多种肿瘤标志物在胰腺癌中的诊断价值及相关性研究
2017-02-15林文科吴吉芳郑志昂
林文科 吴吉芳 郑志昂
(海南省第三人民医院检验科,三亚572000)
多种肿瘤标志物在胰腺癌中的诊断价值及相关性研究
林文科 吴吉芳 郑志昂
(海南省第三人民医院检验科,三亚572000)
目的:探讨血清肿瘤标志物联合检测对胰腺癌的诊断价值及相关性。方法:选取2013年1月至2016年5月我院胰腺癌患者146例,非胰腺癌患者128例和健康体检者124例,放射免疫分析仪检测各组血清CA19-9、CA242、CA50、CA125、CEA及TSGF水平,并进行各组间比较。绘制受试工作特征曲线(ROC)分析各肿瘤标志物在胰腺癌患者中的诊断价值,线性相关分析各肿瘤标志物的相关性。应用多元Logistic回归模型分析胰腺癌的独立危险因素。结果:胰腺癌组血清CA19-9、CA242、CA50、CA125、CEA及TSGF水平明显高于对照组和非胰腺癌组,差异有统计学意义(P<0.05或P<0.01)。Ⅳ期和Ⅲ期患者血清CA19-9、CA242、CA50、CA125及TSGF水平明显高于Ⅰ期和Ⅱ期(P<0.01),且Ⅳ期患者血清CA19-9、CA242、CA125及CEA水平明显高于Ⅲ期(P<0.01)。胰腺癌组血清CA19-9、CA242、CA50、CA125、CEA及TSGF的阳性率明显高于对照组和非胰腺癌组(P<0.01)。ROC曲线显示,血清CA19-9的AUC高于其他单项指标,其最佳临界值、灵敏度和特异度分别为114.5 U/ml、81.2%和79.3%。6项联合检测的诊断效能均优于各单项检测,其灵敏度和特异度分别为92.4%和76.5%。相关性分析显示,血清CA19-9与CA242、CA50及CA125均呈正相关(r=0.703,P=0.005;r=0.572,P=0.024;r=0.439,P=0.036)。多元Logistic回归分析显示,吸烟、不正确的饮食习惯、糖尿病史、胆系疾病史及CA19-9、CA242、CEA进入回归模型,其OR值及95%CI分别为1.717(0.736~2.359)、2.865(2.217~3.685)、2.614(2.186~3.127)、3.527(2.842~4.377)、4.214(3.570~4.962)、2.315(2.114~2.539)、1.876(1.175~2.852)。结论:血清肿瘤标志物联合检测有助于提高早期胰腺癌诊断的准确性,吸烟、不正确的饮食习惯、糖尿病史、胆系疾病史及高水平的CA19-9、CA242、CEA是胰腺癌的独立危险因素。
胰腺癌;肿瘤标志物;ROC曲线;相关性
胰腺癌(Pancreatic cancer,PC)是一种恶性程度极高、预后极差的消化道常见肿瘤,近来其发病率和死亡率呈逐年上升趋势,已成为危及人类的生命健康的主要原因之一。由于胰腺癌患者早期缺乏典型的临床表现,肿瘤呈进行性生长并较早发生转移,使得临床上90%以上的患者确诊为胰腺癌时常属于中晚期,失去了治疗的最佳时机,5年生存率仅为5%[1]。因此,胰腺癌的早期发现、早期诊断、早期治疗是降低患者死亡率和提高患者生活质量的关键。目前探索特异性的早期诊断肿瘤标志物,实现对胰腺癌的早期诊断是近年来研究的热点[2-4]。本研究通过检测胰腺癌患者糖类抗原19-9(CA19-9)、糖类抗原242(CA242)、糖类抗原50(CA50)、糖类抗原125(CA125)、癌胚抗原(CEA)及肿瘤特异生长因子(TSGF)的表达情况,探讨各肿瘤标志物在胰腺癌中的诊断价值及相关性。
1 资料与方法
1.1 资料
1.1.1 研究对象 选取2013年1月至2016年5月我院收治的胰腺癌患者146例,男95例,女51例,年龄36~78岁,平均(56.27±10.48)岁。所有患者均经病理学、影像学和细胞诊断学明确诊断。根据国际抗癌联盟(Union for International Cancer Control,UICC)标准胰腺癌分期:Ⅰ期32例、Ⅱ期37例、Ⅲ期33例及Ⅳ期44例。另选择同期住院的128例良性胰腺病患者(包括慢性胰腺炎、胰腺囊肿等)作为非胰腺癌组,男77例,女51例,年龄29~81岁,平均(55.18±12.06)岁;124例我院健康体检者作为正常对照组,其中男78例,女46例,年龄32~75,平均(54.72±10.53)岁。所有研究对象均排除消化系统疾病、胃肠肿瘤、肝功能不全及精神障碍患者。本研究经医院伦理委员会批准,并获得患者或家属签署知情同意书。
