18F-氟脱氧葡萄糖的最大标准摄取值评估宫颈癌伴淋巴结转移患者预后的价值
2017-02-17赵红霞董艳双蔡友治朱颖军
赵红霞,董艳双,蔡友治,朱颖军
·论著·
18F-氟脱氧葡萄糖的最大标准摄取值评估宫颈癌伴淋巴结转移患者预后的价值
赵红霞1,董艳双1,蔡友治2,朱颖军3*
背景 淋巴结转移是影响宫颈癌预后的主要因素,早期诊断可以有效提高患者的生存率。目的 探讨18F-氟脱氧葡萄糖(18F-FDG)的最大标准摄取值(SUVmax)评估宫颈癌伴淋巴结转移患者预后的价值,并分析患者生存率的影响因素。方法 收集2004年12月—2011年8月天津市第四中心医院妇产科经活组织检查证实的伴盆腔淋巴结转移和/或腹主动脉旁淋巴结转移宫颈癌患者70例为研究对象。患者均行正电子发射断层联合计算机断层扫描术(PET/CT)检查,记录18F-FDG的SUVmax,患者均接受放、化疗,从患者接受治疗开始随访,随访至患者复发或死亡,随访截止日期为2015-06-30。结果 SUVmax预测患者复发的受试者工作特征(ROC)曲线下面积(AUC)为0.703,95%CI(0.542,0.838),临界值为7.5,灵敏度为85.7%,特异度为98.2%,阳性预测值为92.3%,阴性预测值为96.5%,约登指数为0.8。SUVmax<7.5 13例,SUVmax≥7.5 57例。SUVmax<7.5患者与SUVmax≥7.5患者总生存率(OS)比较,差异无统计学意义(χ2=2.934,P=0.087)。SUVmax<7.5患者无病生存率(DFS)高于SUVmax≥7.5患者(χ2=4.791,P=0.035)。多元Cox比例风险回归分析结果显示,SUVmax、淋巴结转移部位、疗效反应是OS的影响因素(P<0.05);SUVmax、淋巴结转移部位、疗效反应是DFS的影响因素(P<0.05)。结论18F-FDG的SUVmax可以较好地评估宫颈癌伴淋巴结转移患者预后;18F-FDG的SUVmax较大、伴盆腔淋巴结转移、完全反应宫颈癌患者生存率较差。
宫颈肿瘤;淋巴转移;氟脱氧葡萄糖F18;最大标准摄入值
赵红霞,董艳双,蔡友治,等.18F-氟脱氧葡萄糖的最大标准摄取值评估宫颈癌伴淋巴结转移患者预后的价值[J].中国全科医学,2017,20(6):668-672.[www.chinagp.net]
ZHAO H X,DONG Y S,CAI Y Z,et al. Prognostic value of18F-FDG SUVmax in pelvic lymph nodes metastases of patients with cervical cancer[J].Chinese General Practice,2017,20(6):668-672.
