Exenatide promotes regeneration of injured rat sciatic nerve
2017-05-03ErsinKuyucuBilalOytunErbasFatihOltuluArslanBora
Ersin Kuyucu, Bilal Gümüs, Oytun Erbas, Fatih Oltulu, Arslan Bora
1 Department of Orthopedics and Traumatology, Faculty of Medicine, Istanbul Medipol University, Istanbul, Turkey
2 Orthopedics Clinic, Antalya State Hospital, Antalya, Turkey
3 Department of Physiology, Ege University Faculty of Medicine, Izmir, Turkey
4 Department of Histology Clinic, Ege University Faculty of Medicine, Izmir, Turkey
5 Department of Orthopedics and Traumatology, Izmir Atatürk Training and Educational Research Hospital, Izmir, Turkey
Exenatide promotes regeneration of injured rat sciatic nerve
Ersin Kuyucu1,*, Bilal Gümüs2, Oytun Erbas3, Fatih Oltulu4, Arslan Bora5
1 Department of Orthopedics and Traumatology, Faculty of Medicine, Istanbul Medipol University, Istanbul, Turkey
2 Orthopedics Clinic, Antalya State Hospital, Antalya, Turkey
3 Department of Physiology, Ege University Faculty of Medicine, Izmir, Turkey
4 Department of Histology Clinic, Ege University Faculty of Medicine, Izmir, Turkey
5 Department of Orthopedics and Traumatology, Izmir Atatürk Training and Educational Research Hospital, Izmir, Turkey
How to cite this article:Kuyucu E, Gümüs B, Erbas O, Oltulu F, Bora A (2017) Exenatide promotes regeneration of injured rat sciatic nerve. Neural Regen Res 12(4):637-643.
Open access statement:This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
Damage to peripheral nerves results in partial or complete dysfunction. Aer peripheral nerve injuries, a full functional recovery usually cannot be achieved despite the standard surgical repairs. Neurotrophic factors and growth factors stimulate axonal growth and support the viability of nerve cells.e objective of this study is to investigate the neurotrophic ef f ect of exenatide (glucagon like peptide-1 analog) in a rat sciatic nerve neurotmesis model. We injected 10 μg/d exenatide for 12 weeks in the experimental group (n= 12) and 0.1 mL/d saline for 12 weeks in the control group (n= 12). We evaluated nerve regeneration by conducting electrophysiological and motor functional tests. Histological changes were evaluated at weeks 1, 3, 6, and 9. Nerve regeneration was monitored using stereomicroscopy.e electrophysiological and motor functions in rats treated with exenatide were improved at 12 weeks aer surgery. Histological examination revealed a signif i cant increase in the number of axons in injured sciatic nerve following exenatide treatment conf i rmed by stereomicroscopy. In an experimentally induced neurotmesis model in rats, exenatide had a positive ef f ect on nerve regeneration evidenced by electromyography, functional motor tests, histological and stereomicroscopic fi ndings.
nerve regeneration; sciatic nerve; glucagon like peptid 1; electromyography; stereomicroscopy; histology; neural regeneration
Introduction
Peripheral nerves are the axonal extensions of the motor neurons of the anterior horn of the spinal cord, the sensory neurons of the dorsal ganglia, and the sympathetic neurons of the sympathetic ganglia (Shenaqand Kim, 2006; Winogradand Mackinnon, 2006). Damage to peripheral nerves results in partial or complete dysfunction. Aer peripheral nerve injuries, a full functional recovery usually cannot be achieved despite the standard surgical repairs (Brushart, 1998; Madison et al., 1999). Development of new technologies, widespread use of surgical microscope, use of tension-free and anatomically sutured nerve endings with epineural or perineural stitches, and discovery of the molecular mechanisms of nerve degeneration and regeneration processes all have led to more successful results in the fi eld of surgical nerve repair. However, there is still no treatment method for nerve damage that enables sensory and functional nerve recovery to the same level as before injury (Lundborg, 2000; Shenaq and Kim, 2006; Hsu and Stevenson, 2015; Tseng et al., 2015). Besides, permanent dysfunction of only one peripheral nerve, for example, ulnar nerve in the hand may lead to serious functional limitations.erefore, it is important to accelerate nerve regeneration aer injury.