1.1.2 主要仪器和试剂 使用Maglumi2000plus全自动化学发光分析仪检测血清CA19-9、CA242、CA50、CA125、CEA水平和贝克曼DX1800生化分析仪检测TSGF、肝功能等生化指标,所用试剂盒、校准品及质控品均由深圳市新产业生物医学工程股份有限公司和美国贝克曼库尔特有限公司提供的配套产品。将各肿瘤标志物测定结果的正常值上限作为阳性界值,阳性判断标准为:CA19-9>35 U/ml,CA242>20 U/ml,CA50>35 U/ml,CA125>35 U/ml,CEA>6 ng/ml,TSGF>65 U/ml。
1.2 方法 所有研究对象均于清晨空腹静脉采血,取静脉血5 ml,注入肝素抗凝的试管中混匀,以离心半径13.5 cm,3 500 r/min离心5 min,分离血清后采用放射免疫法检测血清CA19-9、CA242、CA50、CA125、CEA水平和生化定量分析法检测TSGF水平。整个操作过程均严格按照SOP文件进行。

2 结果
2.1 各组血清肿瘤标志物水平比较 胰腺癌组血清CA19-9、CA242、CA50、CA125、CEA及TSGF水平明显高于对照组和非胰腺癌组,差异有统计学意义(P<0.05或P<0.01)。非胰腺癌组血清CA19-9、CA242及CEA水平明显高于对照组,差异有统计学意义(P<0.05或P<0.01)。见表1。
2.2 胰腺癌患者各期血清CA19-9、CA242、CA50、CA125、CEA及TSGF水平比较 Ⅳ期和Ⅲ期患者血清CA19-9、CA242、CA50、CA125及TSGF水平明显高于Ⅰ期和Ⅱ期,差异有统计学意义(P<0.01)。Ⅳ期患者血清CA19-9、CA242、CA125及CEA水平明显高于Ⅲ期,差异有统计学意义(P<0.01)。Ⅱ期患者血清CA19-9水平明显高于Ⅰ期,差异有统计学意义(P<0.01);而Ⅱ期与Ⅰ期血清CA242、CA50、CA125、CEA及TSGF水平比较,差异无统计学意义(P>0.05)。见表2。
2.3 各组血清CA19-9、CA242、CA50、CA125、CEA及TSGF阳性率比较 胰腺癌组和非胰腺癌组血清CA19-9、CA242、CA50、CA125、CEA及TSGF的阳性率明显高于对照组,差异有统计学意义(P<0.01)。胰腺癌组血清CA19-9、CA242、CA50、CA125、CEA及TSGF的阳性率明显高于非胰腺癌组,差异有统计学意义(P<0.01)。见表3。



GroupsCasesCA19⁃9(U/ml)CA242(U/ml)CA50(U/ml)CA125(U/ml)CEA(ng/ml)TSGF(U/ml)Controlgroup1241246±417956±437746±128968±514325±0864872±1063Nonpancreaticcancergroup1284285±13262)1751±8201)1124±3651287±643618±1631)5194±1227Pancreaticcancergroup14617843±46392)4)6647±12932)4)5538±20142)4)5184±18622)4)1234±5622)3)8546±18292)4)F3218614827112161087458418573P000000000000000000170001
Note:Compared with the control group,1)P<0.05 or 2)P<0.01;compared with non pancreatic cancer group,3)P<0.05 or 4)P<0.01.


