应用双腔起搏器频率适应性房室延迟实现双室收缩再同步超应答一例报道并文献复习
2017-02-17赵璐露蒲里津华宝桐
赵璐露,蒲里津,赵 玲,王 钰,华宝桐,郭 涛
·病例研究·
应用双腔起搏器频率适应性房室延迟实现双室收缩再同步超应答一例报道并文献复习
赵璐露,蒲里津,赵 玲,王 钰,华宝桐,郭 涛*
本文报道了1例诊断为扩张型心肌病的患者,通过双腔起搏器单左心室起搏运用频率适应性房室延迟(RAAV)功能实现心脏再同步化治疗(CRT)。通过术后6个月随访,QRS波时限由术前170 ms变窄为术后118 ms,左心室舒张末内径(LVDd)由术前78 mm缩小为术后49 mm,左心室射血分数(LVEF)由术前32%升高为术后48%,心胸比由术前0.64减小为术后0.55,美国纽约心脏病学会(NYHA)心功能分级由术前Ⅲ级降低为术后Ⅰ级,左房室瓣反流面积(MRA)由术前14.0 cm2减少为术后1.8 cm2,左心室12节段达峰时间标准差(TS-SD12)由术前150 ms减少为术后77 ms,主、肺动脉射血时间差(IVMD)由术前47 ms改善为术后33 ms,达到超应答标准。同时结合文献复习,以提高临床医生对双腔起搏器通过RAAV实现双室收缩再同步的认识和应用。
心力衰竭;心脏再同步疗法;双腔起搏器;生理性起搏;频率适应性房室延迟
赵璐露,蒲里津,赵玲,等.应用双腔起搏器频率适应性房室延迟实现双室收缩再同步超应答一例报道并文献复习[J].中国全科医学,2017,20(4):501-503.[www.chinagp.net]
ZHAO L L,PU L J,ZHAO L,et al.Super-response to biventricular systolic resynchronization achieved by dual-chamber pacemaker implantation with rate adaptive atrio-ventricular delay:report of one case and literature review [J].Chinese General Practice,2017,20(4):501-503.
慢性充血性心力衰竭(CHF)患者常合并心内电活动的传导异常,当伴左束支传导阻滞(LBBB)时,左、右心室间收缩不同步,导致室间隔矛盾运动及有效心排血量减少[1]。伴LBBB的CHF患者通常右侧希-浦系传导正常,无需右心室起搏,因此,只要单左心室起搏跟踪右侧固有的房室传导间期,与自身激动融合即可实现心脏再同步化治疗(CRT)。本文报道了1例诊断为扩张型心肌病的患者,通过双腔起搏器单左心室起搏运用频率适应性房室延迟(RAAV)功能实现CRT,达到超应答标准,并结合文献复习,以期提高临床医生对双腔起搏器通过RAAV实现双室收缩再同步的认识和应用。
1 病例简介
患者女,52岁,因“胸闷,气促2年”于2015-05-06入院。患者于2年前活动时出现胸闷、气促,休息症状缓解,并伴有腹胀、恶心,时感咳嗽。入院诊断为扩张型心肌病,左心扩大,窦性心律,美国纽约心脏病学会(NYHA)心功能分级为Ⅲ级。入院后动态心电图(Holter)示:窦性心律,完全性LBBB,60次/min及100次/min的PR间期分别为190 ms及130 ms,QRS波时限为170 ms。胸部X线片示:心外形重度增大,心胸比为0.64(参考值为0.50)。心脏彩超示:左心室舒张末内径(LVDd)为78 mm(参考值为55 mm),左心房内径(LAD)为57 mm(参考值为34 mm),左心室射血分数(LVEF)为32%(参考值为50%),主、肺动脉射血时间差(IVMD)为47 ms,左心室舒张早、晚期快速充盈的充盈峰(EA峰)间距为156 ms,主动脉瓣血流速度时间积分(AVI)为19.3 cm,左心室12节段达峰时间标准差(TS-SD12)为150 ms,左房室瓣反流面积(MRA)为14.0 cm2。符合CRT Ⅰ类适应证,但患者因经济原因不能承担三腔起搏器费用,向患者及其家属告知治疗方案并签署知情同意书后,于2015-05-09成功植入带RAAV功能的双腔起搏器(BIOTRONIK Talos D),按常规方法分别将右心房及左心室电极植入右心耳及左侧后静脉,成功建立右心房+左心室起搏系统,测左心室阈值2.5 V、感知7.0 mV,右心房阈值0.5 V、感知5.5 mV。
