4%;肾小球滤过率>90 mL/(min·1.73m2)患者的发生率为11.9%,相比较之前的研究来说,高磷血症发生率是有所升高的[7]。同时,本研究显示性别、年龄、蛋白尿、胆固醇水平均会影响血磷水平,其中年龄较小、女性比例增加、尿蛋白增加、胆固醇高是引起血磷升高的相关因素。尿蛋白升高可影响近端小管的重吸收从而使血磷水平升高,胆固醇升高可以增加心血管风险,而高磷血症也可以增加心血管风险,两者可能存在一定的相关性,这提示我们在临床工作中遇到此类因素时需密切监测血磷水平。
综上所述,糖尿病肾病早期的患者高磷血症的发生率增高,高磷血症同时和肾脏的受损程度显著相关,并且是影响患者发生终末期肾病的独立危险因素,对预测患者的远期预后有一定价值。
表1 不同血磷水平DN患者的基线资料比较(±s)
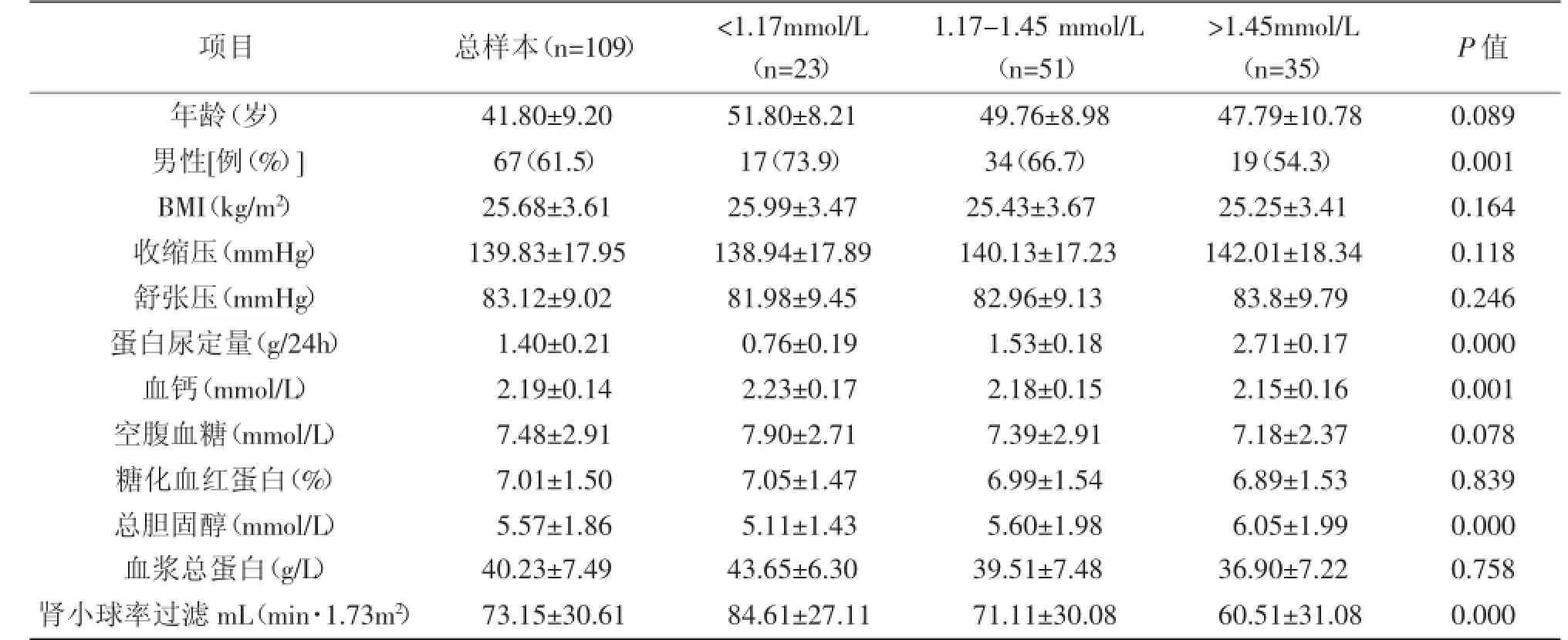
表1 不同血磷水平DN患者的基线资料比较(±s)
项目总样本(n = 1 0 9)<1 . 1 7 m m o l / L(n = 2 3)1 . 1 7 -1 . 4 5 m m o l / L(n = 5 1)>1 . 4 5 m m o l / L(n = 3 5)P值年龄(岁)4 1 . 8 0 ± 9 . 2 0 5 1 . 8 0 ± 8 . 2 1 4 9 . 7 6 ± 8 . 9 8 4 7 . 7 9 ± 1 0 . 7 8 0 . 0 8 9男性[例(%)] 6 7(6 1 . 5)1 7(7 3 . 9)3 4(6 6 . 7)1 9(5 4 . 3)0 . 0 0 1 B M I(k g / m2)2 5 . 6 8 ± 3 . 6 1 2 5 . 9 9 ± 3 . 4 7 2 5 . 4 3 ± 3 . 6 7 2 5 . 2 5 ± 3 . 4 1 0 . 1 6 4收缩压(m m H g)1 3 9 . 8 3 ± 1 7 . 9 5 1 3 8 . 9 4 ± 1 7 . 8 9 1 4 0 . 1 3 ± 1 7 . 2 3 1 4 2 . 0 1 ± 1 8 . 3 4 0 . 1 1 8舒张压(m m H g)8 3 . 1 2 ± 9 . 0 2 8 1 . 9 8 ± 9 . 4 5 8 2 . 9 6 ± 9 . 1 3 8 3 . 8 ± 9 . 7 9 0 . 2 4 6蛋白尿定量(g / 2 4 h)1 . 4 0 ± 0 . 2 1 0 . 7 6 ± 0 . 1 9 1 . 5 3 ± 0 . 1 8 2 . 7 1 ± 0 . 1 7 0 . 0 0 0血钙(m m o l / L)2 . 1 9 ± 0 . 1 4 2 . 2 3 ± 0 . 1 7 2 . 1 8 ± 0 . 1 5 2 . 1 5 ± 0 . 1 6 0 . 0 0 1空腹血糖(m m o l / L)7 . 4 8 ± 2 . 9 1 7 . 9 0 ± 2 . 7 1 7 . 3 9 ± 2 . 9 1 7 . 1 8 ± 2 . 3 7 0 . 0 7 8糖化血红蛋白(%)7 . 0 1 ± 1 . 5 0 7 . 0 5 ± 1 . 4 7 6 . 9 9 ± 1 . 5 4 6 . 8 9 ± 1 . 5 3 0 . 8 3 9总胆固醇(m m o l / L)5 . 5 7 ± 1 . 8 6 5 . 1 1 ± 1 . 4 3 5 . 6 0 ± 1 . 9 8 6 . 0 5 ± 1 . 9 9 0 . 0 0 0血浆总蛋白(g / L)4 0 . 2 3 ± 7 . 4 9 4 3 . 6 5 ± 6 . 3 0 3 9 . 5 1 ± 7 . 4 8 3 6 . 9 0 ± 7 . 2 2 0 . 7 5 8肾小球率过滤m L(m i n · 1 . 7 3 m2)7 3 . 1 5 ± 3 0 . 6 1 8 4 . 6 1 ± 2 7 . 1 1 7 1 . 1 1 ± 3 0 . 0 8 6 0 . 5 1 ± 3 1 . 0 8 0 . 0 0 0
[1]Schwarz S,Trivedi BK,Kalantar-Zadeh K,et al.Association of disorders in mineral metabolism with progression of chronickidneydisease[J].ClinAmSocNephrol,2006,1(4):825-831.
[2]AdeneyKL,Siscovick DS,IxJH,et al.Association ofserumphosphate with vascular and vascular calcification in moderate CKD[J].AmSoc Nephrol,2009,20(2):381-387.
[3]JfippnerH.PhosphateandFGF-23[J].KidneyIntSuppl,2011(121):24-27.
[4]Ferraro PM,Bonello M,Gambaro A,et al.Ageand sex tailored serum phosphate thresholds do not improve cardiovascular risk estimation in CKD[J].Nephrol,2011,24(4):446-452.