EachstageCasesCA19⁃9(U/ml)CA242(U/ml)CA50(U/ml)CA125(U/ml)CEA(ng/ml)TSGF(U/ml)Ⅰstage3210457±17242634±5272846±9173186±1242728±2066274±1250Ⅱstage3713286±25411)3218±7033725±9543647±1238914±2376892±1246Ⅲstage3317316±30531)2)6893±15841)2)6172±19351)2)4906±20451)2)1053±3629347±19611)2)Ⅳstage4420548±38651)2)3)8056±19121)2)3)6826±24381)2)6570±23871)2)3)1758±6731)2)3)9682±21731)2)F18483118279185989376145692P000000000001000000050018
Note:Compared with Ⅰstage,1)P<0.01;compared with Ⅱstage,2)P<0.01;compared with Ⅲstage,3)P<0.01.
表3 各组血清CA19-9、CA242、CA50、CA125、CEA及TSGF阳性率比较[n(%)]
Tab.3 Comparison of positive rate of CA19-9,CA242,CA50,CA125,CEA and TSGF in each group[n(%)]
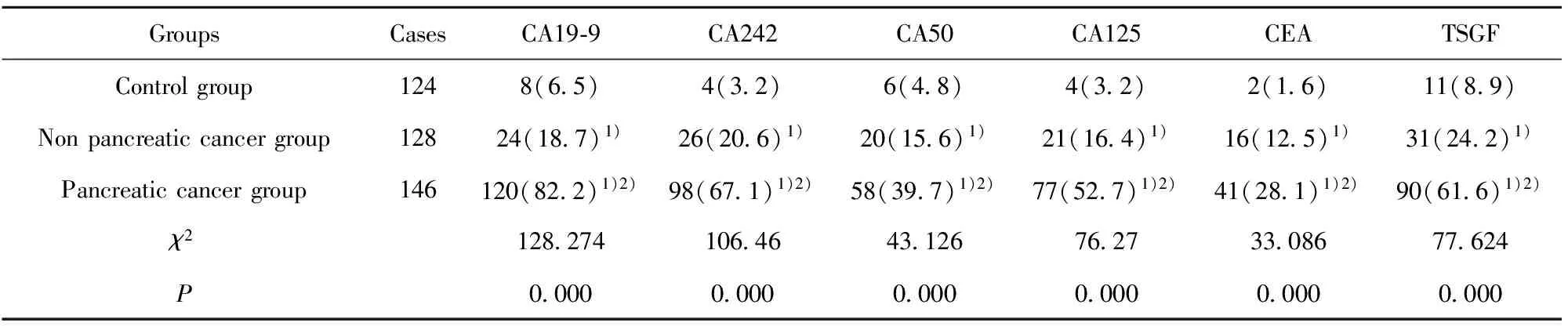
GroupsCasesCA19⁃9CA242CA50CA125CEATSGFControlgroup1248(65)4(32)6(48)4(32)2(16)11(89)Nonpancreaticcancergroup12824(187)1)26(206)1)20(156)1)21(164)1)16(125)1)31(242)1)Pancreaticcancergroup146120(822)1)2)98(671)1)2)58(397)1)2)77(527)1)2)41(281)1)2)90(616)1)2)χ2128274106464312676273308677624P000000000000000000000000
Note:Compared with the control group,1)P<0.01;compared with non pancreatic cancer group,2)P<0.01.
