Esophagogastric malignancies detected in a tertiary surgical center endoscopy unit from Turkey: a descriptive study
2017-03-23OrhanUreyenUlviMehmetMeralMuratUzEnverIlhan
Orhan Ureyen, Ulvi Mehmet Meral, Murat Uz, Enver Ilhan
(1. Department of Genaral Surgery, Health Sciences Universty Izmir Bozyaka Training and Research Hospital, Division A, Izmir, Turkey;2. Department of General Surgery, Izmir Katip Celebi University Ataturk Training and Research Hospital, Izmir, Turkey)
Contributions: Conception and design: O Üreyen, M Uz; Administrative support: E Ilhan, UM Meral; Provision of study materials or patients:O Üreyen, E Ilhan; Collection and assembly of data: M Uz, UM Meral; Data analysis and interpretation: O Üreyen, E Ilhan; Manuscript writing:All authors; (VII) Final approval of manuscript: All authors.
Introduction
The most common symptoms of upper gastrointestinal(UGI) diseases are epigastric pain and heartburn,nausea and vomiting,regurgitation and swallowing difficulties(dysphagia).While these symptoms may be signs of functional disorders of the gastrointestinal tract,they can indicate a serious UGI disease[1].Despite the reduction in the frequency of UGI diseases including peptic ulcer especially with the introduction of proton pump inhibitors,these diseases still holds an important place in surgical practice[2].
Gastric cancer is one of the leading causes of cancer deaths worldwide and approximately 990 000 new cases are being diagnosed annually and prognosis depend on the tumor stage[3].Gastric cancer is the cause of 776 000 deaths per year worldwide.The disease shows a various distribution in different geographical regions.Due to the relatively high incidence of gastric cancer;Japan,South Korea,Chile and Venezuela implement national screening programs for gastric cancer,even though routine screening programs is not recommended in other countries[4].
Due to the absence of specific clinical symptoms of esophageal and gastric cancer,endoscopy should be performed to the cases with alarm symptoms for early diagnosis[5].Endoscopic examination is the most reliable method for assessing UGI evaluation[6].The frequency of detection of malignant tumors in endoscopy among people who has complaints about UGI tract is very low,esophageal and gastric cancer incidence is 0.2–0.4% and 0.5–2.4%,respectively[1].In this study,we investigated the incidence of malignancy in the patients who underwent UGI endoscopy in our tertiary surgical center.
Methods
Malignant tumors detected in UGI endoscopies performed between Dec 31,2015 and Jan 1,2011 were included in our study.Age,gender,indication for endoscopy (presence or absence of alarm symptoms),tumor site,tumor type,stage of disease,type of treatment data were recorded.Malignancy detected cases were classified as gastric and esophageal tumors.Gastric tumors were classified according to the localization of tumor as 1/3 proximal,1/3 middle and 1/3 distal.The presence of weight loss,persistent vomiting,anemia,dysphagia,gastric surgery and palpable mass was determined as alarm symptoms[7].7th Edition UICC/AJCC TNM staging system was used for tumor staging.Statistical analysis
Only descriptive analysis was used because of limited of cases.
Results
According to the analysis of five-year patient data;39 (1.17%) of 3,309 cases had malignancy in the UGI endoscopy.The average age of malignancy detected cases were 63.4 years (range,33–88 years).There were 15 females and 24 males,giving a female-to-male preponderance of 1:1.7.In the malignancy positive group;35 (1%) cases had gastric 4 (0.12%) cases had esophagus tumors.In the fi rst UGI endoscopy of malignancy detected cases;27 (69.2%) had polipoid mass lesion,7 (17.9%)had ulcerovegetan mass,3 (7.69%) had edematous gastric mucosa and 2 (5.13%) had linitis plastica.Squamous cell carcinoma was the only pathological diagnosis of four esophageal malignancy cases.According to the gastric localization of tumors,12 of cases were distal,10 were proximal,7 were middle and 4 were linitis plastica.Two of the cases had previous gastric surgery and the gastric malignancy of these cases was localized at the gastrojejunostomy site.In terms of pathological diagnosis;29 of gastric tumors were adenocarcinoma,5 of them were signet-ring cell carcinoma and one of them was lymphoma.
