单纯前降支病变患者再血管化治疗策略及进展
2017-04-11李双磊综述高长青审校
李双磊(综述),高长青(审校)
·综 述·
单纯前降支病变患者再血管化治疗策略及进展
李双磊(综述),高长青(审校)
前降支病变;再血管化;药物洗脱支架;冠状动脉旁路移植术;机器人
冠状动脉粥样硬化性心脏病(coronary artery disease,CAD)是威胁人类健康的主要疾病之一,据2015中国心血管病报告显示:2014年中国CAD死亡率城市为107.5/10万,农村为105.37/10万。
CAD患者中,50%以上的患者存在多支冠脉病变(两支主要冠状动脉狭窄>70%),约40%以上的患者为单系统病变[1]。前降支作为三支冠脉系统中最重要的一支,占心脏50%以上的供血,病变时临床症状重,单纯药物治疗5年死亡率为90%~98%,故再血管化风险较高[2]。近年,对于多支冠脉病变患者再血管化策略及疗效的研究较多,而对于单纯前降支(isolated left anterior descending,iLAD)病变的再血管化治疗的研究较少。
1 再血管化治疗策略
冠状动脉再血管化的治疗主要包括冠状动脉旁路移植术(coronary artery bypass grafting,CABG)及经皮冠状动脉支架植入术(percutaneous coronary intervention,PCI)。自上世纪60年代 Favaloro创建CABG术式以来,CABG术式及技术不断更新,由传统的体外循环下 CABG(cardiopulmonary bypass-CABG,C-CABG)手术到非体外循环下CABG(offpump CABG,OPCABG)手术,再到小切口CABG,直到今天的全内镜下机器人CABG手术,CABG技术有了巨大的进步。与此同时,PCI技术亦在快速发展,由裸金属支架(baremetal stents,BMS)到技术已非常成熟的药物洗脱支架(drug eluting stent,DES),再到现在正在论证的生物降解支架,PCI已成为大多数CAD患者再血管化的首选治疗手段。
1.1 CABG
1.1.1 C-CABG C-CABG采用正中开胸,游离带蒂乳内动脉,建立体外循环后阻断升主动脉,在心脏停跳下完成乳内动脉至LAD的吻合,吻合完毕后,心脏复跳。早在上世纪九十年代,一组随机对照试验(randomized controlled trial,RCT)研究已证实,对于iLAD患者,以乳内动脉(internal thoracic artery,ITA)行CABG,不仅在症状缓解上疗效显著,且在免于心血管事件发生率方面优于经皮冠状动脉成形术(percutaneous transluminal coronary angioplasty,PTCA)或口服药物治疗[3]。因此直至今天,C-CABG仍然是CABG的主流术式之一。
1.1.2 OPCABG OPCABG采用正中开胸,游离带蒂乳内动脉,在心脏跳动下,利用心表固定器固定LAD吻合口处,行ITA至LAD吻合。MASSⅢ试验证实,与C-CABG相比,OPCABG在远期生存率、桥血管远期通畅率及心血管事件发生率等方面无显著差异[4],但其减少了体外循环带来的炎症反应及机体损伤[5],同时OPCABG在减少住院天数、减少输血量、减少神经系统症状方面优于C-CABG[6]。但OPCABG较C-CABG而言,对外科医师的水平要求较高[7]。
1.1.3 小切口冠状动脉旁路移植术(minimally invasive direct coronary artery bypass,MIDCAB) MIDCAB主要包括胸部前外侧切口及胸骨上段切口两种。前者为胸骨左缘第四肋间行长约10 cm的切口,向上游离LAD至2~3肋间,向下至6~7肋间,而后在心脏跳动下应用搭桥稳定器完成ITA至LAD吻合。后者在胸骨劈开时行自胸骨上窝至第3肋软骨的倒L形切口,游离LAD后,利用搭桥稳定器在心脏跳动下行ITA至LAD吻合。目前MIDCAB已证实具有较高的安全性和有效性,与OPCABG相比,MIDCAB损伤小、恢复快,且具有较好的美容效果[8]。