表4 ROC曲线分析各肿瘤标志物对胰腺癌的诊断价值
Tab.4 Diagnostic value of tumor markers in pancreatic cancer by ROC curve analysis
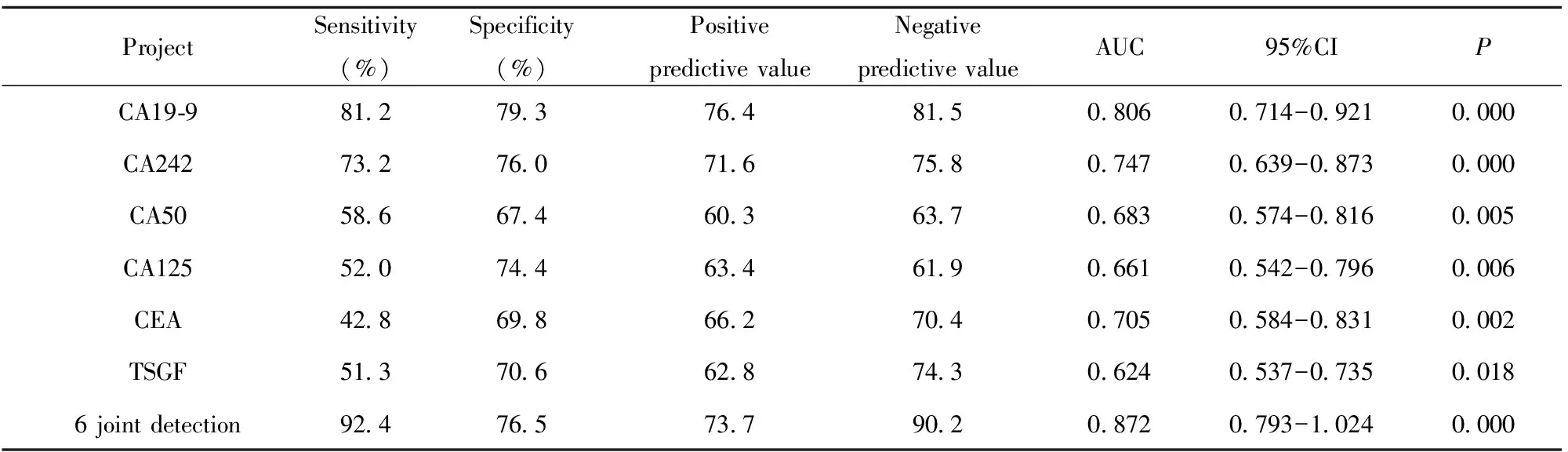
ProjectSensitivity(%)Specificity(%)PositivepredictivevalueNegativepredictivevalueAUC95%CIPCA19⁃981279376481508060714-09210000CA24273276071675807470639-08730000CA5058667460363706830574-08160005CA12552074463461906610542-07960006CEA42869866270407050584-08310002TSGF51370662874306240537-073500186jointdetection92476573790208720793-10240000
表5 多元Logistic回归分析胰腺癌的独立危险因素
Tab.5 Multivariate Logistic regression analysis of independent risk factors for pancreatic cancer

VariableRegressioncoefficientStandarderrorWaldvalueORvalue95%CIPSmoking06040376563117170736-23590019Incorrectdiet14280532678428652217-36850008Historyofdiabetes21670719541626142186-31270021Gallbladderdiseasehistory170304851587335272842-43770000CA19⁃9152105581370642143570-49620000CA24208160447901423152114-25390000CEA11480603652818761175-28520007

图1 各肿瘤标志物在胰腺癌诊断中的ROC曲线Fig.1 ROC curves of tumor markers in diagnosis of pancreatic cancer
2.4 ROC曲线分析各肿瘤标志物对胰腺癌的诊断价值 血清CA19-9、CA242、CA50、CA125、CEA、TSGF及联合检测在胰腺癌诊断中的AUC分别为:0.806、0.747、0.683、0.661、0.705、0.624、0.872,与对照组(AUC=0.5)比较,差异均有统计学意义(P<0.05),见图1。单项检测中,血清CA19-9的AUC高于其他单项指标,其最佳临界值、灵敏度和特异度分别为114.5 U/ml、81.2%和79.3%。6项联合检测的诊断效能均优于各单项检测,其灵敏度和特异度分别为92.4%和76.5%。见表4。
2.5 胰腺癌患者血清CA19-9与CA242、CA50、CA125、CEA及TSGF的相关性分析 血清CA19-9与CA242、CA50及CA125均呈正相关(r=0.703,P=0.005;r=0.572,P=0.024;r=0.439,P=0.036),而血清CA19-9与CEA及TSGF无明显相关性(P>0.05)。血清CA19-9与CA242的相关性最好,其线性回归方程为y=0.773 5x+1.386 2,见图2。