宫颈癌临床症状隐匿、分化程度低、易累及淋巴结、高频复发等特点造成其病死率居高不下,宫颈癌也是临床治疗上最棘手的恶性肿瘤[1]。年龄、肿瘤分期、淋巴结的累及情况等是宫颈癌患者预后的影响因素,其中盆腔淋巴结转移及腹主动脉旁淋巴结转移与宫颈癌的临床治疗和患者预后有密切关系[2-3]。18F-氟脱氧葡萄糖(18F-FDG)正电子发射断层联合计算机断层扫描术(PET/CT)是一种将解剖位置与代谢功能相结合的检查方法,用于探测肿瘤的定位及生物学特征[4]。目前,PET/CT可以观察肿瘤浸润范围,受累淋巴结的大小、远近等,逐渐成为分析肿瘤分级的重要方法[5-6]。研究证实,原发肿瘤18F-FDG的最大标准摄取值(maximim standardized uptake,SUVmax)与肿瘤大小、淋巴结转移率、疗效反应、治疗后总生存率(OS)及无病生存率(DFS)有一定相关性[7]。但是,18F-FDG的SUVmax对宫颈癌患者预后的价值尚未明确。本研究分析70例宫颈癌伴盆腔淋巴结转移和/或腹主动脉旁淋巴结转移患者18F-FDG的SUVmax,探讨其评估宫颈癌伴淋巴结转移患者预后的价值,为临床上调整治疗方案及康复监测提供依据。
1 对象与方法
1.1 纳入与排除标准 纳入标准:(1)经PET/CT进行诊断、分级及放/化疗治疗;(2)临床诊断资料齐全;(3)伴盆腔淋巴结转移和/或腹主动脉旁淋巴结转移;(4)患者均已根据国际妇产科联盟(FIGO)标准分期[8]。排除标准:(1)病史、体格检查、妇科检查、血液生化检查、腹部和盆腔的磁共振成像或CT检查资料缺失的患者;(2)无淋巴结转移患者;(3)未进行PET/CT诊断的患者。
1.2 研究对象 收集2004年12月—2011年8月天津市第四中心医院妇产科经活组织检查证实的宫颈癌患者70例为研究对象。所有患者及其家属签署知情同意书。本研究通过天津市第四中心医院伦理审查委员会批准。
1.3 PET/CT检查[9]
1.3.1 检查方法 (1)所有患者禁食至少6 h,注射18F-FDG前检测空腹血糖水平(要求≤15 mg/L),静脉注射370~555 MBq(10~15 mCi)的18F-FDG,患者仰卧位以确保18F-FDG全身均匀分布,60 min后采集PET/CT资料。(2)非增强CT扫描颅骨底至盆腔下缘,电压140 kV,电流80 mA,层厚5 mm。(3)PET按照相对应的CT扫描区采集图像,3 min/床位,共6~7个床位。(4)采集的所有数据经衰减校正。
1.3.2 PET/CT图像分析 PET/CT图像均由同一资深影像学诊断医师双盲法阅片,根据18F-FDG分布的位置、强度、形状、大小、与CT图像的相关性等综合判断摄入的18F-FDG水平与定位。由计算机分析出18F-FDG的SUVmax。
1.4 治疗方案 盆腔淋巴结转移患者患者行三维适形放射治疗(3-dimensional conformal external beam RT,3DCRT)同步联合顺铂和高剂量(HDR)近距离放射治疗(BRT)方案。其中,3DCRT条件是18-MV光子,1.8 Gy/次(周一至周五连续放疗),共计50.4 Gy;静脉注射顺铂,40 mg/m2,1次/周;BRT条件是7.0 Gy/次。腹主动脉淋巴结转移患者,除上述治疗方案外,在腹主动脉旁淋巴结进行额外放射,1.8 Gy/次,共计45.0 Gy,若发现淋巴结肿大,额外增加9.0 Gy的放射剂量。