Neurotropic factors and growth factors stimulate axonal growth and support the viability of nerve cells. Glucagon-like peptide (GLP-1) is a polypeptide hormone composed of 30 amino acids, which is secreted by the endocrine cells of the small intestine (Luo et al., 2016). GLP-1 receptors (GLP-1Rs) have been detected in the central and peripheral nervous systems; GLP-1 is thought to exert neurotropic ef f ects through these receptors (Shenaq and Kim, 2006). GLP-1 is also known as a potent incretin and its injections may cause a weight loss (Liu et al., 2011). GLP-1 is contraindicated in renal dysfunction and if the creatinine clearance less than 30 mL/min, its usage is not recommended.
Exendin-4 is the best GLP-1 analogue in nature. It is derived from the saliva of glia monster (Göke et al., 1993). Exenatide is the synthetic analogue of exendin-4, which is currently used subcutaneously in the treatment of type 2 diabetes and approved by Food and Drug Administration (FDA) (Buse et al., 2004; Gallwitz, 2005).
Recent studies with GLP-1 analogues documented both amelioration of central degenerative changes and prevention of peripheral nerve degeneration in diabetic rats (Seddonet al., 1943; Liu et al., 2011; Chen et al., 2012). Another recent study explored the effect of exendin-4 on peripheral nerve regeneration in rats with crush sciatic nerve injury.ey reported signif i cant changes in functional, electrophysiologicaland histological parameters in just 4 weeks aer use of exendin-4 (Liu et al., 2011). However, to the best of our knowledge, there are no previous studies investigating the ef f ects of currently used GLP-1 analogue, exenatide, on peripheral nerve regeneration.
A stereomicroscope produces a truly three-dimensional image which documents the regeneration process better. A stereomicroscope cannot magnify an image as much as a compound microscope, which allows seeing the hole tissue without any preparation. To the best of our knowledge, stereomicroscopic follow-up of neuronal tissue was not performed in former studies with GLP-1 analogues.
Materials and Methods
Ethics statement
Animals
We used male Sprague-Dawley rats aged 12–16 weeks and weighing 190–220 g.e animals were kept under standard experimental conditions (21–22°C, 55–65% humidity, 12-hour light/dark cycle).ey were fed commercial rat chow pellets and were allowed water and foodad libitum. These animals were randomly divided into an experimental group and a control group, with 12 rats in each group.
In the experimental group, following induction of sciatic nerve transaction injury, Exenatide (AstraZeneca, Wilmington, DE, USA) was injected subcutaneously from the back skin at 10 μg/d for 12 weeks. To detect the harmful ef f ects, we injected the maximum dose (10 μg/d) for human therapeutic usage (Buse et al., 2004; Gallwitz, 2005).
Surgical procedure
All rats were anesthetized by intraperitoneal administration of 50 mg/kg ketamine HCl (Alfamine, Egevet, Turkey) and 10 mg/kg xylazine (Alfazyne).e same orthopedic surgeon (EK) performed the same surgical procedure on the right and lehindlimbs in all rats in both groups using the same microsurgery equipment (Bahadır Medical Equipment Inc., Turkey). An oblique incision of 1 cm was made on the right thigh posteriorly with a No. 15 scalpel. Aer the blunt dissection of the biceps femoris muscle, the sciatic nerve was exposed and completely transected at the mid-thigh level with microsurgical scissors (Bahadır Medical Equipment Inc.). The dissected part of the biceps femoris muscle was sutured using 4/0 vicryl, and the skin was closed with 4/0 prolene.e procedure was terminated aer wound antisepsis with povidone-iodine solution. For the lehindlimb, the sciatic nerve was completely transected, forming a gap of 1 cm at the mid-thigh level.
Assessment methods
Weight, blood glucose level (at 0 hours or 3 hours aer exenatide administration), motor function, and electromyography (EMG) records were assessed separately in all rats at 1, 3, 6 and 9 weeks aer surgery. One rat was randomly selected from each group for stereomicroscopic evaluation, after which both of them were sacrificed for histological evaluation of the sciatic nerve. At 12 weeks, EMG records and motor strength tests were performed and all rats underwent stereomicroscopic evaluation.ereaer, rats were sacrif i ced and the sciatic nerves were evaluated histologically.
Evaluation of muscle strength of hindlimbs
Using the motor power measurement device (OE-Turkey) (Figure 1), the climbing angle, an indicator of the muscle strength of the hindlimbs, was measured. The rat was released onto the device when the angle was 0 degrees. The angle was gradually increased, and the last angle at which the rat was able to cling to the device was recorded.is procedure was repeated three times for each rat, and the highest value was recorded.