[5]AsaiO,Nakatani K,Tanaka T,et al.Decreased renal klotho expression in early diabetic nephropathy in humans and mice and its possible role in urinary calcium excretion[J]. KidneyInt,2012,81(6):539-547.
[6]Drion I,JoostenH,Dikkeschei LD,et al.eGFR and creatinine clearance in relation tometabolic changes in fin unselected patient population[J].Eur Intern Med,2009,20(7):722-727.
[7]Tervaert DY,Mooyaart AL,Amann K,et al.Pathologic classification ofdiabetic nephropathy[J].Am Soc Nephrol,2010,21(4):556-563.
Correlative Analysis of Glomerular Filtration Rate and Long-term Prognosis in Patients With Diabetic Nephropathy and Hyperphosphatemia
Qian Yong
(Xinyi People’s Hospital,Maoming 525300,China)
ObjectiveTo study the correlation between glomerular filtration rate and long-term prognosis in patients with hyperphosphatemia and diabetic nephropathy.MethodsCollected from March 2011 to September 2015,admitted during the period of 436 patients diagnosed with type 2 diabetes nephropathy patients as the research object,the patients clinical baseline information collection,to patients were followed for patients with hyperphosphatemia,incidence of blood phosphorus levels and renal damage degree of correlation,and blood phosphorus levels predicted value of the long-term prognosis in patients with diabetic nephropathy. ResultsHyperphosphatemia occurred in 24 of 109 patients,with an incidence of 22.0%.The incidence of hyperphosphatemia was 32.1%in patients with glomerular filtration rate<60mL/(min·1.73m2),and the incidence of hyperphosphatemia in patients with glomerular filtration rate of 60-90mL/(min·1.73m2)Was 16.7%.The incidence of hyperphosphatemia was 10.5%in glomerular filtration rate>90mL/(min·1.73m2).The incidence of hyperphosphatemia increased with decreasing glomerular filtration rate.With the decrease of glomerular filtration rate,the higher the serum phosphorus level,the higher the risk of end-stage renal disease.ConclusionDiabetic nephropathy patients with high incidence of hyperphosphatemia,hyperphosphatemia and significantly associated with the degree of the damage to the kidney at the same time,and is independent of terminal nephropathy in patients with risk factors,and to predict the long-term prognosis of patients with a certain value.
Hyperphosphatemia;Diabetic nephropathy;End-stage renal disease;CKD
R586.9
A学科分类代码:32024
1001-8131(2017)02-0112-03
2016-11-17