1.5 随访 从患者接受治疗开始电话或门诊随访,治疗后≤3年,3个月随访1次;治疗后>3年,6个月随访1次,随访至患者复发或死亡,随访截止日期为2015-06-30,随访时间为6~70个月。疗效反应:完全反应(complete response,CR)为所有目标病灶消失;局部反应(partial response,PR)为基线病灶最大径之和至少减少30%;病变进展(progressive disease,PD)为基线病灶最大径之和至少增加20%或出现新病灶。发生远端转移定义为复发。

2 结果
2.1 基本情况 70例患者年龄30~89岁,平均年龄(55.7±17.8)岁;FIGO临床分期:ⅠB2期5例,ⅡA期1例,ⅡB期34例,ⅢA期8例,ⅢB期20例,ⅣA期2例;鳞癌55例,腺癌14例,鳞腺癌1例;单纯盆腔淋巴结转移48例,盆腔淋巴结转移及腹主动脉旁淋巴结转移22例;疗效反应:CR50例,PR18例,PD2例;平均SUVmax(7.6±0.5);疾病复发14例,存活30例,死亡26例(其中24例死于宫颈癌,2例死于其他疾病)。
2.2SUVmax预测患者复发的价值SUVmax预测患者复发的AUC为0.703,95%CI(0.542,0.838),临界值为7.5,灵敏度为85.7%,特异度为98.2%,阳性预测值为92.3%,阴性预测值为96.5%,约登指数为0.8(见表1)。

表1 SUVmax预测患者复发的价值
注:SUVmax=最大标准摄取值
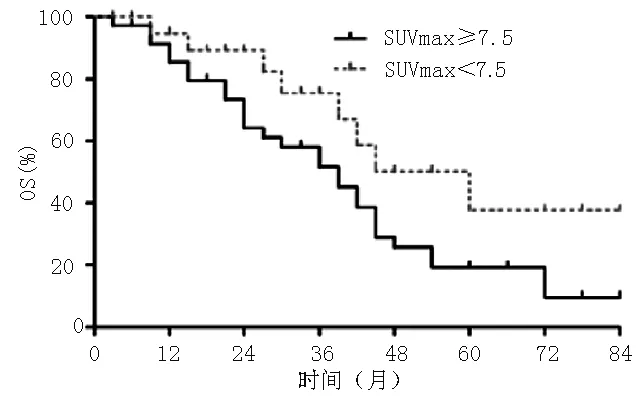
2.3 OS、DFS比较 SUVmax<7.5 57例,SUVmax≥7.5 13例。SUVmax<7.5患者与SUVmax≥7.5患者OS比较,差异无统计学意义(χ2=2.934,P=0.087,见图1)。SUVmax<7.5患者DFS高于SUVmax≥7.5患者,差异有统计学意义(χ2=4.791,P=0.035,见图2)。
2.4 OS、DFS影响因素的多元Cox比例风险回归分析 以生存时间、OS为因变量,SUVmax、临床分期、淋巴结转移部位、疗效反应为自变量(见表2),进行多元Cox比例风险回归分析,结果显示,SUVmax、淋巴结转移部位、疗效反应是OS的影响因素(P<0.05,见表3)。
以生存时间、DFS为因变量,SUVmax、临床分期、淋巴结转移部位、疗效反应为自变量(见表2),进行多元Cox比例风险回归分析,结果显示,SUVmax、淋巴结转移部位、疗效反应是DFS的影响因素(P<0.05,见表4)。
注:OS=总生存率
图1 SUVmax<7.5患者与SUVmax≥7.5患者OS比较
Figure 1 Comparison of OS of patients of SUVmax<7.5 and SUVmax≥7.5

注:DFS=无病生存率
图2 SUVmax<7.5患者与SUVmax≥7.5患者DFS比较
Figure 2 Comparison of DFS of patients of SUVmax<7.5 and SUVmax≥7.5
表2 OS、DFS影响因素的多元Cox比例风险回归分析赋值表
Table 2 Assignment of multivariate Cox proportional hazard regression analysis of influencing factors for OS and DFS
