术后化疗对早期肺大细胞神经内分泌肿瘤患者生存期的影响
2017-04-19韩轲范力文赵珩
韩轲 范力文 赵珩
术后化疗对早期肺大细胞神经内分泌肿瘤患者生存期的影响
韩轲①②范力文①赵珩①
目的:探讨术后化疗对早期肺大细胞神经内分泌肿瘤(large cell neuroendocrine carcinoma,LCNEC)患者生存期的影响。方法:回顾性分析2008年1月至2014年12月在上海交通大学附属胸科医院50例行肺癌根治性切除及系统性淋巴结清扫LCNEC患者的临床资料,根据术后是否接受化疗将50例患者分为化疗组(n=32)和非化疗组(n=18)。随访其生存状况。结果:化疗组和非化疗组中位生存时间分别为48个月和29个月,5年总生存率分别为72.5%和35.6%。单因素及多因素Cox分析均表明:术后辅助化疗为LCNEC患者OS的预后影响因素(P=0.005;HR=0.281,P=0.008)。结论:术后化疗可提高早期LCNEC术后患者的远期生存率。
肺大细胞神经内分泌肿瘤 外科手术 术后化疗 总生存期
根据2015年世界卫生组织(WHO)最新分类,肺神经内分泌肿瘤包括:典型类癌、非典型类癌、大细胞神经内分泌肿瘤(large cell neuroendocrine carcino⁃ma,LCNEC)和小细胞肺癌,其中LCNEC和小细胞癌同属于高级别神经内分泌肿瘤,具有相似的临床和生物学特征[1]。关于小细胞肺癌的诊断与治疗,临床上均有较多报道,然而对于LCNEC的报道都因病例数较少,而LCNEC患者的最优治疗方案和生存因素并没有得到很好的阐述,本研究对上海交通大学附属胸科医院收治的50例经早期LCNEC术后患者进行了回顾性分析。
1 材料与方法
1.1 病例资料
2008年1月至2014年12月间上海交通大学附属胸科医院共对104例LCNEC患者行外科手术治疗。依照2015年WHO最新的肺癌诊断及分类标准[1],回顾性分析其中50例LCNEC早期术后患者(其中Ⅰ期36例,Ⅱ期14例),围手术期死亡0例(术后30 d内死亡)。所有患者均经过全面的术前检查,排除远处转移,具有潜在的手术可切除性。局部显微镜下肿瘤残留、楔形切除、淋巴结采样及不完全手术切除的患者均排除在外。
1.2 方法