The most frequent symptoms were abdominal pain,anemia,dyspepsia,bleeding,weight loss,obstruction and dysphagia in patients with gastric cancer (Table 1).Two(5.7%) of the cases had previous gastrectomies because of benign causes.Malignant tumors were detected in the remnant tissue of these cases.All of the patients with esophageal tumor were referred to a physician with dysphagia.The percentage of over 50-year-old patients was 89.7% in UGI malignancy detected patients.Three (8.6%)of the gastric tumor detected cases were excluded from analysis of our study because of their de fi nitive treatment was not performed in our institute.Three percent of gastric cancers were stage I,18% of them were stage II,25%of them were stage III and 53% of the cases were stage IV.Seventy-five percent of esophageal cancer cases had systemic metastases.According to the treatment;40.6% of the gastric cancer patients had curative surgery,21.8% of cases had palliative surgery.The distribution of our patients about staging at the diagnosis and type of surgery is shown in Table 2.

Table 1 The complaints of patients with gastric malignancies in the fi rst admittance
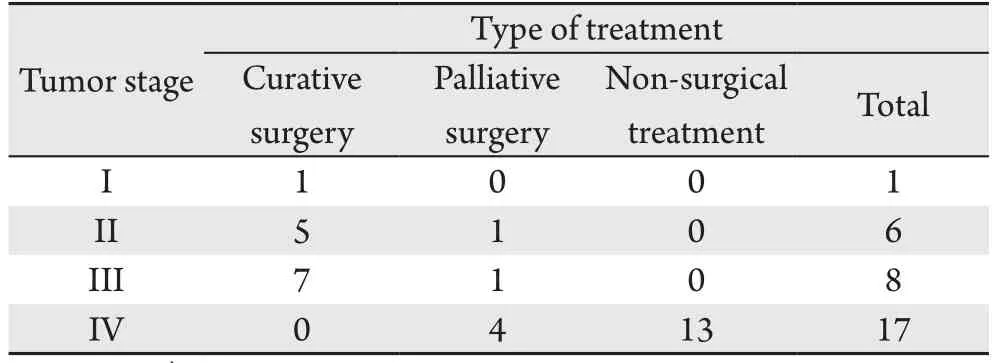
Table 2 The distribution of patients according to gastric tumor staging and surgical treatment types1)
Discussion
Gastroduodenoscopy is a common test for the patients with the complaints of dyspepsia and reflux,to reveal the cause of the warning symptoms and upper abdominal complaints[8].The method is protecting its popularity about recognition of the lesion,taking biopsies and performing essential interventions[9].Therefore,application of endoscopy for UGI symptoms is a gold standard diagnostic method[1].
Despite developing modern diagnostic appliances,advanced surgical techniques,radiation and chemotherapeutic treatment;of gastric cancer takes an important place in cancer deaths due to its rapid progression[8].In a SEER data analysis,5-year survival was reported as 27% for the patient with all stages during 2002–2008[10].
For the male gender;gastric cancer is nearly two times more than female,this rate is five times for esophageal cancer[11].In our study;while this rate was 1.7/1 for gastric cancer and 1/1 for esophageal cancer.In a study of Vradelis et al.,they examined data of 3 years and 9,764 cases and found the gastric cancer incidence as 0.8% and the average age as 76.0[12].While the gastric cancer incidence is lower than our study,average age was higher than ours in their study.In the study of Kobayashi et al.,this rate was reported at 0.9%[4].In the series of Park et al.including 54,889 cases;gastric cancer rate was reported as 0.14%[13].We conclude this reduced rate as a result of routine gastric screening instead of symptomatic patients.Likewise;according to the Korea routine gastric cancer screening program implementation data,the incidence of gastric cancer has been identi fi ed as 0.44% to 0.47%[13].
According to the results of endoscopic studies in the literature,the incidence of esophageal cancer is below 1%,also in our study the rate is reported as 0.12%,consistent with the literature[1,14].In the studies of our country,gastric cancer incidence varies between 0.5–4%[6].In the evaluation of 3 871 endoscopies performed by general surgeons,malignancy rate was found as 1.4%.Also we found this rate as 1.17%.