Electrophysiological evaluation
EMG was performed for each rat before and at 1, 3, 6, 9, and 12 weeks aer surgery. For electrophysiological measurements, a computer-aided, MP30, nerve conduction velocity measurement kit (Biopac Systems, Inc., Goleta, CA, USA) was used.e proximal pole was placed 10 mm distal to the sciatic notch while the distal pole was put in the second interdigital space. At 9 and 12 weeks after surgery, both the second interdigital space and the distal part of gastrosoleus muscle were used as the distal pole.e latency and the amplitude values of compound muscle action potential (CMAP) were recorded and statistically analyzed.
Stereomicroscopic evaluation of the sciatic nerve
Using the stereomicroscope (45× magnification) (SOIF ST6024-B1) and a video recorder (3.2× magnification) (MD30, İmage Transfer-China), video and photo recordings were taken at a magnif i cation of 7× and 120×, respectively.
Histological evaluation

Figure 1e muscle strength device used to measure the maximum degree at which the rat cannot roll from the device.

Figure 2 Stereomicroscopic observation of injured sciatic nerve in rats.
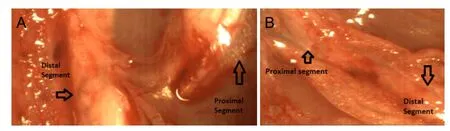
Figure 3 Stereomicroscopic observation of the right sciatic nerve transaction site of the experimental group at 3 weeks aer surgery.
Statistical analysis
Parametric variables were compared using one-way analysis of variance, whereas the values within the groups were compared using the parametric pairedt-test. AP-value < 0.05 was considered statistically signif i cant. Descriptive statistics are presented as the mean ± SD. All analyses were performed using SPSS 15.0 for Windows (SPSS, Chicago, IL, USA), with a conf i dence level of 95%.
Results
Body weight and blood glucose level
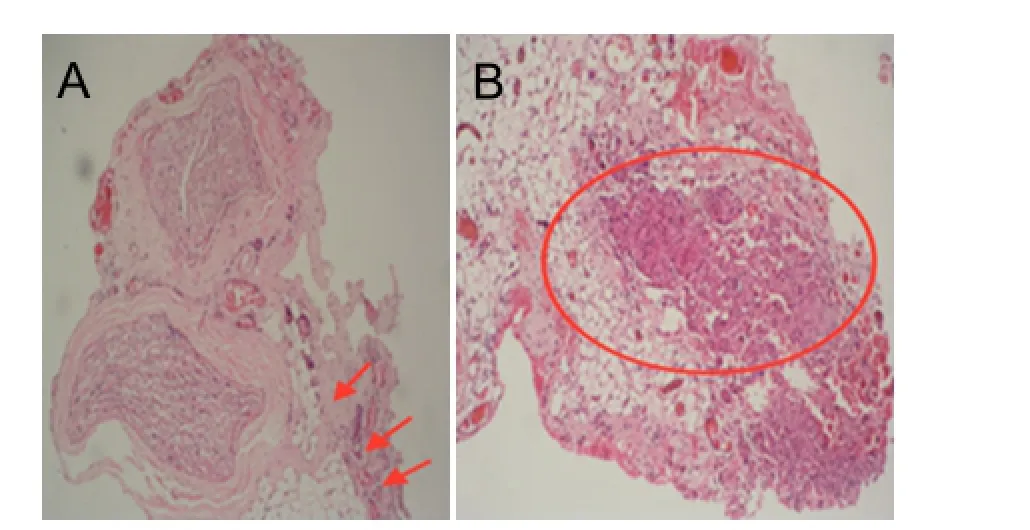
Figure 4 Histological evaluation of the right sciatic nerve by hematoxylin-eosin staining at 12 weeks aer surgery.
Muscle strength of hindlimbs
Electrophysiological function of the sciatic nerve
Before surgery, the sciatic nerves of rats in both groups were assessed bilaterally using EMG and all were intact. EMG results showed that there were no responses in the second interdigital space in the right and lehindlimbs in the experimental and control groups at 1, 3 and 6 weeks aer surgery. At 9 and 12 weeks aer surgery, there was no response in the second interdigital space in the right and left hindlimbs of rats in both groups. At 9 weeks aer surgery, there was nosignificant difference in latency of CMAP between experimental and control groups (P> 0.05), whereas the amplitude of CMAP of the right hindlimb was signif i cantly greater in the experimental group than in the control group (P< 0.01). There was no significant difference in terms of latency or amplitude of CMAP of the lehindlimb between these two groups (bothP> 0.05). At 12 weeks aer surgery, there was no EMG response from the distal part of the gastrosoleus muscle in either group.e amplitude and latency of CMAP of the proximal part of the gastrosoleus muscle in the left and right hindlimbs of rats in the experimental group were signif i cantly greater than in the control group (Table 3).
