N末端脑钠肽联合GRACE评分对非ST段抬高型急性冠脉综合征患者的远期预测
2017-02-28曹荣元赵思源顾遵
曹荣元++++++赵思源++++++顾遵才++++++张淑花++++++王正忠++++++孙黎明


[摘要] 目的 探讨N末端脑钠肽(NT-proBNP)联合全球冠状动脉事件注册(GRACE)评分与非ST段抬高型急性冠脉综合征(NSTE-ACS)患者远期预后的相关性。 方法 选取2013年1月~2015年1月在江苏省连云港市第二人民医院心内科诊断为NSTE-ACS的患者77例。患者入院24 h内测定NT-proBNP水平,计算GRACE评分。出院后对患者进行12个月的随访,将随访期间发生不良心血管事件的患者作为事件组(n=9),未发生心血管事件的患者作为非事件组(n=68)。观察NT-proBNP水平及GRACE评分对不良心血管事件的影响。 结果 研究發现事件组患者NT-proBNP水平明显高于非事件组患者,差异有高度统计学意义(P < 0.01);事件组患者的GRACE风险评分明显高于非事件组患者(P < 0.05)。Logistic回归分析表明:NT-proBNP水平和GRACE评分是NSTE-ACS患者远期不良心血管事件发生的独立预测因素(P < 0.05)。在预测NSTE-ACS患者12个月不良心血管事件发生的受试者工作特征(ROC)曲线中,NT-proBNP水平的曲线下面积为0.824(95%CI:0.774~0.848,P < 0.01),GRACE评分的曲线下面积为0.793(95%CI:0.743~0.829,P < 0.01),两项联合的曲线下面积为0.833(95%CI:0.788~0.879,P < 0.01)。 结论 NT-proBNP和GRACE评分是预测NSTE-ACS患者远期预后的可靠指标;NT-proBNP联合GRACE评分能提高评估NSTE-ACS患者远期预后的能力。
[关键词] N末端脑钠肽;GRACE评分;非ST段抬高型急性冠脉综合征
[中图分类号] R541.4 [文献标识码] A [文章编号] 1673-7210(2016)11(b)-0065-04
[Abstract] Objective To investigate the correlation of the N-terminal pro-brain natriuretic peptide (NT-proBNP) and global registered acute events (GRACE) risk score in patients with non-ST elevation acute coronary syndrome (NSTE-ACS) for long-term prognosis. Methods From January 2013 to January 2015, in the Second People's Hospital of Lianyungang, 77 cases of patients with NSTE-ACS were selected. The level of NT-proBNP was measured and GRACE score was calculated in 24 h admitted to hospital. After discharge, patients were followed up for 12 months. According to the incidence of adverse cardiovascular events during the follow-up period, all patients were divided into two groups: event group (n=9) and non event group (n=68). The effects of NT-proBNP level and GRACE score on adverse cardiovascular events were observed. Results The study found that the level of NT-proBNP in patients of the event group was significantly higher than that of patients in the non event group, the difference was statistically significant (P < 0.01). The GRACE risk score of the event group was significantly higher than that of the non event group (P < 0.05). Logistic regression analysis showed that NT-proBNP level and GRACE score were independent predictors of long-term adverse cardiovascular events in patients with NSTE-ACS (P < 0.05). The prediction of receiver operating characteristic curve (ROC) showed that the area under the curve of NT-proBNP was 0.824 (95%CI: 0.774-0.848, P < 0.01), the area under the curve of GRACE score was 0.793 (95%CI: 0.743-0.829, P < 0.01), the two joint area under the curve was 0.833 (95%CI: 0.788-0.879, P < 0.01). Conclusion NT-proBNP level and GRACE score are reliable indicators for predicting long-term prognosis of patients with NSTE-ACS. The combination of GRACE score and NT-proBNP can improve the prediction of the long-term prognosis.