术后进行心脏彩超优化时同步描记十二导联心电图,延长房室延迟(AVD),直至腔内图显示心房感知-心室感知(AS-VS),优化时心率为80 次/min,测定PR间期为160 ms,以优化时的PR间期-感知补偿(默认值为30 ms),即以起搏器感知的房室间期(SAV)130 ms为基线进行滴定,每次以10 ms为步长缩短或延长AVD进行“双向滴定”,当SAV为110 ms时,AVI、LVEF最大,MRA最小、心电图上QRS波时限最窄时对应的AVD为优化的AVD,设置起始和终止频率分别为60次/min和100次/min,设置RAAV变化量为:终止频率的PR间期-起始频率的PR间期=130-190=-60(ms),设置起始频率的SAV为:优化的AVD+(起始频率的PR间期-优化时的PR间期)= 110+(190-160)=140(ms)。终止频率的SAV为:优化的AVD-(优化时的PR间期-终止频率的PR间期)=110-(160-130)=80(ms),打开RAAV功能后起搏器程控的AVD动态跟踪右侧房室的生理性AVD实现双室再同步。术后予患者规范的抗心力衰竭药物治疗,病情明显好转。术后6个月随访,QRS波时限为118 ms,LVDd为49 mm,LVEF为48%,心胸比为0.55,NYHA心功能分级为Ⅰ级,MRA为1.8 cm2,TS-SD12为77 ms,IVMD为33 ms,均较术前明显改善,达到超应答标准(见图1~4)。

注:A为术前心电图,CLBBB,QRS波时限为170 ms;B为术后6个月心电图,QRS波时限为118 ms;CLBBB=完全性左束支传导阻滞
图1 患者在植入双腔起搏器术前与术后6个月心电图QRS波比较
Figure 1 Electrocardiogram QRS complexes of the patient before and 6 months after the dual-chamber pacemaker implantation

注:A为术前胸部X线片检查结果,心脏外形明显扩大,心胸比为0.64 ;B为术后6个月胸部X线片检查结果,心脏外形明显缩小,心胸比为0.55
图2 患者在植入双腔起搏器术前与术后6个月胸部X线片检查结果比较
Figure 2 X-ray findings of the patient before and 6 months after the dual-chamber pacemaker implantation
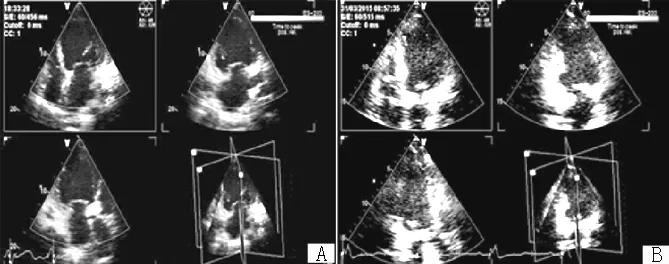
注:A为术前组织同步化显像结果,室间隔、下壁延迟于侧壁;B为术后6个月组织同步化显像结果,左心室同步性良好
图3 患者在植入双腔起搏器术前与术后6个月组织同步化显像结果比较
Figure 3 Tissue synchronization imaging(TSI) results of the patient before and 6 months after the dual-chamber pacemaker implantation
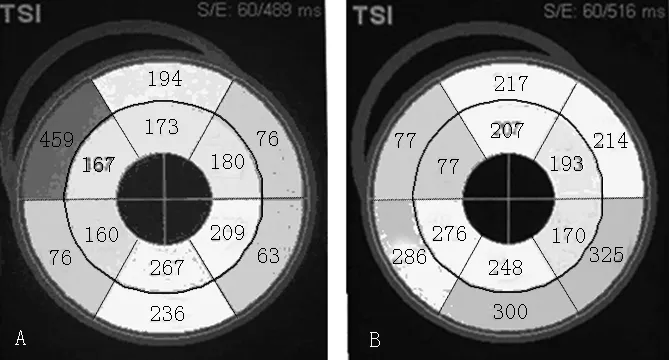
注:A为术前TS-SD12,150 ms;B术后6个月TS-SD12,77 ms;TS-SD12=左心室12节段达峰时间标准差
图4 患者在植入双腔起搏器术前与术后6个月TS-SD12比较
Figure 4 Values of TS-SD12 of the patient before and 6 months after the dual-chamber pacemaker implantation
2 讨论