Table 1 Blood glucose level (mg/dL) at 0 or 3 hours aer administration
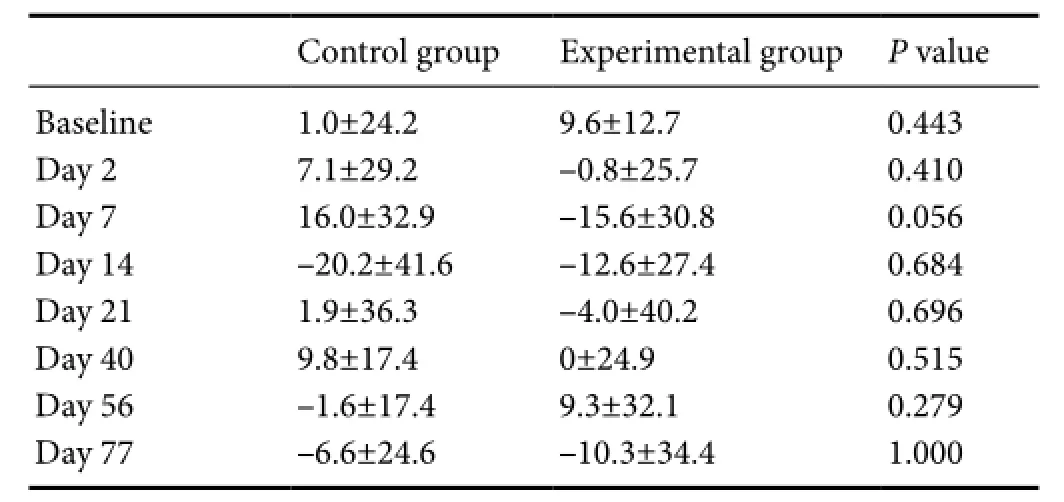
Table 1 Blood glucose level (mg/dL) at 0 or 3 hours aer administration
Data were expressed as the mean ± SD and analyzed using one-way analysis of variance.
Control group Experimental groupPvalue Baseline 1.0±24.2 9.6±12.7 0.443 Day 2 7.1±29.2 –0.8±25.7 0.410 Day 7 16.0±32.9 –15.6±30.8 0.056 Day 14 –20.2±41.6 –12.6±27.4 0.684 Day 21 1.9±36.3 –4.0±40.2 0.696 Day 40 9.8±17.4 0±24.9 0.515 Day 56 –1.6±17.4 9.3±32.1 0.279 Day 77 –6.6±24.6 –10.3±34.4 1.000
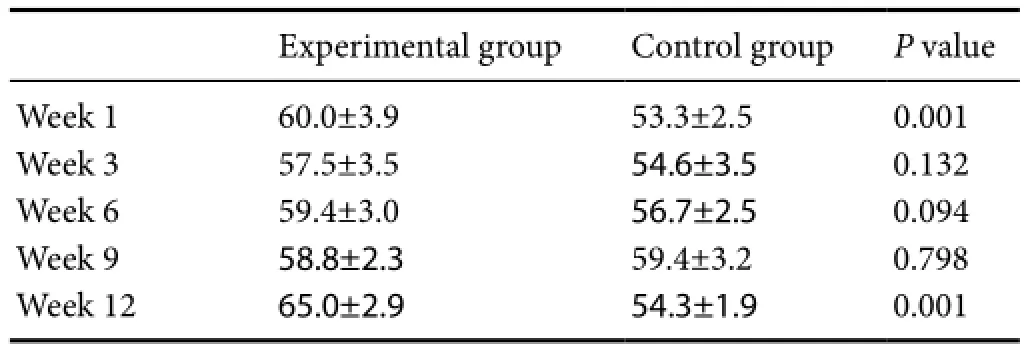
Table 2 Muscle strength of hindlimbs (angle (°)

Table 3 Electromyography results
Stereomicroscopic characteristics
1-week imaging
3-week imaging
In the images taken at 3 weeks, vascularization increased at the transection site, in particular in the proximal segment,which was more prominent in the experimental group. Nerve sprouting had started in the right sciatic nerves of both experimental and control groups, and the sprouting exhibited a wider area and a greater diameter in the experimental group than in the control group.ere was no obvious sprouting in the lesciatic nerve with a 1-cm gap. Moreover, in the distal segment of the lesciatic nerve, diameter and vascularity of the sprouting decreased due to degeneration (Figure 3).