1.2.1 术前准备 纳入研究的患者均经过全面的术前检查并排除远处转移,其中包括胸部和颅脑CT、腹腔彩超(肝胆脾、肾上腺)、骨扫描、行气管镜活检;对于纵隔淋巴结肿大超过1 cm者,常规进行经颈部纵隔镜检查、支气管内超声引导针吸活检术(endobron⁃chial ultra-sound guided transbronchial needle aspira⁃tion,EBUS-TBNA)或正电子发射计算机断层扫描(positron emission computed tomography,PET-CT)检查。同时,依据国际抗癌协会的诊断标准[2]进行TNM分期。收集的临床数据包括性别、年龄、吸烟史、体力状况、肿瘤位置(中叶型/周围型)、术后辅助化疗。本研究经过被研究对象或其家属知情同意并得到医院伦理委员会批准。
1.2.2 随访 从术后开始随访至2016年6月30日,随访期2~100个月,平均随访期为45个月。截至2016年6月30日,共健在32例,死亡18例。
1.2.3 分组 50例患者分为2组,术后4周内开始辅助化疗,按时完成4个疗程以上为化疗组(n=32);未进行术后化疗和未完成术后辅助化疗为非化疗组(n=18),分析患者性别、年龄、吸烟史、体力状况、肿瘤位置(中叶型/周围型)、病理分期(TNM)对总生存期(overall survival,OS)的影响。
1.3 统计学分析
采用SPSS 19.0软件进行统计学分析。以每3个月为时间点,计算患者生存情况,判断两组5年生存率是否差异具有统计学意义。计数资料采用例数(构成比)进行描述,两组之间构成比的比较采用χ2检验,不满足χ2检验的条件,采用确切概率。OS定义为患者手术时间至最后一次随诊或死亡的时间。采用Kaplan-Meier法进行生存分析,不同组别间生存比较采用Log-rank检验,采用Cox模型进行预后多因素分析。以P<0.05为差异具有统计学意义。
2 结果
2.1 患者的临床特征及治疗方法
纳入研究的50例LCNEC患者,年龄36~79岁,平均为63.2岁;包括7例(14%)中央型和43例(86%)周围型。其中,11例患者行术前活检,大多为非特异性细胞类型,其中包括非小细胞肺癌(non-small cell lung cancer,NSCLC)3例(27.3%),LCNEC 2例(18.2%),非典型内癌2例(18.2%),低分化癌1例(9.1%),3例(27.3%)活检标本表现为坏死组织。
上述患者中,采用常规开胸手术患者为15例(30%),电视胸腔镜(video-assisted thoracic surgery,VATS)手术35例(70%),平均淋巴结清扫数16(10~22)枚。