2.6 多元Logistic回归分析胰腺癌的独立危险因素以有或无胰腺癌为因变量,以年龄(>50或≤50岁)、性别(男或女)、体质指数(>30或≤30 kg/m2)、吸烟(有或无)、不正确的饮食习惯(有或无)、高血压史(有或无)、糖尿病史(有或无)、肿瘤家族史(有或无)、胆系疾病史(有或无)、CA19-9、CA242、CA50、CA125、CEA及TSGF为自变量,按α=0.05水平进行多元Logistic回归分析,发现吸烟、不正确的饮食习惯、糖尿病史、胆系疾病史及高水平的CA19-9、CA242、CEA是胰腺癌的独立危险因素。见表5。

图2 胰腺癌患者血清CA19-9与CA242的相关性Fig.2 Correlation between serum CA19-9 and CA242 in patients with pancreatic cancer
3 讨论
胰腺癌是临床上常见的恶性肿瘤之一,其缺乏有效的早期诊断手段,使得患者化疗和放疗的效果较差,外科切除率和总体生存率较低。血清肿瘤标志物是指肿瘤组织在其发生、发展过程中分泌的物质,可反映早期肿瘤的存在,在恶性肿瘤患者中呈高表达,而正常组织或良性病变中表达甚微[5,6]。因此,研究血清肿瘤标志物与胰腺癌患者的相关性对早期诊断胰腺癌具有重要意义。
CA19-9是一种黏蛋白型糖类肿瘤标志物,多种肿瘤组织、正常胰腺和胃肠道黏膜均可表达。因胰腺癌可致胰管机械性梗阻、胰腺细胞的极性消失和血管早期受侵,故胰腺癌中CA19-9呈高表达,在良性疾病或正常人群中表达较低。研究证实,CA19-9是检测胰腺癌敏感性较高的指标,但其在多种消化道肿瘤如胆囊癌、胃癌、肠癌等中也有不同程度的升高,故被称为胃肠癌相关抗原[7]。CA242是唾液酸化的糖脂类抗原,主要存在于胰腺和结肠恶性肿瘤细胞中,在胰腺癌中常有高表达,其中以胰头癌时表达最高,是筛选胰腺癌的标志物[8]。
CA50是一种高分子糖蛋白,广泛存在于上皮组织肿瘤中,属于广谱性肿瘤标志物[9]。CA125主要用于辅助诊断恶性浆液性卵巢癌、上皮性卵巢癌,但在消化系统肿瘤(胃癌、结直肠癌、胰腺癌)患者中也有升高[10]。CEA是细胞表面糖蛋白家族成员,研究发现其与胰腺癌发生、发展相关,但其敏感性和特异性不高,一般多与其他指标联合检测以提高其诊断的准确性[11]。TSGF是恶性肿瘤及其周边毛细血管扩增所产生的一类多肽物质,与肿瘤生长密切相关,对恶性肿瘤具有广谱性、较高敏感性及特异性[12]。
本研究结果显示,血清CA19-9、CA242及CEA水平在良性胰腺病患者中升高,胰腺癌患者血清CA19-9、CA242、CA50、CA125、CEA及TSGF水平升高更明显,而正常对照组各肿瘤标志物表达水平较低。说明血清肿瘤标志物对胰腺癌的早期诊断具有一定的临床价值。Wang等[13]研究报道,胰腺癌患者血清CA125、CA19-9浓度显著高于良性胰腺疾病。Chen等[14]研究表明,血清CA242、CA199、CA125、CEA和TSGF水平对胰腺癌患者的诊断和预后评估具有重要的临床价值。随着胰腺癌分期越高患者血清CA19-9、CA242、CA50、CA125、CEA及TSGF水平升高越明显,提示可根据肿瘤标志物的表达水平来评估胰腺癌患者的预后。