Table 4 Quantitation of axon numbers in the leand right sciatic nerves by histological evaluation at 3 and 12 weeks aer surgery
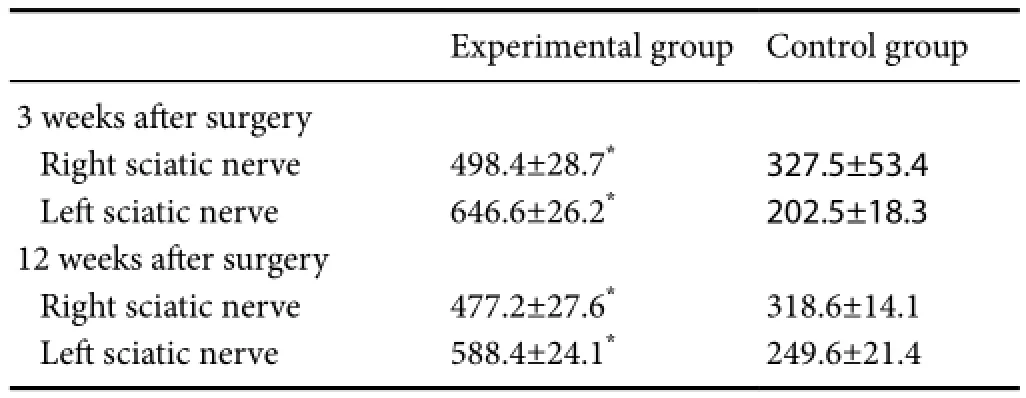
Table 4 Quantitation of axon numbers in the leand right sciatic nerves by histological evaluation at 3 and 12 weeks aer surgery
Data are expressed as the mean ± SD. *P< 0.05,vs. control group (oneway analysis of variance).
Experimental group Control group 3 weeks aer surgery Right sciatic nerve 498.4±28.7*327.5±53.4 Lesciatic nerve 646.6±26.2*202.5±18.3 12 weeks aer surgery Right sciatic nerve 477.2±27.6*318.6±14.1 Lesciatic nerve 588.4±24.1*249.6±21.4
9-week imaging
In the images taken at 9 weeks aer surgery, nerve sprouting greatly increased in both control and in particular experimental groups. A gel-like lining was maintained between the proximal and the distal poles of the transection site in the experiemntal group.e gel-like lining was less prominent in the right sciatic nerve in the control group and in the lesciatic nerve in the experimental group. Nerve sproting in the lesciatic nerve was observed in both the experimental and control groups. In the experimental group, although there was no integrity between the segments with sprouting, sprouting was more prominent.
12-week imaging
In the images taken at 12 weeks after surgery, in the right sciatic nerve, the vascularization of the segmental integrity provided by sprouting was increased compared to that at 9 weeks aer surgery, and more than 50% integration between distal and proximal poles was observed. There was nerve sprouting in the proximal segment of the lesciatic nerve, but no integration with the distal segment was observed. Inthe distal segment, diameter and vascularization reduced. However, there was no signif i cant difference in this respect between the experimental and control groups (Figure 2C, D).
Histological changes of the sciatic nerve
Discussion
Peripheral nerves are likely to be injured in many different ways, such as mechanical (compression, stretching, crushing), thermal, chemical, and ischemic injuries (Seddon, 1943).e main objective of treatment aer the injury is to achieve neuronal integrity and re-enable the nerve function and conduction.e purpose of this experimental study was to investigate the neurotropic effect of exenatide (a GLP-1 analogue) in a rat sciatic nerve injury model and to determine the electrophysiological, behavioral, hisotomorphological and stereomicroscopic changes. Our study showed that use of exenatide accelerated peripheral nerve regeneration from the electrophysiological, behavioral, hisotomorphological and stereomicroscopic viewpoints without affecting body weight and blood glucose level.
There is strong evidence that numerous peptides have been identified to have ef f ects on the viability and the regeneration capacity of the nerve tissue (Madison et al., 1999; Lundborg, 2000; Hsu and Stevenson, 2015).ese so-called neurotropic factors affect the different phases of nerve regeneration positively. Luo et al. (2016) investigated the role of insulin-like growth factor-1 in the treatment of tibial nerve injury in rat models.ey found that local insulin-like factor-1 administration reverses age-related declines in recovery and they might consider available adjuvant therapy to the current treatment modalities.
GLP-1 is an insulin tropic hormone secreted by the endocrine L cells of the human intestine post-prandial (Perry et al., 2007). By radioimmunoassay and immunohistochemical methods, immunoreactivity consistent with GLP-1 has been shown in human and rat brains, spinal oblongata, pons, and sciatic nerve. GLP-1 has anti-apoptotic properties in the hippocampal nucleus of (Avcı et al., 2002). Aer this discovery, the potential of GLP-1 to protect the central nervous system from the neurodegenerative damage has become a matter of interest (Luo et al., 2016).