[Key words] N-terminal pro-brain natriuretic peptide; GRACE score; Non ST-segment elevation acute coronary syndrome
非ST段抬高型急性冠脉综合征(NSTE-ACS)是常见的临床急重症,有时临床症状不典型,心电图变化不特异,容易延误治疗。如何早期识别高危患者成为临床研究热点。全球冠状动脑事件注册(GRACE)评分被认为是最有效的预测NSTE-ACS患者病情危险程度及预后的评分体系[1],目前广泛應用于临床,但单一指标评估有时不够全面。有研究表明,N末端脑钠肽(NT-proBNP)水平与冠心病严重程度相关[2],可作为判断心肌梗死、心力衰竭预后指标,是指导冠心病临床危险分层的指标,同时对急性冠脉综合征(ACS)患者的预后有一定的预测作用[3],但主要是针对ACS预后的相关性研究,关于NSTE-ACS患者预后的临床研究较少。本文通过检测NT-proBNP水平和GRACE评分,随访NSTE-ACS患者预后情况,探讨NT-proBNP水平和GRACE评分在NSTE-ACS患者危险分层中的临床意义及二者判断NSTE-ACS患者远期预后的意义。
1 资料与方法
1.1 一般资料
选取2013年1月~2015年1月在江苏省连云港市第二人民医院心内科诊断为NSTE-ACS的患者77例,其中男56例,女21例。入选标准符合2012年NSTE-ACS诊断和治疗指南[4]:①典型的缺血性胸痛的临床表现:静息型心绞痛、恶化型心绞痛、初发型心绞痛等;②典型的缺血性心电图改变:新发生或一过性ST段下移≥0.1 mV或T波倒置≥0.2 mV;③心肌坏死标志物,包括心肌肌钙蛋白T或I(cTnT/cTnI)或肌酸激酶同功酶(CK-MB)水平升高,则诊断为ST段抬高型心肌梗死。排除标准:合并严重肝功能障碍、感染性疾病、肺栓塞、败血症、严重凝血机制异常、自身免疫性疾病、恶性肿瘤、碘过敏试验阳性。
1.2 方法
收集入院时患者的基本情况、体格检查和实验室检查结果,包括:年龄、心率、收缩压、Killip分级、心脏骤停病史、心电图ST段下移、体质量指数等,检验肾功能肌酐、cTnI、NT-proBNP、低密度脂蛋白胆固醇(LDL-C)、血糖等化验室指标,计算GRACE评分[5]。出院后对患者进行电话随访或门诊随访,记录患者1~12个月发生主要心血管事件(MACE)情况,包括全因死亡、心源性死亡、心绞痛、再发心肌梗死、心力衰竭。根据随访期间不良心血管事件发生与否分为事件组(n=9)和非事件组(n=68)。
1.3 统计学方法
应用SPSS 22.0软件进行数据分析。计量资料正态性检验使用Kolmogorov- Smirno法。正态分布计量资料使用均数±标准差(x±s)表示,两组间比较采用t检验。采用逐步Logistic回归分析模型分析NSTE-ACS患者远期MACE发生的影响因素。采用ROC曲线分析各影响因素对NSTE-ACS患者远期MACE发生的预测价值。以P < 0.05为差异有统计学意义。
2 结果
2.1 两组一般资料比较
随访1~12个月,77例患者中共发生MACE 9例。9例中心源性死亡2例,再发心肌梗死2例,心绞痛3例,心力衰竭2例,总发生率为11.7%。两组患者年龄、心率、收缩压、血肌酐、cTnI、空腹血糖、体重指数、LDL-C等方面比较,事件组cTnI水平高于非事件组,差异有高度统计学意义(P < 0.01),其余指标两组差异无统计学意义(P > 0.05)。见表1。
2.2 两组NT-proBNP水平和GRACE评分比较
事件组患者血浆NT-proBNP水平明显高于非事件组患者,差异有高度统计学意义(P < 0.01)。事件组患者GRACE评分明显高于非事件组患者,差异有统计学意义(P < 0.05)。见表2。
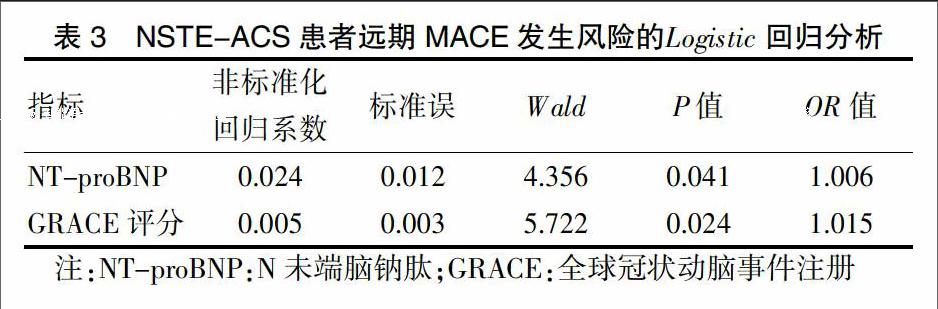
2.3 NSTE-ACS患者远期MACE发生风险的Logistic回归分析
Logistic回归分析发现,NT-proBNP水平与GRACE评分均为NSTE-ACS患者远期MACE发生风险的独立预测因素(P < 0.05)。见表3。
2.4 血浆NT-proBNP水平、GRACE评分及两项联合预测NSTE-ACS患者远期MACE发生的ROC曲线