1.1.4 机器人辅助下CABG(Endo-A-CAB) Endo-A-CAB采用da Vinci System,经左侧胸壁3、5、7肋间打孔,内镜下骨骼化游离ITA,游离完毕后采用两种路径行ITA至LAD吻合:①内镜定位下在左胸前外侧4或5肋间行4~6 cm切口,暴露LAD后进行吻合;②剑突下做长度约2 cm工作孔,内镜下暴露LAD后,由工作孔送入搭桥稳定器,利用机械臂在内镜下行ITA至LAD吻合。Endo-A-CAB已证明具有较高的安全性和有效性[9-10]。与MIDCAB相比,Endo-A-CAB可对ITA进行全程游离,且由于内镜放大、术野清晰、电刀灼烧功率小,ITA的骨骼化游离更加精确,且损伤小;且在减少呼吸机辅助时间,减少住院天数,减少术后引流,减小手术创伤及美容等方面更有优势[11]。
1.2 PCI
1.2.1 金属裸支架 PCI由PTCA技术的基础上发展而来,经股动脉或桡动脉穿刺后,导入导丝及PTCA导管,到达指定位置后,在扩张狭窄冠脉的同时,置入BMS,永久性扩张狭窄冠脉,已达到较好的治疗效果。但由于支架植入术后血管管腔丢失,血管壁内膜破坏,进而导致血小板黏附聚集,纤维蛋白原结合,血栓形成,平滑肌迁移,内膜增生,从而导致BMS植入后再狭窄。BMS短、中期再狭窄的发生率达到15%~20%。有研究表明,对于iLAD病变患者,BMS有着良好的治疗效果,在主要不良心血管事件(major adverse cardiovascular events,MACE)发生率及死亡率等方面与MIDCAB无显著差异[12],但在免除再次再血管化及心绞痛缓解方面不如CABG[13]。
1.2.2 DES 为抑制平滑肌细胞和内膜细胞的增殖,在BMS的基础上,DES应运而生。DES涂层主要有两种:雷帕霉素和紫杉醇。RAVEL试验是第一组DES(雷帕霉素)和BMS的RCT研究。RAVEL试验证实:DES在再狭窄发生率、血管内血栓形成、靶病变重建率(target lesion reconstruction,TLR)、靶血管失败率(target vessel failure,TVF)及MACE发生率较BMS明显低[14]。同样,在TAXUS I(紫杉醇)及随后的XIENCE V试验中,也证实了DES在免于TVF、TLR及降低MACE发生率的优越性[15-16]。
1.2.3 可降解支架 为进一步减少靶血管再狭窄风险,降低MACE发生率,有学者在上世纪90年代提出可降解支架的概念。可降解支架主要以聚乳酸、镁、酪氨酸等为基础材料,目前研究最多为生物可降解支架(biodegradable stent,BDS)。ABSORB EXTEND试验表明,可降解支架在降低血管再狭窄、减少血管内血栓形成及降低MACE发生率等方面疗效喜人[17]。BIOSOLVE-Ⅰ试验表明可降解支架在单支冠脉病变的患者中疗效显著,植入成功率100%,TLR事件发生率低,且在12个月随访时未发现心源性死亡和支架内血栓形成[18]。虽然研究表明可降解支架的疗效鼓舞人心,但目前缺乏中远期疗效的证据,故可降解支架仍处论证当中。
2 CABG与PCI疗效对比
近年对于CABG与PCI在冠脉多支病变(MVD)患者中的研究较多,而两种再血管化方式在iLAD病变患者中的研究较少,见图1。多项研究证实,对于左主干病变(leftmain disease,LMD)患者及多支血管病变(multivessel disease,MVD)患者,CABG在减低患者死亡率、降低心梗发生率及减少再次再血管化方面优于PCI,但发生卒中的风险较高[19]。对CABG与PCI在MVD患者的研究中,SYTAX试验最为经典,对于低射血分数、三支病变及糖尿病患者等SYTAX评分较高患者,CABG较PCI具有更为显著的临床效果[20-21]。对于iLAD的研究中,共有10篇RCT论著对CABG和PCI的疗效进行比较,见表1。多项研究指出,两者在术后30天、1年及5年的死亡率、卒中发生率及心梗发生率方面无显著差别。CABG在减少再次再血管化和心绞痛缓解方面优于PCI,但CABG患者的平均住院天数为PCI患者的3.2倍,且伴有更高的输血率、术后早期心律失常发生率和心外科围术期相关并发症发生率[22]。