Yamamoto et al. (2013) demonstrated in a rat sciatic nerve injury model that exendin-4 did not affect blood glucose levels. In this study, blood glucose level was measured in rats before and 3 hours after surgery. There was no significant difference in blood glucose level or hypoglycemia between the experimental and control groups.e use of an anti-diabetic drug in peripheral nerve injury in clinical practice may lead to hesitation because of side ef f ects including possible hypoglycemia and body weight loss. The neutral effect of exenatide on blood glucose levels compared to control group in our study is important and encouraging regarding drug safety (Ahmed et al., 1999).
Kaimal et al. (2012) observed in patients with type 2 diabetes mellitus that a GLP-1 analogue led to an average weight loss of 6.6 kg by reducing the rate of gastric emptying and due to its intestinal effects. Ohki et al. (2016) also reported weight reduction is a benef i t of treatment with GLP-1 analogues in diabetic patients. However, we observed weight gain in both groups, without a statistically significant difference between the groups.is is also another important safety indicator for clinical use in future. When exenatide is planned to use in patients with peripheral nerve injury, weight change is not a possible side ef f ect in the light of our results.
In experimental studies examining the peripheral nerve regeneration, both morphological and functional examinations are recommended (Luis et al., 2007).e best test to show the recovery after nerve injury, to the best of our knowledge, has not been clarified in experimental models. However, there are various evaluation parameters, such as gait analysis, EMG, climbing apparatus, histological evaluation, and foot withdrawal ref l ex (Rivli and Tator, 1977).
Electrophysiological tests are frequently used in the evaluation of peripheral nerve regeneration.ese tests are based on the magnif i cation of the action potentials in nerve fi bers caused by the stimulation of the muscle fi bers, using an amplif i er (Wolthers et al., 2005). In this study, we documented a statistically significant increase in the amplitude of right hindlimbs at 9 weeks and there were signif i cant differences in both amplitude and latency of CMAP of the leand right hindlimbs at 12 weeks between the experimental and control groups.
Wolters et al. (2005) demonstrated that as axonal regeneration increases and remyelination progresses, the synchronization and the amplitude increase due to the increased change and response in the fi bers. Baykal et al. (2002) reported that the time elapsed between the latency values and the start of contraction potentials is an important indicator of myelinization. In our study, EMG recordings at 9 weeks, in particular at 12 weeks, have shown that exenatide increased myelinization and total axonal synchronization in nerve regeneration, resulting in faster nerve regeneration.
To evaluate the motor function of rats in this study, the climbing angles were monitored and recorded at 0, 1, 3, 6, 9, and 12 weeks aer surgery (Fisher and Peduzzi, 2007; Luis et al., 2007).e climbing angle was signif i cantly greater in the experimental group at 1 and 12 weeks than in the control groups. Findings from a 12-week observation indicate that the sciatic function had recovered to a great extent. The data concerning functional evaluation indicates thatelectrophysiological changes in nerve regeneration can refl ect motor function capacity which is the most important endpoint regarding peripheral nerve injuries in daily clinical practice.
Results from this study revealed a faster degeneration in the distal pole of the nerve of neuromesis model with a 1-cm gap in the lesciatic nerve. At 12 weeks aer surgery, the proliferation was more irregular over a wide range, with a severe degeneration of the distal poles. In the right sciatic nerve, which was transected and showed regeneration, the healing was subjectively more rapid and regular, and the proliferation and the integrity between the distal and the proximal pole were achieved earlier, in rats treated with GLP-1 than in control rats. However, in the lesciatic nerve, there was no significant difference in the phase of regeneration between the experimental and control groups. Also in the lesciatic nerve, there was no signif i cant difference in stereological stereomicroscopic changes, which should be followed up for a longer time period.is study adds much to document the regenerative capacity of exenatide on tissue level according to these stereomicroscopic fi ndings. To the best of our knowledge, this is the fi rst study in literature which demonstrated the accelerated peripheral nerve regeneration aer use of exenatide on the tissue level. We documented better regeneration in an injured sciatic nerve in the absence of surgical repair. Much better healing is expected when exenatide is applied aer surgical repair because anatomical integrity will already be provided by surgery.