在Ⅰ期胰腺癌患者血清中,CA50、CA125及TSGF的表达水平仍在正常范围内。如果单一地将它们作为胰腺癌的诊断依据,明显会造成胰腺癌的漏诊率。因此,对于胰腺癌的早期诊断应联合多项肿瘤学标志物。胰腺癌组血清CA19-9、CA242、CA50、CA125、CEA及TSGF的阳性率明显高于对照组和非胰腺癌组。胰腺癌患者以CA19-9的阳性率最高为82.2%,其次为CA242(67.1%)和TSGF(61.6%),且CA19-9、CA242和TSGF在非胰腺癌组和对照组中阳性率较低,故其可作为检测胰腺癌变的主要指标。尽管CA125主要用于卵巢癌的诊断,但本研究CA125在胰腺癌中的阳性率达52.7%,提示胰腺癌患者也可高表达CA125。CA50和CEA在胰腺癌中的阳性率仅为39.7%和28.1%,消化道各种肿瘤的发生也可导致CA50和CEA明显上升,其特异性差,故单独检测CA50或CEA对胰腺癌的诊断意义不大。我们进一步采用ROC曲线分析,结果显示血清CA19-9、CA242、CA50、CA125、CEA、TSGF及联合检测在胰腺癌诊断中的AUC均明显高于对照组(AUC=0.5)。单项检测中,血清CA19-9的诊断效能最好,其灵敏度和特异度分别为81.2%和79.3%。6项联合检测的诊断效能均优于各单项检测,其灵敏度和特异度分别为92.4%和76.5%。既往研究表明,CA19-9诊断胰腺癌的敏感度为71%~95%和特异度为70%~81%,其敏感度较强,但特异度略低[15,16]。Gu等[17]研究表明,血清肿瘤标志物(CA19-9,CEA,CA125和CA242)联合检测有助于提高胰腺癌的诊断效率。Zhang等[18]研究显示,CA19-9诊断胰腺癌的特异性优于CEA,其用于诊断胰腺癌的敏感性和特异性分别达到80.0%和86.0%。相关性分析显示,血清CA19-9与CA242、CA50及CA125均呈正相关,其中血清CA19-9与CA242的相关性最好(r=0.703,P=0.005)。这进一步说明各肿瘤标志物之间存在良好的相关性,联合检测有利于提高胰腺癌的检出率。多元Logistic回归分析,发现吸烟、不正确的饮食习惯、糖尿病史、胆系疾病史及高水平的CA19-9、CA242、CEA是胰腺癌的独立危险因素。美国进行了一项以人口和家庭为基础的关于环境、遗传与胰腺癌的危险因素研究,发现吸烟是胰腺癌最常见的危险因素[19]。Lee等[20]研究发现,CA19-9和CEA是胰腺癌的影响因素,对胰腺癌患者预后评估有重要的临床意义。
综上所述,血清CA19-9、CA242、CA50、CA125、CEA及TSGF单独检测某一标记物对胰腺癌的早期确诊率不高,联合检测可提高胰腺癌的检出率,弥补单一检测的不足。了解胰腺癌的危险因素并针对胰腺癌的高危人群进行监测,可准确评估高危个体患胰腺癌的风险,从而达到胰腺癌的早期诊断及早期治疗。
[1] Siegel R,Ward E,Brawley O,etal.Cancer statistics,2011:the impact of eliminating socioeconomic and racial disparities on premature cancer deaths[J].CA Cancer J Clin,2011,61(4):212-236.