2.1 CABG与PCI术后早期疗效对比 接受CABG和PCI的iLAD患者30天内术后生存率高达99%,两者在术后30天生存率方面无显著差异,且与CCABG相比,OPCABG与MIDCAB在生存率方面均与PCI无显著差异。与MVD患者不同,iLAD患者在PCI或CABG术后的卒中发生率无显著差别;原因可能为接受CABG的iLAD患者多采用ITA至LAD吻合,不涉及钳夹升主动脉的操作,故卒中发生率低。在术后早期心肌梗死(myocardial infarction,MI)发生率方面,CABG与PCI无显著差异。在围术期心律失常方面,CABG高于PCI,这在AMIST和SIMA的研究中均有提及[23-24],但此两项研究中,CABG均在体外循环下完成,体外循环可能为诱发术后房颤的因素。在围术期输血方面,CABG高于PCI,这可能与外科创伤相关。
2.2 CABG与PCI术后中、远期疗效对比 接受CABG和PCI的iLAD患者在术后1年及5年的生存率与心梗发生率方面无显著差异。在降低再次再血管化发生率及心绞痛缓解方面,CABG明显优于PCI。在AMIST和SIMA的研究中,同时对CABG和PCI患者术后的生存质量予以评估,方式包括SF-36评分、西雅图心绞痛评分及EuroQol评分,随访时间为术后6个月至15个月,结果显示两者在患者术后生活质量方面无明显差异[23-24]。在随访长达10年的SIMA试验中,Jean-Jacques等人对行CABG和植入BMS的患者进行对比,发现其在生存率与心梗发生率方面无显著差异,但PCI患者的再次再血管化发生率及支架内血栓形成率较高,尤其在术后1个月内发生率较高,因此作者指出,应用DES可能会减小这一差距[25]。
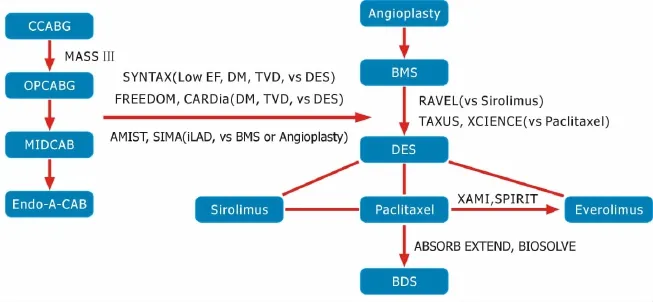
图1 冠状动脉再血管化的经典随机对照实验

表1 iLAD患者的10篇RCT试验
2.3 DES与CABG疗效对比 与BMS相比,DES在再狭窄发生率、血管内血栓形成、TLR、TVF及MACE发生率等方面体现出诸多优势,而可降解支架目前正在研发、论证阶段,且未大规模应用于临床,因此DES为目前PCI治疗的主流。SYNTAX试验、FREEDOM试验及CARDia试验阐述了在三支病变患者及糖尿病患者中,CABG较DES有更为优越的临床效果,但其卒中发生率较高[26-27]。对于左主干病变患者,CABG较DES在生存率、卒中发生率及MI发生率方面无显著差异,TLR发生率在DES患者中发生率较高[28-30]。对于DES与CABG在iLAD病变患者中的研究较少,仅有两篇RCT试验,两篇RCT均为MIDCAB与DES的比较,其中Thiele等人随访12个月,证实MIDCAB与DES患者在生存率、TLR发生率及MACE发生率方面无显著差异[31];而Hong等人证实,虽然二者在临床疗效方面无显著差异,但CABG的平均住院天数及围术期并发症发生率略高于DES患者[32]。上述两篇RCT试验随访时间较短,随访人数较少,因此在CABG与PCI疗效对比的证据上略显不足。
3 小结
iLAD的再血管化治疗一直是冠脉血运重建领域中争论较多但研究较少的话题。在疗效上,目前的研究证实CABG与PCI在生存率、卒中发生率及MI发生率方面无显著差异,但CABG在减低TLR发生率和心绞痛缓解方面明显优于PCI。DES是PCI领域一项里程碑的发展,其疗效优于BMS。但在既往的研究中,所涉及的DES支架多为雷帕霉素及紫杉醇涂层,而极少涉及雷帕霉素衍生物—依维莫司涂层支架。在SPIRIT IV试验及XAMI试验中已证实,依维莫司支架与紫杉醇支架相比,依维莫司支架1年内的TLR发生率及MACE发生率低于紫杉醇支架[33-34]。同样,对于可降解支架,已有研究证实其在降低血管再狭窄、减少血管内血栓形成及降低MACE发生率等方面更为优越。因此,依维莫司DES及可降解支架是否在疗效上更胜于CABG有待进一步证实。