Luis et al. (2007) and Rizli and Tator (1977) also used a sciatic nerve model with a defect. They used hematoxylin-eosin staining to measure axon diameter, myelin thickness and nerve density to evaluate nerve regeneration. In this study, histological evaluation at 3 and 12 weeks revealed Wallerian axonal degeneration bilaterally in the sciatic nerve in both the experimental and control groups. However, the number of axons in the experimental group was greater than in the control group.e number of newly formed axons was also increased significantly in the experimental group than in the control group both on the right and the lesciatic nerves at 12 weeks. In this study, we investigated the ef f ects of 10 μg/d exenatide on sciatic nerve injury in rat models. Future research is needed to investigate the ef f ects of exenatide at different doses. Another limitation of this study is the follow-up period and another incretin mimetic drug will be added as a control group. Further studies with longer follow-up periods are required to demonstrate the efficacy of exenatide in severe nerve injury.
In conclusion, in an experimentally induced neurotmesis model in rats, GLP-1 had a positive ef f ect on nerve regeneration as evidenced by EMG, stereomicroscopic and histological fi ndings and motor functional tests.e drug seems to have no ef f ects on body weight and blood glucose levels.e absence of auto-cannibalization in the experimental group implies that exenatide accelerates the healing of sensory symptoms and helps to reduce pain.ese fi ndings have important implications for use of exenatide in the treatment of peripheral nerve injury in future.
Author contributions:EK and AB conceived the study. EK performed surgeries, measured blood glucose level, and took stereomicroscope images. BG performed electromyography and motor function tests and wrote the paper. OE participated in electromyography and physiological tests. FO carried out histological evaluation. All authors approved the f i nal version of this paper.
Conficts of interest:None declared.
Plagiarism check:This paper was screened twice using CrossCheck to verify originality before publication.
Peer review:This paper was double-blinded and stringently reviewed by international expert reviewers.
Ahmed Z, Brown RA, Ljungberg C, Wiberg M, Terenghi G (1999) Nerve growth factor enhances peripheral nerve regeneration in non-human primates. Scand J Plast Reconstr Surg Hand Surg 33:393-401.
Avcı G, Akan M, Yıldırım S, Aköz T (2002) Nerve repair and graing (review of the literature). T Klin Tıp Bilimleri 22:428-437.
Baykal S, Boz C, Çakır E, Baytan ŞH, Karakuş M, Kuzeyli K (2002)e ef f ects of pentoxifylline in experimental nerve injury, Turk J Med Sci 32:207-210.
Brushart TM (1998) Nevre repair and graing. In: Operative Hand Surgery. 4thed (Green DP). Churchill Livingstone Inc.
Buse JB, Henry RR, Han J, Kim DD, Fineman MS, Baron AD; Exenatide-113 Clinical Study Group (2004) Ef f ects of exenatide (exendin-4) on glycemic control over 30 weeks in sulfonylurea-treated patients with type 2 diabetes. Diabetes Care 27:2628-2635.
Chen S, Liu AR, An FM, YaoWB, Gao XD (2012) Amelioration of neurodegenerative changes incellular and rat model of diabetes-related Alzheimer’s disease by exendin-4. Age (Dordr)34:1211-1224.
Fisher PD, Peduzzi JD (2007) Functional recovery in rats with chronic spinal cord injuries aer exposure to an enriched environment. J S Cord Med 30:147-155.
Gallwitz B (2005) Glucagon-like peptide-1-based therapies for the treatment of type 2 diabetes mellitus. Treat Endocrinol 4:361-370.
Göke R, Fehmann HC, Linn T, Schmidt H, Krause M, Eng J, Göke B (1993) Exendin-4 is a high potency agonist and truncated exendin-(9-39)-amide an antagonist at the glucagon-like peptide 1-(7-36)-amide receptor of insulin-secreting beta-cells. J Biol Chem 268:19650-19655.
Hsu M, Stevenson FF (2015) Wallerian degeneration and recovery of motor nerves after multiple focused cold therapies. Muscle Nerve 51:268-275.
Kaimal N, Schof i eld J, Zaki A, Patel R, Sharma M, McCourt E, Imtiaz KE (2012) Ef f ects of exenatide in poorly controlled type 2 diabetes. QJM 105:321-326.
Liu WJ, Jin HY, Lee KA, Xie SH, Baek HS, Park TS (2011) Neuroprotective ef f ect of the glucagon-like peptide-1 receptor agonist, synthetic exendin-4, in streptozotocin-induced diabetic rats. Br J Pharmacol 164:1410-1420.