50例患者中,32例患者接受术后辅助化疗,采用以铂类为基础的化疗方案,均完成4个或以上疗程辅助化疗,其中21例采用小细胞化疗方案(依托泊甙/顺铂);11例采用NSCLC化疗方案,其中(吉西他滨4例、长春瑞宾3例、培美曲塞2例、紫杉醇2例)。32例辅助化疗患者中,ⅠA期5例(10%),ⅠB期16例(32%),ⅡA期2例(4%),ⅡB期9例(18%)。18例未接受术后化疗的患者中,ⅠA期4例(8%),ⅠB期11例(22%),ⅡA期0例,ⅡB期3例(6%)。
两组患者的年龄、性别、吸烟史、肿瘤大小、TNM分期、体力状况评分(KPS)等临床资料基本均衡(表1)。
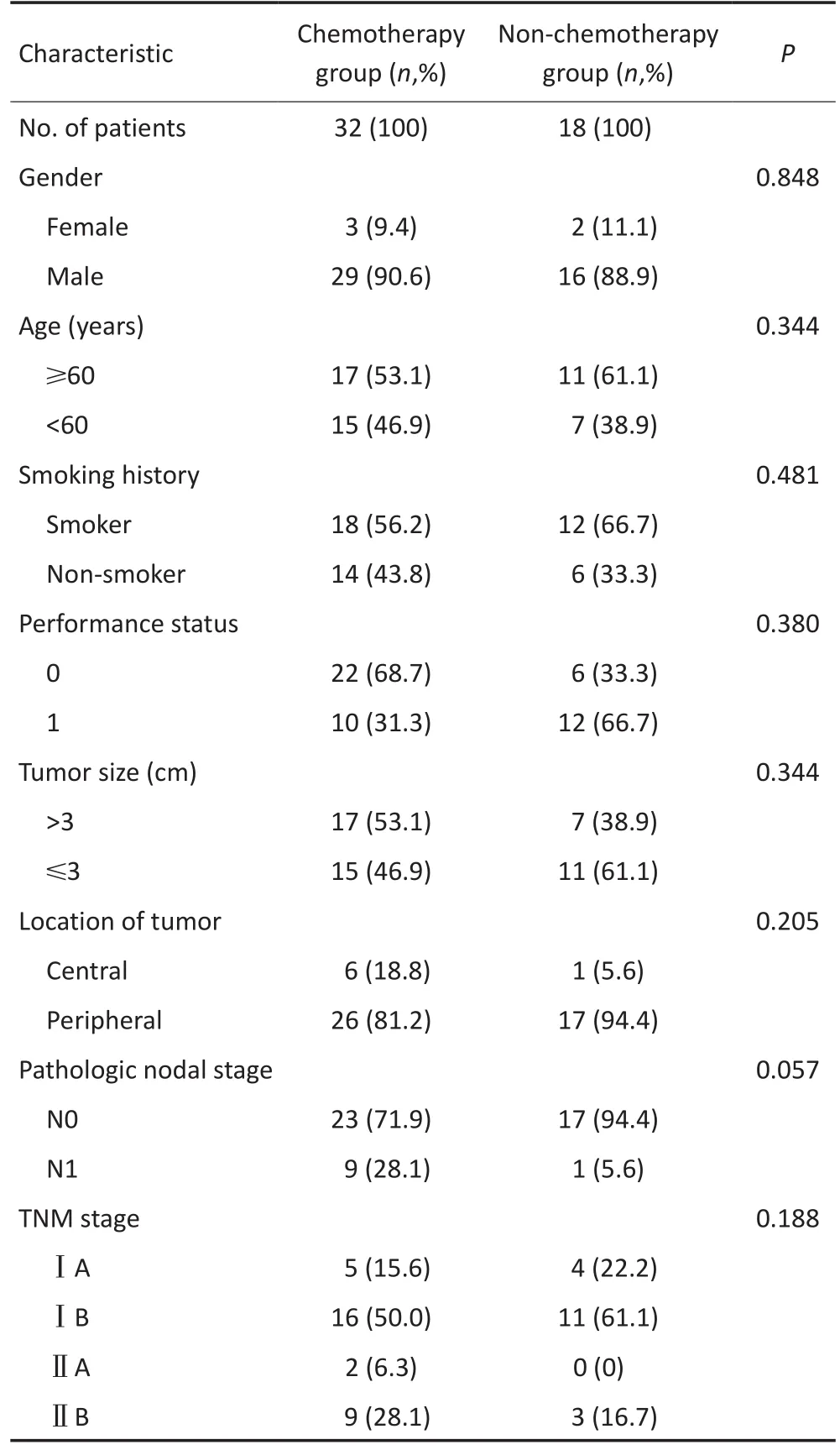
表1 基本病例资料特征Table 1 Baseline characteristics of all patients
2.2 远期疗效
单因素分析:本组患者的中位随访时间为45(2~100)个月,截止至最后一次随访,18例(36%)患者死亡,21例患者局部区域复发和远处转移,5年总生存率为60.1%。化疗组和非化疗组中位生存时间分别为48(12~100)个月和29(2~85)个月,5年生存率分别为72.5%和35.6%(图1)。单因素分析表明:术后辅助化疗为OS的独立影响因素(P=0.005,表2)。
多因素Cox分析表明:术后辅助化疗同样为OS独立的预后影响因素(HR=0.281,P=0.008,表3)。
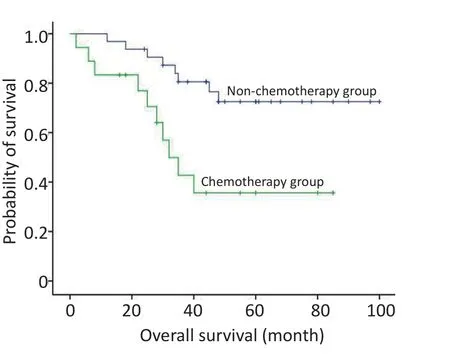
图1 化疗组与非化疗组生存率比较Figure 1 Overall survival according to different treatment group:chemotherapy and non-chemotherapy
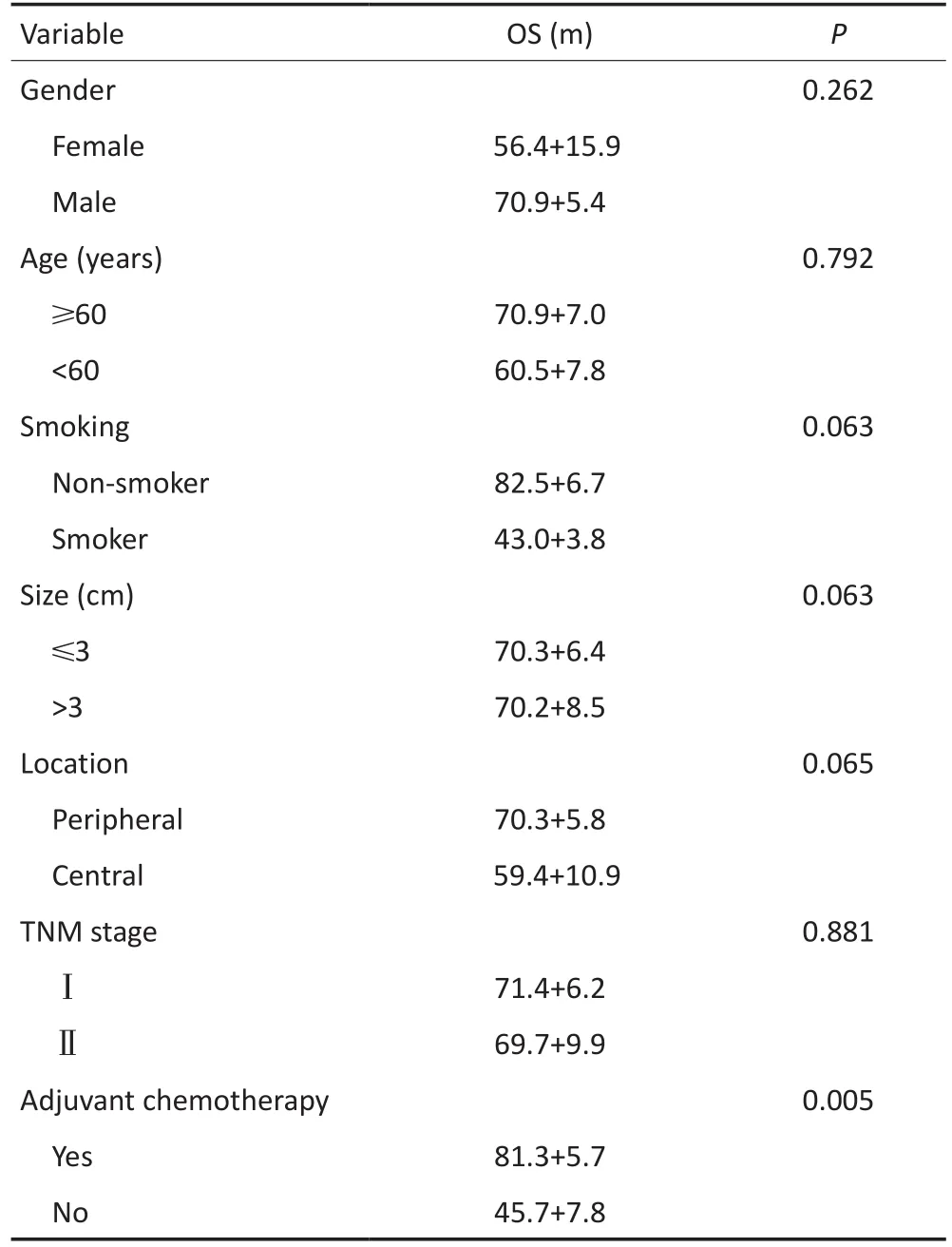
Variable Gender Female Male Age(years)≥60<60 Smoking Non-smoker Smoker Size(cm)≤3>3 Location Peripheral Central TNM stage OS(m)P 0.262 56.4+15.9 70.9+5.4 0.792 70.9+7.0 60.5+7.8 0.063 82.5+6.7 43.0+3.8 0.063 70.3+6.4 70.2+8.5 0.065 70.3+5.8 59.4+10.9 0.881ⅠⅡ71.4+6.2 69.7+9.9 Adjuvant chemotherapy Yes No 0.005 81.3+5.7 45.7+7.8