与CABG相比,更多的人选择PCI治疗,主要因为其创伤小且住院时间短。但对于LAD严重钙化、迂曲、狭窄部位存在大分叉血管及LAD闭塞而行PCI困难的患者,CABG仍具有不可替代的地位,尤其在疗效上,iLAD病变患者多采用ITA至LAD吻合,ITA桥血管10~20年的通畅率为95%~98%,目前无任何一种支架可与之比拟[35]。但与PCI相比,CABG具有住院时间长、手术创伤大、术后早期心律失常及输血率高等弱点。随着CABG技术的不断革新,OPCABG、MIDCAB在C-CABG的技术基础上有了极大提升,尤其是Endo-A-CAB,不但具有较高的安全性和可靠性,而且兼顾了OPCAB、微创及骨骼化乳内动脉等诸多优点,在减少手术创伤、减少输血、降低心外科术后围术期并发症及美容等发面具有很大的优势,因此Endo-A-CAB可作为iLAD患者的自选治疗方案。
[1] Aziz O,Rao C,Panesar SS,etal.Meta-analysisofminimally invasive internal thoracic artery bypass versus percutaneous revascularisation for isolated lesions of the left anterior descending artery[J].BMJ,2007,334(7594):617.
[2] Califf RM,Tomabechi Y,Lee KL,et al.Outcome in one-vessel coronary artery disease[J].Circulation,1983,67(2):283-290.
[3] Hueb WA,Bellotti G,de Oliveira SA,etal.The Medicine,Angioplasty or Surgery Study.(MASS):a prospective,randomized trial ofmedical therapy,balloon angioplasty or bypass surgery for single proximal left anterior descending artery stenoses[J].JAm Coll Cardiol,1995,26(7):1600-1605.
[4] Butler J,Rocker GM,Westaby S.Inflammatory response to cardiopulmonary bypass[J].Ann Thorac Surg,1993,55(2):552-559.
[5] Hueb W,Lopes NH,Pereira AC,etal.Five-year follow-up of a randomized comparison between off-pump and on-pump stable multivessel coronary artery bypass grafting.The MASS III Trial[J].Circulation,2010,122(11 Suppl):S48-52.
[6] Al-Ruzzeh S,George S,Bustami M,et al.Effect of off-pump coronary artery bypass surgery on clinical,angiographic,neurocognitive,and quality of life outcomes:randomised controlled trial[J].BMJ,2006,332(7554):1365.
[7] Hickey GL,Pullan M,Oo A,etal.A comparison of survival between on-pump and off-pump left internalmammary artery bypass graft surgery for isolated left anterior descending coronary artery disease:an analysis of the UK National Adult Cardiac Surgery Audit Registry[J].Eur JCardiothorac Surg,2016,49(5):1441-1449.