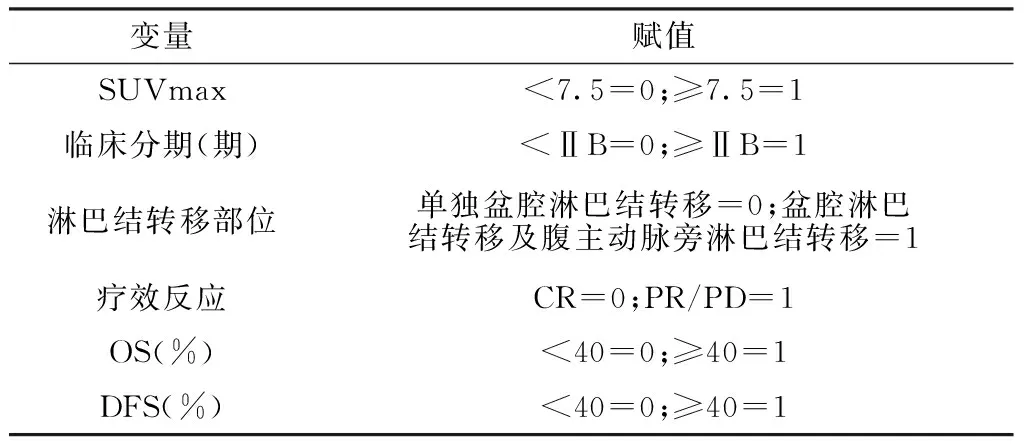
变量赋值SUVmax<7.5=0;≥7.5=1临床分期(期)<ⅡB=0;≥ⅡB=1淋巴结转移部位单独盆腔淋巴结转移=0;盆腔淋巴结转移及腹主动脉旁淋巴结转移=1疗效反应CR=0;PR/PD=1OS(%)<40=0;≥40=1DFS(%)<40=0;≥40=1
注:CR=完全反应,PR=局部反应,PD=疾病进展
表3 OS影响因素的多元Cox比例风险回归分析
Table 3 Multivariate Cox proportional hazard regression analysis of influencing factors for OS
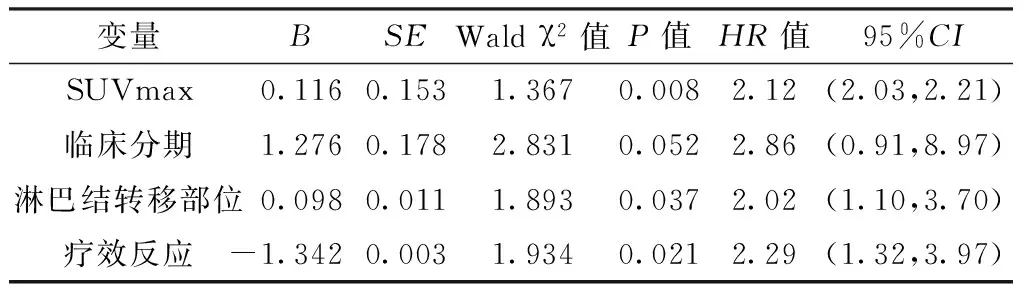
变量BSEWaldχ2值P值HR值95%CISUVmax0.1160.1531.3670.0082.12(2.03,2.21)临床分期1.2760.1782.8310.0522.86(0.91,8.97)淋巴结转移部位0.0980.0111.8930.0372.02(1.10,3.70)疗效反应-1.3420.0031.9340.0212.29(1.32,3.97)
表4 DFS影响因素的多元Cox比例风险回归分析
Table 4 Multivariate Cox proportional hazard regression analysis of influencing factors for DFS

变量BSEWaldχ2值P值HR值95%CISUVmax0.9340.1344.2810.0022.12(2.04,2.21)临床分期1.0240.0012.7810.1672.71(0.93,7.99)淋巴结转移部位3.1340.2912.1030.0412.05(1.15,3.64)疗效反应-1.2310.0211.9330.0042.32(1.92,2.80)
3 讨论
多项研究表明,早期、精确、高效诊断淋巴结转移是解决宫颈癌的治疗及疾病控制的重要前提[9]。淋巴结的转移基本上遵循着从盆腔淋巴结、腹主动脉旁淋巴结,到锁骨淋巴结,后期至纵隔淋巴结这一过程。作为淋巴结转移的首站,盆腔淋巴结转移的探查是决定宫颈癌治疗策略和评估预后的主要因素。PET/CT能够综合病灶的解剖位置和代谢水平,有效评估宫颈癌患者肿瘤分期[10],但关于其对疾病的进展及预后评估的研究较少。本研究采用PET/CT检查手段,探讨18F-FDG的SUVmax评估宫颈癌伴淋巴结转移患者预后的价值。
本研究结果显示,SUVmax预测患者复发的AUC为0.703,95%CI(0.542,0.838),临界值为7.5,灵敏度为85.7%,特异度为98.2%,阳性预测值为92.3%,阴性预测值为96.5%,约登指数为0.8;SUVmax<7.5患者与SUVmax≥7.5患者OS无差异,SUVmax<7.5患者DFS高于SUVmax≥7.5患者。有研究证实,与无淋巴结转移的宫颈癌患者相比,有淋巴结转移的宫颈癌患者5年生存率降低了30%~40%;而伴有盆腔淋巴结转移及腹主动脉旁淋巴结转移的宫颈癌患者5年生存率降低了20%~60%[11]。GRIGSBY等[12]发现,淋巴结18F-FDG摄入与DFS显著相关。YOON等[13]发现,18F-FDG低摄入其疗效反应好,CR患者的DFS和OS高于无反应患者或PR患者。