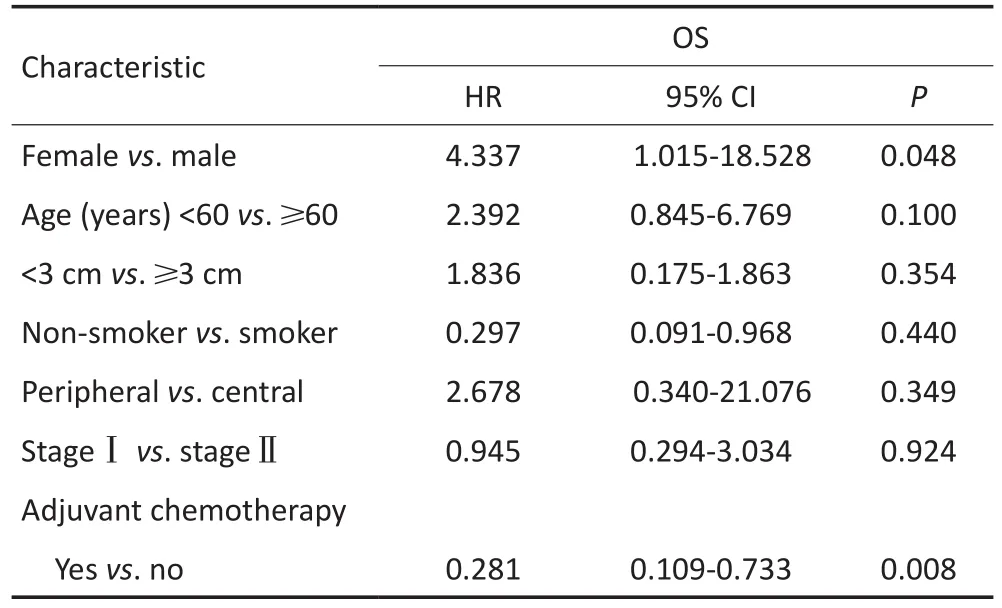
表3 多变量分析Table 3 Multivariable analysis
3 讨论
LCNEC是一类较为少见的肺部恶性肿瘤,报道其发生率约占可切除肺部肿瘤的3%[3-4],本研究LCNEC的发生率为0.6%。LCNEC同时也是恶性程度较高的肿瘤,据以往的文献报道,LCNEC患者的5年总生存率约为13%~57%[5-7],远低于大细胞癌和NSCLC。即使是Ⅰ期LCNEC患者,预后也相对较差,据报道5年总生存率约为27%~67%[8-12]。因此,单纯手术不足以提高LCNEC患者的预后。
术后辅助化疗在小细胞肺癌中的疗效已经得到一致的认可[13],但应用于LCNEC仍颇有争议。Tana⁃ka等[11]和Iyoda等[14]及其研究团队分别于2005年和2006年报道了对LCNEC术后患者行辅助化疗(依托泊甙/顺铂),均取得较为理想的结果。Fournel等[15]对Ⅰ期LCNEC术后部分患者行辅助化疗,化疗组同非化疗组相比,均取得相对较好的预后结果。本研究对LCNEC早期术后患者(Ⅰ+Ⅱ期)应用以铂类为基础的辅助化疗,化疗组和非化疗组中位生存时间分别为48(12~100)个月和29(2~85)个月,5年生存率分别为72.5%和35.6%。单因素及多因素Cox分析均表明:术后辅助化疗的LCNEC患者OS的预后影响因素为(P=0.005,HR=0.281,P=0.008),本研究术后化疗组5年生存率达到72.5%,较之前的报道有所增加,其原因可归结为两点:1)以铂类为基础化疗药物的应用;2)本研究收集的研究对象均行肺癌根治性切除+系统淋巴结清扫(不同于其他研究报道[16],部分患者行局部切除+淋巴结采样,而非标准的肺叶切除+系统淋巴结清扫术)。
本研究同其他研究相比,同样存在一定的局限性。首先,病例数相对较少,其原因主要归结为LCNEC同其他类型的肺部恶性肿瘤相比,其发病率较低,本研究团队将会继续收集更多的病例以便进一步研究;其次,未接受术后辅助化疗的患者同化疗组患者相比,大多身体状况相对较差,也可能是影响其远期预后的因素之一;最后,回顾性研究内在的选择偏倚性可能对研究结果产生一定的影响。
综上所述,尽管LCNEC是一类少见且恶性程度较高的肺部恶性肿瘤,本研究提示以铂类为基础的辅助化疗可以提高早期(Ⅰ+Ⅱ期)LCNEC患者术后的远期生存率,关于具体的化疗方案,是采用以小细胞化疗方案还是NSCLC化疗方案,将在今后的研究中进一步予以证实。