Luís AL, Amado S, Geuna S, Rodrigues JM, Simões MJ, Santos JD, Fregnan F, Raimondo S, Veloso AP, Ferreira AJ, Armada-da-Silva PA, Varejão AS, Maurício AC (2007) Long-term functional and morphological assessment of a standardized rat sciatic nerve crush injury with a non-serrated clamp. J Neurosci Methods 163:92-104.
Lundborg G (2000) A 25-year perspective of peripheral nerve surgery: evolving neuroscientific concepts and clinical significance. J Hand Surg Am 25:391-414.
Luo TD, Alton TB, Apel PJ, Cai J, Barnwell JC, Sonntag WE, Smith TL, Li Z (2016) Ef f ects of age and insulin-like growth factor-1 on rat neurotrophin receptor expression aer nerve injury. Muscle Nerve 54:769-775.
Madison RD, Archibald SJ, Lacin R, Krarup C (1999) Factors contributing to preferential motor reinnervation in the primate peripheral nervous system. J Neurosci 19:11007-11016.
Martins RS, Siqueira MG, da Silva CF, Plese JP (2006) Correlation between parameters of electrophysiological, histomorphometric and sciatic functional index evaluations aer rat sciatic nerve repair. Arq Neuropsiquiatr 64(3B):750-756.
Ohki T, Isogawa A, Toda N, Tagawa K (2016) E ff ectiveness of ipraglifl ozin, a sodium-glucose co-transporter 2 inhibitor, as a second-line treatment for non-alcoholic fatty liver disease patients with type 2 diabetes mellitus who do not respond to incretin-based therapies including glucagon-like peptide-1 analogs and dipeptidyl peptidase-4 inhibitors. Clin Drug Investig 36:313-319.
Perry T, Holloway HW, Weerasuriya A, Mouton PR, Duf f y K, Mattison JA, Greig NH (2007) Evidence of GLP-1-mediated neuroprotection in an animal model of pyridoxine-induced peripheral sensory neuropathy. Exp Neurol 203:293-301.
Rivli AS, Tator CH (1977) Objective clinical assessment of motor function after experimental spinal cord injury in the rat. J Neurosurg 47:577-581.
Seddon HJ, Medawar PB, Smith H (1943) Rate of regeneration of peripheral nerves in man. J Physiol 102:191-215.
Shenaq SM, Kim JY (2006) Repair and graing of peripheral nerve. In: Plastic surgery. 2nded (Mathes SJ, ed). Philadelphia: Saunders Elsevier.
Tseng TJ, Hsiao TH, Hsieh ST, Hsieh YL (2015) Determinants of nerve conduction recovery aer nerve injuries: Compression duration and nerve fi ber types. Muscle Nerve 52:107-112.
Winograd JM, Mackinnon SE (2006) Peripheral nevre injuries: Repair and reconstruction. In: Plastic surgery. 2nded (Mathes SJ, ed). Philadelphia: Saunders Elsevier.
Wolthers M, Moldovan M, BinderupT, Schmalbruch H, Krarup C (2005).Comparative electrophysiological functional and histological studies of nevre lesions in rats. Microsurgery 25:508-519.
Yamamoto K, Amako M, Yamamoto Y, Tsuchihara T, Nukada H, Yoshihara Y, Arino H, Fujita M, Uenoyama M, Tachibana S, Nemoto K (2013) Therapeutic effect of exendin-4, a long-acting analogue of glucagon-like peptide-1 receptor agonist, on nerve regeneration aer the crush nerve injury. Biomed Res Int 2013:315848.
Copyedited by Li CH, Song LP, Zhao M
*< class="emphasis_italic">Correspondence to: Ersin Kuyucu, M.D., ersinkuyucu@yahoo.com.tr.
Ersin Kuyucu, M.D., ersinkuyucu@yahoo.com.tr.
orcid: 0000-0003-3976-9530 (Ersin Kuyucu)
10.4103/1673-5374.205105
Accepted: 2017-03-27
杂志排行

中国神经再生研究(英文版)的其它文章
- Recovery of multiply injured ascending reticular activating systems in a stroke patient
- Neuroprotective mechanism of Kai Xin San: upregulation of hippocampal insulin-degrading enzyme protein expression and acceleration of amyloid-beta degradation
- Mitomycin C induces apoptosis in human epidural scar fi broblasts after surgical decompression for spinal cord injury
- Recombinant human fi broblast growth factor-2 promotes nerve regeneration and functional recovery after mental nerve crush injury
- Ca2+involvement in activation of extracellular-signalregulated-kinase 1/2 and m-calpain after axotomy of the sciatic nerve
- Low frequency repetitive transcranial magnetic stimulation improves motor dysfunction after cerebral infarction