Although the gastric cancer incidence is higher in patients older than the age of 40,it can also be seen in younger patients[3].In our case series,5%[2]of patients were under the age of 40.In their paper,Kobayashi et al.have maintained variations about development of gastric cancer in terms of age and they suggested different time intervals for gastric cancer screening tests.According to this suggestion,UGI endoscopy must be performed every year for the patients over the age of 70,once for 2 or 3 years for the age of 60–69 years,once for 3 or 4 years for the age of 50–59 and once for 5 years under the age of 49[4].Although the presence of suggestions about 5-year interval about UGI endoscopy for the patients under the age of 49;urgent UGI endoscopy should be performed in the presence of alarm symptoms.
Nearly 40% of gastric cancer patients are asymptomatic and have little chance for early diagnosis.Disease is mostly diagnosed in endoscopic examination of nonspecific abdominal pain and dyspepsia[7,15–16].In our study,42.8% of patients with gastric cancer had UGI endoscopies due to non-specific dyspeptic symptoms.According to our results,the presence of alarm symptoms of gastric cancer was higher than literature.Our patients’first admittance and endoscopies were performed in general surgery clinical endoscopy unit.This might be related to higher rate of alarm symptoms of our study.In the study of Stephens et al.,they reported weight loss as the most common alarm symptom[7].This was followed by intractable vomiting and hemorrhage.Moreover,this study indicated weight loss and intractable vomiting as most specific symptoms for gastric cancer.According to our results,anemia and hemorrhage were the most common alarm symptoms,respectively.
A very large part of gastric cancers in 1900’s were localized in distal gastric region.However,in recent years;the incidence of distal gastric cancer quickly decreased and esophagogastric junction tumors have been shown to be increased[17].
As in all malignancies,in gastric cancers,stage of the cancer is the main determinant of the prognosis.Upon admittance,tumor is detected further than the locoregional area over 50% of the cases[18].Because surgical resection is the current primary treatment choice,curative surgical resection should be primary target.In more than 50% of the cases whom are gone under surgery,metastasis in the regional lymph node(N+) is positive.Survey is associated with metastatic lymph node involvement.The rate of fi ve years of survival is 50% when there is no lymph node metastasis (N0),it drops down to 10% in the patients have N3[17].
Although surgery’s effect on survey is proven,40% of all the cases go under surgery[19–20].Disease is detected in advanced stages in northern countries and this is associated with poor prognosis.Because of this,curative surgery cannot be performed on many of the patients and in cases of bleeding and obstruction,surgery can be performed only for palliation.Although there is still a debate on the type and width of this surgery,radical gastrectomy and D2lymph node dissection is commonly accepted[19,21].In our study,among the patients those whom stage is detected,few of them were stage I or stage II.53% of gastric cancer cases were metastatic (stage IV) and 25% of them were stage III.All of the cases with esophagus cancer were metastatic.Among all the cases,36% of them had the chance to go under radical surgery.Seventeen percent of the cases had palliative surgery.
Our study has some limitations.It is a retrospectivedesigned study and number of cases is low.Also,future results and prognosis of the cases on whom endoscopy is performed is unknown,and rates of false negative results are unknown.Because all of the cases are consisting of patients from internal medicine and surgery outpatient clinics,endoscopy might be performed on them secondary to various symptoms and signs.For this reason,we have the idea of that any common implication cannot be made regionally or commonly.
Conclusions
As a result,UGI endoscopy is the baseline technique for the patients with gastrointestinal symptoms or complaints;in both diagnostic and treatment phases of the disease.This diagnosis/treatment tool is commonly used by the surgeons as well.Malignity is rarely detected among the patients from general surgery outpatient clinic,on whom UGI endoscopy is performed.But it is not different from the literature.Most of the malignancies are at advanced stage.In older age patients,endoscopy should be recommended even there are nonspecific symptoms.In the presence of alarm symptoms,UGI endoscopy should be recommended without considering the age.
Acknowledgements
None.
Footnote
Conflicts of Interest:This study was presented at the 51th Congress of the European Society for Surgical Research,Prague/Czech Republic held on 25–28,May,2016.
Ethical Statement:None.
[1]Sit M,Aktas G,Yılmaz EE.Endoscopy in tıme can be a life saver:our upper endoscopy results[J].Natl J Med Res,2013,3(3):270–272.
[2]Bani-Hani KE,Yaghan RJ,Heis HA,et al.Gastric malignancies in Northern Jordan with special emphasis on descriptive epidemiology[J].World J Gastroenterol,2004,10(15):2174–2178.