有研究表明,83例FIGO临床分期为ⅠB期~ⅢB期的宫颈癌患者,SUVmax≥4.3患者复发率高、OS和DFS低、预后差[14]。另一项研究表明,SUVmax≥2.36的宫颈癌患者OS及DFS相对于SUVmax<2.36差[15]。此外,OH等[16]发现,60例宫颈癌患者经放、化疗后,18F-FDG的SUVmax减少≥60%时其疗效反应好,疾病无快速进展。结合以上研究数据和本研究结果,提示18F-FDG的摄入水平与宫颈癌进展程度、疗效低反应、低生存率有关。
有关宫颈癌的预后因素很多,包括临床肿瘤分级、肿瘤浸润范围、分化程度、鳞状上皮细胞癌抗原(squamous cell carcinoma antigen,SCC-Ag)水平、淋巴结转移率等。KIDD等[17]结合Cox比例风险回归分析发现,盆腔淋巴结18F-FDG的SUVmax增高(≥4.3)可作为宫颈癌的独立预后因子;CHUNG等[18]研究显示,盆腔淋巴结18F-FDG的SUVmax和宫旁浸润程度是宫颈癌复发的危险因素。本研究结果显示,SUVmax、淋巴结转移部位、疗效反应是OS的影响因素,SUVmax、淋巴结转移部位、疗效反应是DFS的影响因素,与其他研究结果[19]不一致,可能的原因是本研究筛选的资料多数是单纯盆腔淋巴结转移的宫颈癌患者,且ROC曲线分析得到的SUVmax预测患者复发的临界值也高于其他研究[20]。
本研究有一些局限性。首先,本研究样本量有限。其次,PET/CT本身有部分容积效应,在探查淋巴结时,降低了分辨率,低估了淋巴结转移率。增加样本量和提高PET/CT及仪器的分辨率能更准确地分析18F-FDG的SUVmax对宫颈癌诊断、治疗及预后的临床意义。本研究并未涉及远端淋巴结转移的患者,仍需进一步研究。
综上所述,18F-FDG的SUVmax可以较好地评估宫颈癌伴淋巴结转移患者预后;18F-FDG的SUVmax较大、伴盆腔淋巴结转移、完全反应宫颈癌患者生存率较差。
作者贡献:赵红霞进行试验设计与实施、资料收集整理、撰写论文并对文章负责;赵红霞、董艳双、蔡友治、朱颖军进行试验实施、评估、资料收集;朱颖军进行质量控制及审校。
本文无利益冲突。
[1]FOROUZANFAR M H,FOREMAN K J,DELOSSANTOS A M,et al.Breast and cervical cancer in 187 countries between 1980 and 2010:a systematic analysis[J].Lancet,2011,378(9801):1461-1484.
[2]ATAHAN I L,ONAL C,OZYAR E,et al.Long-term outcome and prognostic factors in patients with cervical carcinoma:a retrospective study[J].Int J Gynecol Cancer,2007,17(4):833-842.
[3]KIDD E A,SIEGEL B A,DEHDASHTI F,et al.Lymph node staging by positron emission tomography in cervical cancer:relationship to prognosis[J].J Clin Oncol,2010,28(12):2108-2113.