NT-proBNP水平预测NSTE-ACS患者远期MACE发生的曲线下面积为0.824(95% CI:0.774~0.848,P < 0.01),GRACE评分的曲线下面积为0.793(95%CI:0.743~0.829,P < 0.01),两项联合的曲线下面积为0.833(95%CI:0.788~0.879,P < 0.01)。见图1。
3 讨论
NSTE-ACS是冠心病监护病房最常见疾病之一,疾病发展过程中急骤多变是对临床治疗的极大挑战。对NSTE-ACS患者依照其预后风险进行危险分层,有助于正确识别高危患者,指导分诊治疗,并以此为依据,制订更为合理的治疗策略以改善患者的临床预后。常用的危险评分模型如GRACE评分、TIMI评分等在许多大型临床试验、注册研究中得到广泛应用,价值受到肯定[6]。其中Granger等[7]创立并使用GRACE评分系统评估出院ACS患者的病死风险,它对于ACS患者的近期及远期不良结局预测准确度较高[8],优于TIMI评分[9-11]而被广泛应用于临床。目前国内外研究选择的目标研究对象多为ACS[12]患者或急性ST段抬高心肌梗死患者[13]。Aragam等[14]在分析中发现GRACE评分对NSTE-ACS患者住院期间及近期预后有较高预测价值,而GRACE评分应用于NSTE-ACS患者远期预后的研究鲜有报道,故本研究关注GRACE评分对NSTE-ACS患者远期预后的影响。
以往临床上仅用GRACE评分对ACS患者预后做出评估,但是GRACE评分也存在一定的缺陷,如数据繁多,整理麻烦。另外反映机体神经体液因素变化的指标未纳入,对心血管不良事件预测的准确性有一定影响[15]。近年来国内外提倡应用两个甚至多个指标期盼提高对NSTE-ACS远期预后的预测评估。其中NT-proBNP为研究热点之一,其作为心力衰竭的重要标志物,对预测ACS患者不良预后有重要临床意义[16-17]。多个研究证实,ACS中NT-proBNP水平明显升高的患者提示其左心功能重度下降,属于死亡的高危人群[18-19]。目前认为,NT-proBNP比其他的危险因子更有价值,NT-proBNP水平越高,其ACS远期预后越差。此前的研究主要集中于ACS特别是ST段抬高型心肌梗死(STEMI)的预后研究上,而对于NSTE-ACS这一疾病谱涉足较少,特别是将NT-proBNP水平与GRACE评分结合应用于NSTE-ACS患者危险分层的研究鲜有报道。因此,本研究对两者的远期心血管事件风险预测效力进行对比和分析,探讨二者结合能否提高预测效力。
本研究结果显示,发生MACE的患者血浆NT-proBNP水平显著高于未发生MACE的患者水平,回归分析显示血浆NT-proBNP水平是NSTE-ACS患者MACE发生风险的独立预测因子。提示血浆NT-proBNP水平是影响NSTE-ACS患者预后的独立危险因素,可作为NSTE-ACS远期预后评估的重要标志物。通过回归分析GRACE评分证实,GRACE评分亦为NSTE-ACS患者远期MACE预后的独立预测因素。
本研究使用GRACE评分联合血浆NT-proBNP预测NSTE-ACS患者预后的结果显示:血浆NT-proBNP水平和GRACE评分联合对NSTE-ACS患者远期MACE发生风险的预测效力高于二者单独预测效力。这与Sohail等[20]研究相似,但是其预测效力提高不如报道明显,考虑与其他研究入选STEMI患者为研究对象有关。此外本研究入选的患者例数较少,可能会影响客观性。
综上所述,NT-proBNP水平是影响NSTE-ACS患者预后的独立危险因素之一;NT-proBNP水平和GRACE评分是预测NSTE-ACS患者远期预后的可靠指标;NT-proBNP水平联合GRACE评分能提高预测NSTE-ACS患者远期预后的能力。如果应用GRACE评分联合NT-proBNP水平则可能更加科学有效地对NSTE-ACS患者进行临床危险分层,以此进行更有针对性的治疗。选择高危人群强化治疗方案,将会极大地减少不良心血管事件发生,改善患者预后。
[参考文献]
[1] Widera C,Pencina MJ,Meisner A,et al. Adjustment of the GRACE score by growth differentiation factor 15 enables a more accurate appreciation of risk in non-ST-elevation acute coronary syndrome [J]. Eur Heart J,2012,33(9):1095-1104.