[3]Park CH,Kim EH,Chung H,et al.Periodic Endoscopies Might Not Increase the Detection of Early Gastric Cancer in a Young Population[J].PLoS One,2016,11(7):e0159759.doi:10.1371/journal.pone.0159759.
[4]Kobayashi D,Takahashi O,Arioka H,et al.The optimal screening interval for gastric cancer using esophago-gastro-duodenoscopy in Japan[J].BMC Gastroenterol,2012,12:144.doi:10.1186/1471–230X-12–144.
[5]Siersema PD,Dees J,Tilanus HW,et al.Early detection and treatment of oesophageal and gastric cancer.The Rotterdam Oesophageal Tumour Study Group[J].Neth J Med,1995,47(2):76–86.
[6]Polat Y.Endoscopic Experience of a Surgeon:The Evaluation of 8453 Cases[J].Int J Basic Clin Med,2015,3:1–5.
[7]Stephens MR,Lewis WG,White S,et al.Prognostic signi fi cance of alarm symptoms in patients with gastric cancer[J].Br J Surg,2005,92(7):840–846.
[8]Ferlengez E,FerlengezAkgün AG,Çelik A,et al.İkinci Basamak Bir Devlet Hastanesinde Gastroduodenoskopi Ünitesinde Tanı Konulan Olgularının Endoskopik ve Klinik Özellikleri[J].Haseki Tıp Bulteni,2012,50:131–135.
[9]Ayar Y,Şahbaz NA,Bolatkıran Y,et al.Bayburt İlinde Yapılan Üst Gastrointestinal Endoskopi Sonuçları[J].Haseki Tıp Bülteni,2013,51:116–119.
[10]Jemal A,Bray F,Center MM,et al.Global cancer statistics[J].CA Cancer J Clin,2011,61(2):69–90.doi:10.3322/caac.20107.
[11]Zhang H,Chen SH,Li YM.Epidemiological investigation of esophageal carcinoma[J].World J Gastroenterol,2004,10(12):1834–1835.
[12]Vradelis S,Maynard N,Warren BF,et al.Quality control in upper gastrointestinal endoscopy:detection rates of gastric cancer in Oxford 2005–2008[J].Postgrad Med J,2011,87(1027):335–339.doi:10.1136/pgmj.2010.101832.
[13]Park CH,Kim B,Chung H,et al.Endoscopic quality indicators for esophagogastroduodenoscopy in gastric cancer screening[J].Dig Dis Sci,2015,60(1):38–46.doi:10.1007/s10620–014–3288–y.
[14]Demir A,Bahçecioğlu İ,Çelebi S.Fırat üniversitesi tıp fakültesi hastanesinde yapılan 12022 üst gastrointestinal sistem endoskopisinin değerlendirilmesi[J].The Turkish J Gastroenterology,1999,10:86.
[15]Kısaoğlu A,Özoğul B,Yıldırgan Mi,et al.Abant Tıp Dergisi[J].Abant Med J,2014,3:220–225.
[16]Everett SM,Axon AT.Early gastric cancer in Europe[J].Gut,1997,41(2):142–150.
[17]Misleh JG,Santoro P,Strasser JF,et al.Multidisciplinary management of gastric cancer[J].Surg Oncol Clin N Am,2013,22(2):247–264.doi:10.1016/j.soc.2012.12.013.
[18]Ajani J,D'Amico TA,Hayman JA,et al.Gastric cancer.Clinical practice guidelines in oncology[J].J Natl Compr Canc Netw,2003,1(1):28–39.
[19]Brar SS,Mahar AL,Helyer LK,et al.Processes of care in the multidisciplinary treatment of gastric cancer:results of a RAND/UCLA expert panel[J].JAMA Surg,2014,149:18–25.doi:10.1001/jamasurg.2013.3959.
[20]Viudez-Berral A,Miranda-Murua C,Arias-de-la-Vega F,et al.Current management of gastric cancer[J].Rev Esp Enferm Dig,2012,104(3):134–141.
[21]Ilhan E,Demir U,Alemdar A,et al.Management of high-output chylous ascites after D2-lymphadenectomy in patients with gastric cancer:a multi-center study[J].J Gastrointest Oncol,2016,7(3):420–425.doi:10.21037/jgo.2016.02.03.