[4]MONTEIL J,MAUBON A,LEOBON S,et al.Lymph node assessment with(18)F-FDG-PET and MRI in uterine cervical cancer[J].Anticancer Res,2011,31(11):3865-3871.
[5]LV K,GUO H M,LU Y J,et al.Role of18F-FDG PET/CT in detecting pelvic lymph-node metastases in patients with early-stage uterine cervical cancer:comparison with MRI findings[J].Nucl Med Commun,2014,35(12):1204-1211.
[6]GOUY S,MORICE P,NARDUCCI F,et al.Prospective multicenter study evaluating the survival of patients with locally advanced cervical cancer undergoing laparoscopic para-aortic lymphadenectomy before chemoradiotherapy in the era of positron emission tomography imaging[J].J Clin Oncol,2013,31(24):3026-3033.
[7]ONAL C,REYHAN M,GULER O C,et al.Treatment outcomes of patients with cervical cancer with complete metabolic responses after definitive chemoradiotherapy[J].Eur J Nucl Med Mol Imaging,2014,41(7):1336-1342.
[8]ONAL C,REYHAN M,PARLAK C,et al.Prognostic value of pretreatment18F-fluorodeoxyglucose uptake in patients with cervical cancer treated with definitive chemoradiotherapy[J].Int J Gynecol Cancer,2013,23(6):1104-1110.
[9]ONAL C,OYMAK E,FINDIKCIOGLU A,et al.Isolated mediastinal lymph node false positivity of18F-fluorodeoxyglucose-positron emission tomography/computed tomography in patients with cervical cancer[J].Int J Gynecol Cancer,2013,23(2):337-342.
[10]KIDD E A,SIEGEL B A,DEHDASHTI F,et al.Pelvic lymph node F-18 fluorodeoxyglucose uptake as a prognostic biomarker in newly diagnosed patients with locally advanced cervical cancer[J].Cancer,2010,116(6):1469-1475.
[11]SCHWARZ J K,SIEGEL B A,DEHDASHTI F,et al.Association of posttherapy positron emission tomography with tumor response and survival in cervical carcinoma[J].JAMA,2007,298(19):2289-2295.
[12]GRIGSBY P W,SIEGEL B A,DEHDASHTI F,et al.Posttherapy18F fluorodeoxyglucose positron emission tomography in carcinoma of the cervix:response and outcome[J].J Clin Oncol,2004,22(11):2167-2171.
[13]YOON M S,AHN S J,NAH B S,et al.Metabolic response of lymph nodes immediately after RT is related with survival outcome of patients with pelvic node-positive cervical cancer using consecutive18Ffluorodeoxyglucose-positron emission tomography/computed tomography[J].Int J Radiat Oncol Biol Phys,2012,84(4):e491-497.
[14]ONAL C,GULER O C,REYHAN M,et al.Prognostic value of18F-fluorodeoxyglucose uptake in pelvic lymph nodes in patients with cervical cancer treated with definitive chemoradiotherapy[J].Gynecol Oncol,2015,137(1):40-46.
[15]PARKER K,GALLOP-EVANS E,HANNA L,et al.Five years′ experience treating locally advanced cervical cancer with concurrent chemoradiotherapy and high-dose-rate brachytherapy:results from a single institution[J].Int J Radiat Oncol Biol Phys,2009,74(1):140-146.
[16]OH D,LEE J E,HUH S J,et al.Prognostic significance of tumor response as assessed by sequential18F-fluorodeoxyglucose-positron emission tomography/computed tomography during concurrent chemoradiation therapy for cervical cancer[J].Int J Radiat Oncol Biol Phys,2013,87(3):549-554.
[17]KIDD E A,SIEGEL B A,DEHDASHTI F,et al.The standardized uptake value for F-18 fluorodeoxyglucose is a sensitive predictive biomarker for cervical cancer treatment response and survival[J].Cancer,2007,110(8):1738-1744.