生理状态下,室上性激动由房室结,经希-浦系快速均匀下传激动双侧心室,生理性AVD受运动、交感张力及心率改变而呈动态变化[2],以协调心房对心室的充盈,在无房室传导阻滞时,自身的PR间期就是最佳AVD,而传统三腔起搏器CRT为保证100%双室起搏,设定短而固定的AVD[3-6],抑制自身激动通过房室结下传心室,废弃了房室结的生理性AVD功能导致左房室瓣和右房室瓣反流、减少心排血量、恶化血流动力学,这有悖于“房室结优先,生理性动态变化的AVD” 的生理性起搏原则[7]。在传统三腔起搏器中,右心室电极起搏后激动经心肌缓慢非均匀逆希浦系传导,激动顺序发生改变后,导致心室的不同步[8],左、右房室瓣反流及左心房扩张,心脏每搏输出量下降,进而心排血量下降;心室的室内分流能引起左心室的横向不良重构,使左心室逐渐发生球形扩张,最终增加心房颤动和心力衰竭的发病率[9],这都可能会抵消CRT的益处。通常伴LBBB的心力衰竭患者,右侧希-浦系统传导正常,右心室无需起搏,对于充血性心力衰竭的患者,尤其在无房室传导阻滞时,应用RAAV功能的起搏器,启动该功能可模仿生理性AVD,提示单左心室起搏通过RAAV功能跟踪生理性AVD与从右侧希-浦系下传的自身激动形成融合波实现双室再同步,实现生理性起搏,同时由于无需右心室耗电起搏,可延长电池寿命,降低CRT费用。
本例患者运用双腔起搏器单左心室起搏实现双室收缩再同步,起搏器程控的左侧AVD通过RAAV算法动态跟踪生理性AVD,与从右侧希-蒲系下传的激动形成融合波,实现CRT。超应答是指CRT术后 6个月患者NYHA心功能分级回退≥1 级或LVEF增加≥20%或绝对值增加≥0.45或左心室收缩末容积(LVESV) 缩小≥15%[10]。本例患者术后6个月随访时,LVEF、QRS波时限、心脏同步性指标、心功能分级等临床评价指标已较术前均有明显改善,达到超应答标准。运用RAAV算法可跟踪运动及交感张力变化导致的生理性AVD变化,更符合生理性。另外,由于三腔起搏器实现CRT费用昂贵,许多患者由于经济原因难以接受三腔起搏器治疗,运用双腔起搏器通过RAAV算法可实现双室收缩再同步,较三腔起搏器实现CRT相比,治疗费用可显著降低,节约有限的医疗资源,更符合我国国情[8]。
作者贡献:赵璐露、蒲里津进行文章的构思与设计、资料收集整理、撰写论文并对文章负责;赵璐露、蒲里津、赵玲、王钰、华宝桐进行文章的可行性分析;郭涛进行质量控制及审校。
本文无利益冲突。
[1]CIAMPI Q,PETRUZZIELLO B,DELLA PORTA M,et al.Effect of intraventricular dyssynchrony on diastolic function and exercise tolerance in patients with heart failure[J].Eur J Echocardiogr,2009,10(8):907-913.
[2]SUN J P,LEE P W,GRIMM R A,et al.Optimisation of atrioventricular delay during exercise improves cardiac output in patients stabilised with cardiac resynchronisation therapy[J].Heart,2012,98(1):54-59.
[3]MANISTY C H,AL-HUSSAINI A,UNSWORTH B,et al.The acute effects of changes to AV delay on BP and stroke volume:potential implications for design of pacemaker optimization protocols[J].Circ Arrhythm Electrophysiol,2012,5(1):122-130.
[4]ELLENBOGEN K A,GOLD M R,MEYER T E,et al.Primary results from the SmartDelay determined AV optimization:a comparison to other AV delay methods used in cardiac resynchronization therapy(SMART-AV) trial:a randomized trial comparing empirical,echocardiography-guided,and algorithmic atrioventricular delay programming in cardiac resynchronization therapy[J].Circulation,2010,122(25):2660-2668.