[2] 王愛萍,张焕轶,杨曙光,等.急性冠脉综合征患者血清氮末端脑钠肽原水平与冠脉病变程度的关系[J].心脏杂志,2011,23(5):629-632.
[3] Gravning J,Smedsrud MK,Omland T,et al. Sensitive troponin assays and N-terminal pro-B-type natriuretic peptide in acute coronary syndrome:prediction of significant coronary lesions and long-term prognosis [J]. Am Heart J,2013,165(5):716-724.
[4] 中华医学会心血管病学分会,中华心血管病杂志编辑委员会.非ST段抬高急性冠状动脉综合征诊断和治疗指南[J].中华心血管病杂志,2012,40(5):353-366.
[5] Gholap NN,Mehta RL,Ng L,et al. Is admission blood glucose concentration a more powerful predictor of mortality after myocardial infarction than diabetes diagnosis? A retrospective cohort study [J]. BMJ Open,2012,2(5):e001596.
[6] Khalill R,Han L,Jing C,et al. The use of risk scores for stratification of non-ST elevation acute coronary syndrome patients[J]. Exp Clin Cardiol,2009,14(2):e25-30.
[7] Granger CB,Goldberg RJ,Dabbous O,et al. Predictors of hospital mortality in the global registry of acute coronary events[J]. Arch Intern Med,2003,163(19):2345-2353.
[8] Martins A,Ribeiro S,Goncalves P,et al. Role of central obesity in risk stratification after an acute coronary event:does central obesity add prognostic value to the Global Registry of Acute Coronary Events(GRACE)risk score in patients with acute coronary syndrome [J]. Rev Port Cardiol,2013,32(3):769-776.
[9] Eagle KA,Lim MJ,Dabbous OH,et al. A validated prediction model for all forms of acute coronary syndrome:estimating the risk of 6-month postdischarge death in an international registry [J]. JAMA,2004,291(22):2727-2733.
[10] Araujo Goncalves PA,Ferreira J,Aguiarc,et al. TIMI,PURSUIT,and GRACE risk scores:sustained prognostic value and interaction with revascularization in NSTE-ACS [J]. Eur Heart J,2005,26(9):865-872.
[11] Fox KA,Dabbous OH,Goldberg RJ,et al. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome:prospective multinational observational study(GRACE)[J]. BMJ,2006,333(7578):1091.
[12] Goodman SG,Huang W,Yan AT,et al. The expanded Global Registry of Acute Coronary Events:baseline chara-cteristics,management practices,and hospital outcomes of patients with acute coronary syndromes [J]. Am Heart J,2009,158(2):193-201.
[13] Alnasser SM,Huang W,Gore JM,et al. Late Consequences of Coronary Syndromes:Global Registry of Acute Coronary Events(GRACE)Follow-up [J]. Am J Med,2015,128(7):766-775.
[14] Aragam KG,Tamhane UU,Kline-Rogrer E,et al. Does simplicity compromise accuracy in ACS risk prediction? A retrospective analysis of the TIMI and GRACE risk scores [J]. PLoS One,2009,4(11):e7947.
[15] 趙晗,刘文娴.非ST段抬高急性冠状动脉综合征患者血浆NT-ProBNP与GRACE危险分层的关系[J].心肺血管病杂志,2011,30(2):111-115.
[16] Amsterdam EA,Wenger NK,Brindis RG,et al. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes [J]. Circulation,2014,130(25):2354-2394.
[17] Arjamaa O. Physiology of natriuretic peptides:The volume overload hypothesis revisited [J]. World J Cardiol,2014, 6(1):4-7.
[18] Omland T,Persson A,Ng L,et al. N terminal pro-B-type natriuretic peptide and long-term mortality in acute coronary syndromes [J]. Circulation,2002,106(23):2913-2918.
[19] Heeschen C,Hamm CW,Mitrovic V,et al. N-terminal pro-B-type natriuretic peptide levels for dynamic risk strati-fication of patients with acute coronary syndromes [J]. Circulation,2004,110(20):3206-3212.
[20] Sohail QK,Hafid N,Kelvin H,et al. N-terminal pro-B-type Natriuretic peptide complements the GRACE risk score in predicting early and late mortality following acute coronar ysyndrome [J]. Clin Sci,2009,117(1):31-39.