[2] Bertsch T,Aschenneller C,Bewarder N,etal.European proficiency study with control serum for the tumor marker CA 19-9 measured on different test systems[J].Clin Lab,2013,59(1-2):185-192.
[3] Al-Shamsi HO,Alzahrani M,Wolff RA.The clinical utility of normal range carbohydrate antigen 19-9 level as a surrogate marker in evaluating response to treatment in pancreatic cancer-a report of two cases[J].J Gastrointest Oncol,2016,7(3):E45-51.
[4] Dranka-Bojarowska D,Lekstan A,Olakowski M,etal.The assessment of serum concentration of adiponectin,leptin and serum carbohydrate antigen-19.9 in patients with pancreatic cancer and chronic pancreatitis[J].J Physiol Pharmacol,2015,66(5):653-663.
[5] Chen JM,Gao HY,Wang Q,etal.Expression and clinical significance of tumor markers in ovarian mature cystic teratoma[J].Clin Exp Obstet Gynecol,2016,43(3):397-400.
[6] D′Onofrio M,Barbi E,Girelli R,etal.Variation of tumoral marker after radiofrequency ablation of pancreatic adenocarcinoma[J].J Gastrointest Oncol,2016,7(2):213-220.
[7] Huang ZB,Zhou X,Xu J,etal.Prognostic value of preoperative serum tumor markers in gastric cancer[J].World J Clin Oncol,2014,5(2):170-176.
[8] Zhou G,Niu L,Chiu D,etal.Changes in the expression of serum markers CA242,CA199,CA125,CEA,TNF-α and TSGF after cryosurgery in pancreatic cancer patients[J].Biotechnol Lett,2012,34(7):1235-1241.
[9] Xie M,Huang H,Hang J,etal.Evaluation of the analytical and clinical performances of time-resolved fluoroimmunoassay for detecting carcinoma antigen 50[J].J Immunoassay Immunochem,2015,36(3):265-283.
[10] Liu L,Xu HX,Wang WQ,etal.Serum CA125 is a novel predictive marker for pancreatic cancer metastasis and correlates with the metastasis-associated burden[J].Oncotarget,2016,7(5):5943-5956.
[11] Wu L,Huang P,Wang F,etal.Relationship between serum CA19-9 and CEA levels and prognosis of pancreatic cancer[J].Ann Transl Med,2015,3(21):328.
[12] Yin LK,Sun XQ,Mou DZ.Value of combined detection of serum CEA,CA72-4,CA19-9 and TSGF in the diagnosis of gastric cancer[J].Asian Pac J Cancer Prev,2015,6(9):3867-3870.
[13] Wang Z,Tian YP.Clinical value of serum tumor markers CA19-9,CA125 and CA72-4 in the diagnosis of pancreatic carcinoma[J].Mol Clin Oncol,2014,2(2):265-268.
[14] Chen Y,Gao SG,Chen JM,etal.Serum CA242,CA199,CA125,CEA,and TSGF are biomarkers for the efficacy and prognosis of cryoablation in pancreatic cancer patients[J].Cell Biochem Biophys,2015,71(3):1287-1291.
[15] Yang XQ,Chen C,Peng CW,etal.Carbohydrate antigen 242 highly consists with carbohydrate antigen 19-9 in diagnosis and prognosis of colorectal cancer:study on 185 cases[J].Med Oncol,2012,29(2):1030-1036.
[16] Zhang Y,Yang J,Li H,etal.Tumor markers CA19-9,CA242 and CEA in the diagnosis of pancreatic cancer:a meta-analysis[J].Int J Clin Exp Med,2015,8(7):11683-11691.
[17] Gu YL,Lan C,Pei H,etal.Applicative value of serum CA19-9,CEA,CA125 and CA242 in diagnosis and prognosis for patients with pancreatic cancer treated by concurrent chemoradiotherapy[J].Asian Pac J Cancer Prev,2015,16(15):6569-6573.