[8] Vicol C,Nollert G,Mair H,et al.Midterm results of beating heart surgery in 1-vessel disease:minimally invasive direct coronary artery bypass versus off-pump coronary artery bypasswith full sternotomy[J].Heart Surg Forum,2003,6(5):341-344.
[9] Yang M,Wu Y,Wang G,etal.Robotic Total Arterial Off-Pump Coronary Artery Bypass Grafting:Seven-Year Single-Center Experience and Long-Term Follow-Up of Graft Patency[J].Ann Thorac Surg,2015,100(4):1367-1373.
[10] HalkosME,Liberman HA,Devireddy C,etal.Early clinical and angiographicoutcomes after robotic-assisted coronary artery bypass surgery[J].JThorac Cardiovasc Surg,2014,147(1):179-185.
[11] Wu Y,Gao CQ,Yang M,et al.Comparison of sternotomy offpump coronary artery bypass and minimally invasive technique for isolated single vessel grafting[J].Zhonghua Yi Xue Za Zhi,2012,92(14):974-976.
[12] Diegeler A,Thiele H,Falk V,et al.Comparison of stenting with minimally invasive bypass surgery for stenosis of the left anterior descending coronary artery[J].N Engl JMed,2002,347(8): 561-566.
[13] Blazek S,Holzhey D,Jungert C,etal.Comparison of bare-metal stenting with minimally invasive bypass surgery for stenosis of the left anterior descending coronary artery:10-year follow-up of a randomized trial[J].JACC Cardiovasc Interv,2013,6(1):20-26.
[14] Regar E,Serruys PW,Bode C,et al.Angiographic findings of themulticenter Randomized Study With the Sirolimus-Eluting Bx Velocity Balloon-Expandable Stent(RAVEL):sirolimus-eluting stents inhibit restenosis irrespective of the vessel size[J].Circulation,2002,106(15):1949-1956.
[15] Grube E,Silber S,Hauptmann KE,et al.TAXUS I:six-and twelve-month results from a randomized,double-blind trial on a slow-release paclitaxel-eluting stent for de novo coronary lesions[J].Circulation,2003,107(1):38-42.
[16] Gada H,Kirtane AJ,Newman W,et al.5-year results of a randomized comparison of XIENCE V everolimus-eluting and TAXUS paclitaxel-eluting stents:final results from the SPIRIT III trial (clinical evaluation of the XIENCE V everolimus eluting coronary stent system in the treatment of patients with de novo native coronary artery lesions)[J].JACC Cardiovasc Interv,2013,6(12): 1263-1266.
[17] Abizaid A,Ribamar Costa J,Bartorelli AL,et al.The ABSORB EXTEND study:preliminary report of the twelve-month clinical outcomes in the first 512 patients enrolled[J].EuroIntervention,2015,10(12):1396-1401.
[18] Haude M,Erbel R,Erne P,et al.Safety and performance of the drug-eluting absorbable metal scaffold(DREAMS)in patients with de-novo coronary lesions:12 month results of the prospective,multicentre,first-in-man BIOSOLVE-I trial[J].Lancet,2013,381(9869):836-844.
[19] Al Ali J,Franck C,Filion KB,etal.Coronary artery bypass graft surgery versus percutaneous coronary intervention with first-generation drug-eluting stents:a meta-analysis of randomized controlled trials[J].JACCCardiovasc Interv,2014,7(5):497-506.
[20] Kappetein AP,Head SJ,Morice MC,et al.for the SYNTAX Investigators.Treatment of complex coronary artery disease in patients with diabetes:5-year results comparing outcomes ofbypass surgery and percutaneous coronary intervention in the SYNTAX trial[J].Eur JCardiothorac Surg,2013,43(5):1006-1013.
[21] Farooq V,van Klaveren D,Steyerberg EW,etal.Anatomical and clinical characteristics to guide decision making between coronary artery bypass surgery and percutaneous coronary intervention for individual patients:development and validation of SYNTAX[J].score II.Lancet,2013,381(9867):639-650.
[22] Kapoor JR,Gienger AL,ArdehaliR,etal.Isolated disease of the proximal leftanterior descending artery comparing the effectiveness of percutaneous coronary interventions and coronary artery bypass surgery[J].JACC Cardiovasc Interv,2008,1(5):483-491.