[1]Travis WD,Brambilla E,Nicholson AG,et al.The 2015 world health organization classification of lung tumors[J].J Thorac Oncol,2015, 10(9):1243-1260.
[2]Goldstraw P,Crowley J,Chansky K,et al.The IASLC lung cancer staging project:proposals for the revision of the TNM stage groupings in the forthcoming(seventh)edition of the TNM classif i cation of malignant tumours[J].J Thorac Oncol,2007,2(8):706-714.
[3]Paci M,Cavazza A,Annessi V,et al.Large cell neuroendocrine carcinoma of the lung:a 10-year clinic pathologic retrospective study [J].Ann Thorac Surg,2004,77(4):1163-1167.
[4]Le Treut J,Sault MC,Lena H,et al.Multicentre phaseⅡstudy of cisplatin-etoposide chemotherapy for advanced large-cell neuroendocrine lung carcinoma:the GFPC 0302 study[J].Ann Oncol,2013, 24(4):1548-1552.
[5]Iyoda A,Hiroshima K,Nakatani Y,et al.Pulmonary large cell neuroendocrine carcinoma:its place in the spectrum of pulmonary carcinoma[J].Ann Thorac Surg,2007,84(2):702-707.
[6]Asamura H,Kameya T,Matsuno Y,et al.Neuroendocrine neoplasms of the lung:a prognostic spectrum[J].J Clin Oncol,2006,24 (1):70-76.