[18] Zhang Y,Jiang L,Song L.Meta-analysis of diagnostic value of serum Carbohydrate antigen 199 in pancreatic cancer[J]. Minerva Med,2016,107(1):62-69.
[19] Bosetti C,Lucenteforte E,Silverman DT,etal.Cigarette smoking and pancreatic cancer:an analysis from the international pancreatic cancer case-control consortium(Panc4)[J].Ann Oncol,2012,23(7):1880-1888.
[20] Lee KJ,Yi SW,Chung MJ,etal.Serum CA 19-9 and CEA levels as a prognostic factor in pancreatic adenocarcinoma[J].Yonsei Med J,2013,54(3):643-649.
[收稿2016-07-16 修回2016-08-25]
(编辑 许四平)
Diagnostic value and correlation of multiple tumor markers in pancreatic cancer
LINWen-Ke,WUJi-Fang,ZHENGZhi-Ang.
DepartmentofClinicalLaboratory,ThirdPeople′sHospitalofHainanProvince,Sanya572000,China
Objective:To explore the diagnostic value and correlation of serum tumor markers combined detection of pancreatic cancer.Methods: Selected January 2013 to may 2016 in our hospital in patients with pancreatic cancer in 146 cases,128 cases of non pancreatic cancer with patients and 124 cases of healthy physical examination.Radiation immunity analyzer test groups of serum CA19-9,CA242,CA50,CA125,CEA and TSGF levels and compared between groups.To draw the working characteristic curve(ROC)to analyze the diagnostic value of tumor markers in patients with pancreatic cancer and the correlation of linear correlation analysis of tumor markers.Analysis of independent risk factors for pancreatic cancer using multiple logistic regression models.Results: The pancreatic cancer group of serum CA19-9,CA242,CA50,CA125,CEA and TSGF levels were significantly higher than the control group and non pancreatic cancer group,the differences were statistically significant(P<0.05 orP<0.01).Ⅳ stage and Ⅲ stage with patients of serum CA19-9,CA242,CA50,CA125 and TSGF levels were significantly higher than Ⅰstage and Ⅱstage with patients(P<0.01).Ⅳ stage with patients of serum CA19-9,CA242,CA125 and CEA levels were significantly higher than Ⅲ stage with patients(P<0.01).The pancreatic cancer group of serum CA19-9,CA242,CA50,CA125,CEA and TSGF of positive rate were significantly higher than that of control group and non pancreatic cancer group(P<0.01).ROC curves showed that the AUC of serum CA19-9 were higher than other single indexes,the best critical value,sensitivity and specificity were 114.5 U/ml,81.2% and 79.3% respectively.The diagnostic efficacy of the six joint detection were better than the single detection,the sensitivity and specificity were 92.4% and 76.5% respectively.Correlation analysis showed that serum CA19-9 were positively correlated with CA242,CA50 and CA125(r=0.703,P=0.005;r=0.572,P=0.024;r=0.439,P=0.036).Multiple logistic regression analysis showed that smoking,incorrect diet,history of diabetes,gallbladder disease history and high levels of CA19-9,CA242,CEA into the regression model,the OR value and 95%CI were 1.717(0.736 to 2.359),2.865(2.217 to 3.685),2.614(2.186 to 3.127),3.527(2.842 to 4.377),4.214(3.570 to 4.962),2.315(2.114 to 2.539),1.876(1.175 to 2.852).Conclusion: Serum tumor markers combined detection can help to improve the accuracy of early diagnosis of pancreatic cancer and smoking,incorrect diet habits,history of diabetes,biliary disease history and high levels of CA19-9,CA242 and CEA are independent risk factors for pancreatic cancer.
Pancreatic cancer;Tumor marker;ROC curve;Correlation
10.3969/j.issn.1000-484X.2017.01.025
林文科(1982年-),男,主管检验师,主要从事临床放射免疫检验学研究,E-mail:415004372@qq.com。
R446.6
A
1000-484X(2017)01-0120-06