[5]STEINBERG B A,WEHRENBERG S,JACKSON K P,et al.Atrioventricular and ventricular-to-ventricular programming in patients with cardiac resynchronization therapy:results from ALTITUDE[J].J Interv Card Electrophysiol,2015,44(3):279-287.
[6]GRAS D,GUPTA M S,BOULOGNE E,et al.Optimization of AV and VV delays in the real-world CRT patient population:an international survey on current clinical practice[J].Pacing Clin Electrophysiol,2009,32(Suppl 1):S236-239.
[7] 郭涛,蒲里津,李锐洁.心脏再同步化治疗无应答的原因与对策[J].中国心脏起搏与心电生理杂志,2014,28(1):1-4. GUO T,PU L J,LI R J.Reasons and countermeasures of non - response in cardiac resynchronization therapy [J].Chinese Journal of Cardiac Pacing and Electrophysiology,2014,28(1):1-4.
[8]郭涛,蒲里津.双室起搏新思路[M].北京:人民卫生出版社,2013:377. GUO T,PU L J.New idea of biventricular pacing[M].Beijing:People′s Medical Publishing House,2013:377.
[9]HOUTHUIZEN P,BRACKE F A,VAN GELDER B M.Atrioventricular and interventricular delay optimization in cardiac resynchronization therapy:physiological principles and overview of available methods[J].Heart Fail Rev,2011,16(3):263-276.
[10]RICKARD J,KUMBHANI D J,POPOVIC Z,et al.Characterization of super-response to cardic resynchronization therapy[J].Heart Rhythm,2010,7(7):885-889.
(本文编辑:崔沙沙)
Super-response to Biventricular Systolic Resynchronization Achieved by Dual-chamber Pacemaker Implantation with Rate Adaptive Atrio-ventricular Delay:Report of One Case and Literature Review
ZHAOLu-lu,PULi-jin,ZHAOLing,WANGYu,HUABao-tong,GUOTao*
DepartmentofCardiology,FirstAffiliatedHospitalofKunmingMedicalUniversity/YunnanInstituteofCardiovascularDiseases,Kunming650032,China
This article reported the positive treatment outcome of 1 patient diagnosed with dilated cardiomyopathy achieved by cardiac resynchronization therapy(CRT) via left ventricular pacing with dual-chamber pacemaker implantation and rate adaptive atrio-ventricular(RAAV) delay.The results of 6-month follow-up showed that the general conditions of the patient were significantly improved,and a super-response to biventricular systolic resynchronization was achieved,which mainly manifested in the following:QRS complexes duration was shortened from 170 ms to 118 ms,left ventricular end-diastolic diameter(LVDd) was decreased from 78 mm to 49 mm,left ventricular ejection fraction(LVEF) was increased from 32% to 48%,the cardiothoracic ratio value was decreased from 0.64 to 0.55,New York Heart Association(NYHA) cardiac functional grading was reduced from level Ⅲ to level Ⅰ,the mitral valve regurgitation area(MRA) was decreased from 14.0 cm2to 1.8 cm2,the standard deviation of the time to regional peak systolic velocity of the 12 left ventricular segments(TS-SD12) was decreased from 150 ms to 77 ms,the interventricular mechanical delay(IVMD) was decreased from 47 ms to 33 ms.Meanwhile,the corresponding literature was reviewed,all in order to improve the clinical understanding and application of using the dual-chamber pacemaker with RAAV to achieve CRT.
Heart failure;Cardiac resynchronization therapy;Dual-chamber pacemaker;Physiological pacing;Rate adaptive atrio-ventricular delay
国家自然科学基金资助项目(81360044);云南省科技厅-昆明医科大学联合专项基金资助项目(2013FB133)
R 541
D
10.3969/j.issn.1007-9572.2017.04.024
2016-07-08;
2016-12-14)
650032云南省昆明市,昆明医科大学第一附属医院心内科 云南省心血管病研究所
*通信作者:郭涛,教授,博士生导师;E-mail:guotao20@hotmail.com
*Correspondingauthor:GUOTao,Professor,Doctoralsupervisor;E-mail:guotao20@hotmail.com