[23] Reeves BC,Angelini GD,Bryan AJ,et al.A multi-centre randomized controlled trial of minimally invasive direct coronary bypass grafting versus percutaneous transluminal coronary angioplasty with stenting for proximal stenosis of the left anterior descending coronary artery[J].Health Technol Assess,2004,8(16):1-43.
[24] Goy JJ,Kaufmann U,Goy-Eggenberger D,et al.A prospective randomized trial comparing stenting to internal mammary artery grafting for proximal,isolated de novo left anterior coronary artery stenosis:the SIMA trial[J].Mayo Clin Proc,2000,75(11): 1116-1123.
[25] Goy JJ,Kaufmann U,Hurni M,et al.10-year follow-up of a prospective randomized trial comparing bare-metal stenting with internalmammary artery grafting for proximal,isolated de novo left anterior coronary artery stenosis the SIMA(Stenting versus Internal Mammary Artery grafting)trial[J].JAm Coll Cardiol,2008,52 (10):815-817.
[26] Farkouh ME,DomanskiM,Sleeper LA,etal.for the FREEDOM Trial Investigators.Strategies for multivessel revascularization in patients with diabetes[J].N Engl JMed,2012,367(25):2375-2384.
[27] Kapur A,Hall RJ,Malik IS,et al.Randomized comparison of percutaneous coronary intervention with coronary artery bypass grafting in diabetic patients:1-year results of the CARDia(Coronary Artery Revascularization in Diabetes)trial[J].J Am Coll Cardiol,2010,55(5):432-440.
[28] Boudriot E,Thiele H,Walther T,et al.Randomized comparison of percutaneous coronary intervention with sirolimus-eluting stents versus coronary artery bypass grafting in unprotected leftmain stem stenosis[J].JAm Coll Cardiol,2011,57(5):538-545.
[29] Park SJ,Kim YH,Park DW,et al.Randomized trial of stents versus bypass surgery for leftmain coronary artery disease[J].N Engl JMed,2011,364(18):1718-1727.
[30] Alam M,Huang HD,Shahzad SA,et al.Percutaneous coronary intervention vs.coronary artery bypass graft surgery for unprotected leftmain coronary artery disease in the drug-eluting stents eradan aggregate data meta-analysis of 11,148 patients[J].Circ J,2013,77(2):372-382.
[31] Thiele H,Neumann-Schniedewind P,Jacobs S,et al.Randomized comparison ofminimally invasive direct coronary artery bypass surgery versus sirolimus-eluting stenting in isolated proximal left anterior descending coronary artery stenosis[J].JAm Coll Cardiol,2009,53(25):2324-2331.
[32] Hong SJ,Lim DS,Seo HS,etal.Percutaneous coronary intervention with drug-eluting stent implantation vs.minimally invasive direct coronary artery bypass(MIDCAB)in patientswith leftanterior descending coronary artery stenosis[J].Catheter Cardiovasc Interv,2005,64(1):75-81.
[33] Stone GW,Rizvi A,Newman W,et al.Everolimus-eluting versus paclitaxel-eluting stents in coronary artery disease[J].N Engl JMed,2010,362(18):1663-1674.
[34] Hofma SH,Brouwer J,Velders MA,et al.Second-generation everolimus-eluting stents versus first-generation sirolimus-eluting stents in acutemyocardial infarction:1-year results of the randomized XAMI(XienceV Stent vs[J].Cypher Stent in Primary PCI for Acute Myocardial Infarction)trial.JAm Coll Cardiol,2012,60(5):381-387.
[35] Jaik NP,Umakanthan R,Leacche M,et al.Current status of hybrid coronary revascularization[J].Expert Rev Cardiovasc Ther,2011,9(10):1331-1337.
2016-07-15)
2016-08-30)
10.13498/j.cnki.chin.j.ecc.2017.01.15
100853北京,中国人民解放军总医院心血管外科
高长青,Email,gaochq301@hotmail.com