[18]CHUNG H H,CHEON G J,KANG K W,et al.Preoperative PET/CT FDG standardized uptake value of pelvic lymph nodes as a significant prognostic factor in patients with uterine cervical cancer[J].Eur J Nucl Med Mol Imaging,2014,41(4):674-681.
[19]HERRERA F G,PRIOR J O.The role of PET/CT in cervical cancer[J].Front Oncol,2013,3(15):34.
[20]YEN T C,SEE L C,LAI C H,et al.Standardized uptake value in para-aortic lymph nodes is a significant prognostic factor in patients with primary advanced squamous cervical cancer[J].Eur J Nucl Med Mol Imaging,2008,35(3):493-501.
(本文编辑:崔丽红)
Prognostic Value of18F-FDG SUVmax in Pelvic Lymph Nodes Metastases of Patients with Cervical Cancer
ZHAOHong-xia1,DONGYan-shuang1,CAIYou-zhi2,ZHUYing-jun3*
1.DepartmentofObstetricsandGynecology,TianjinForthCenterHospital,Tianjin300143,China2.DepartmentofOrthopedics,theFirstHospitalofZhejiangProvince,Hangzhou310003,China3.DepartmentofObstetricsandGynecology,TianjinCentralHospitalofGynecologyObstetrics,Tianjin300052,China
Background Lymph nodes metastasis is the main factor that affects the prognosis of cervical cancer. Early diagnosis can effectively improve the survival rate of patients with cervical cancer. Objective To evaluate the prognostic value of the18F-FDG maximum standardized uptake value(SUVmax) in pelvic lymph nodes metastases of patients with cervical cancer and analyze the impact factors of survival. Methods A total of 70 cervical carcinoma patients with pelvic and/or paraaortic lymph nodes metastases confirmed by biopsy in Department of Obstetrics and Gynecology of Tianjin Forth Center Hospital were enrolled in this study from December 2004 to August 2011. All patients accepted PET/CT examination and18F-FDG SUVmax was recorded. All patients received radiotherapy and chemotherapy. Patients were followed up when the treatment began. The follow-up ended when patients relapsed or died. The deadline of follow-up was 2015-06-30. Results The AUC of SUVmax for predicting patients′ recurrence was 0.703,95%CI(0.542,0.838),the cut-off value was 7.5,the sensitivity was 85.7%,the specificity was 98.2%,the positive predictive value was 92.3% and the negative predictive value was 96.5%,the Youden index was 0.8. There were 13 cases with SUVmax<7.5 and 57 cases with SUVmax≥7.5. There was no statistically significant differences in overall survival(OS) between patients with SUVmax<7.5 and SUVmax≥7.5(χ2=2.934,P=0.087). The disease-free survival(DFS) of patients with SUVmax<7.5 was higher than that of patients with SUVmax≥7.5(χ2=4.791,P=0.035). Multivariate Cox proportional hazards regression analysis showed that SUVmax,sites of lymph nodes metastases and therapeutic response were the impact factors of OS(P<0.05);SUVmax,sites of lymph nodes metastases and therapeutic response were the impact factors of DFS(P<0.05).Conclusion SUVmax of18F-FDG can be used to well evaluate the prognosis of cervical cancer patients with lymph nodes metastases. The survival rate of patients with cervical cancer is poor when they have higher SUVmax of18F-FDG,pelvic lymph nodes metastases and complete therapeutic response.
Uterine cervical neoplasms;Lymphatic metastasis;Fluorodeoxyglucose F18;Maximum standardized uptake value
国家自然科学青年基金资助项目(81201395)
R 737.33
A
10.3969/j.issn.1007-9572.2017.06.007
2016-08-01;
2016-12-02)
1.300143 天津市第四中心医院妇产科
2.310003 浙江省杭州市,浙江省第一医院骨科
3.300052 天津市中心妇产科医院妇产科
*通信作者:朱颖军,副主任医师;E-mail:zhuyingjun5009@sina.com
*Correspondingauthor:ZHUYing-jun,Associatechiefphysician;E-mail:zhuyingjun5009@sina.com