[7]Rossi G,Cavazza A,Marchioni A,et al.Role of chemotherapy and the receptor tyrosine kinases KIT,PDGFR alpha,PDGFR beta,and Met in large-cell neuroendocrine carcinoma of the lung[J].J Clin Oncol,2005,23(34):8774-8785.
[8]Niho S,Kenmotsu H,Sekine I,et al.Combination chemotherapy with irinotecan and cisplatin for large-cell neuroendocrine carcinoma of the lung:a multicenter phaseⅡ study[J].J Thorac Oncol, 2013,8(7):980-984.
[9]Veronesi G,Morandi U,Alloisio M,et al.Large cell neuroendocrine carcinoma of the lung:a retrospective analysis of 144 surgical cases [J].Lung Cancer,2006,53(1):111-115.
[10]Ose N,Inoue M,Morii E,et al.Multimodality therapy for large cell neuroendocrine carcinoma of the thymus[J].Ann Thorac Surg, 2013,96(4):e85-87.
[11]Tanaka Y,Ogawa H,Uchino K,et al.Immunohistochemical studies of pulmonary large cell neuroendocrine carcinoma:a possible association between staining patterns with neuroendocrine markers and tumor response to chemotherapy[J].J Thorac Cardiovasc Surg, 2013,145(3):839-846.
[12]Battafarano RJ,Fernandez FG,Ritter J,et al.Large cell neuroendocrine carcinoma:an aggressive form of non-small cell lung cancer [J].J Thorac Cardiovasc Surg,2005,130(1):166-172.
[13]Liao ML.Lung Tumor[M].Shanghai:Shanghai Sci Tech Publishers, 2008:450.[廖美琳.肺部肿瘤学[M].上海:上海科学技术出版社, 2008:450.]
[14]Iyoda A,Hiroshima K,Moriya Y,et al.Prospective study of adjuvant chemotherapy for pulmonary large cell neuroendocrine carcinoma [J].Ann Thorac Surg,2006,82(5):1802.
[15]Fournel L,Falcoz PE,Alifano M,et al.Surgical management of pulmonary large cell neuroendocrine carcinomas:a 10-year experience[J].Eur J Cardiothorac Surg,2013,43(1):111-114.
[16]Okada M,Koike T,Higashiyama M,et al.Radical sublobar resection for small-sized non-small cell lung cancer:a multicenter study[J].J Thorac Cardiovasc Surg,2006,132(4):769-775.
(2016-11-07收稿)
(2017-01-01修回)
(编辑:杨红欣 校对:孙喜佳)
Role of postoperative chemotherapy in patients with early-stage pulmonary large-cell neuroendocrine carcinoma after resection
Ke HAN1,2,Liwen FAN1,Heng ZHAO1
Heng ZHAO;E-mail:h_zhao28@163.com
1Department of Thoracic Surgery,Shanghai Chest Hospital,Shanghai Jiao Tong University,Shanghai 200030,China;2Department of Thoracic Surgery,Shiyan People's Hospital,Shiyan 442000,China
Objective:To investigate the efficacy of postoperative chemotherapy in patients with early-stage pulmonary large cell neuroendocrine carcinoma(LCNEC)after resection.Methods:A cohort of 50 patients who underwent resection and systematic nodal dissection for LCNEC between January 2008 and December 2014 in our institution was retrospectively reviewed.The patients were divided into adjuvant chemotherapy group(32 cases)and non-chemotherapy group(18 cases).Follow-up information was investigated.Results:The median survival and the 5-year survival rate were 48 months and 72.5%for the adjuvant chemotherapy group whereas 29 months and 35.6%for the non-adjuvant chemotherapy group,respectively.Univariate and multivariate analyses using Cox's proportional hazard models showed that postoperative chemotherapy was a signif i cant prognostic factor for OS(P=0.005;hazard ratio=0.281,P=0.008,respectively).Conclusion: Postoperative chemotherapy is beneficial to patients with early-stage pulmonary LCNEC after complete resection.
large-cell neuroendocrine carcinoma,surgery,postoperative chemotherapy,overall survival
10.3969/j.issn.1000-8179.2017.04.286

①上海交通大学附属胸科医院胸外科(上海市200030);②湖北省十堰市人民医院胸外科
赵珩 h_zhao28@163.com
韩轲 专业方向为肺癌的诊断与治疗。
E-mail:15800558126@163.com
