经皮冠状动脉介入治疗后患者社区管理效果研究
2016-12-27黄冠华闫旭龙王增帅
黄冠华,闫旭龙,王增帅,闫 红
·论著·
经皮冠状动脉介入治疗后患者社区管理效果研究
黄冠华,闫旭龙,王增帅,闫 红
目的 探讨经皮冠状动脉介入治疗(PCI)后适宜的社区管理模式及管理效果,提高社区医生对冠心病患者PCI后不良心血管事件的防治能力,减少其危险因素。方法 选择2014年在包头医学院第二附属医院心内科诊治的符合入选标准的PCI后患者87例,其中回到社区接受社区医生管理者为干预组(47例),无法回到社区接受社区医生管理者为对照组(40例)。项目专家组成员接受原卫生部心血管病防治研究中心的培训后,再对具体管理干预组患者的社区医生进行培训。社区医生对干预组患者进行管理,对照组患者不予任何管理。项目专家组成员在两组患者PCI后6、12个月时进行电话随访,记录两组患者心血管病危险因素、服药情况,评估患者生活方式、主要不良心血管事件。结果 PCI后6、12个月时,干预组体质指数(BMI)、收缩压(SBP)和三酰甘油(TG)均较对照组下降(P<0.05)。PCI后6个月时,两组钙离子拮抗剂(CCB)、硝酸盐类药物服药率比较,差异均有统计学意义(P<0.05);PCI后12个月时,两组CCB、β-受体阻滞剂、他汀类药物服药率比较,差异均有统计学意义(P<0.05)。Logistic回归分析显示,组别是PCI后6个月睡眠、烦躁、抑郁的影响因素,组别是PCI后12个月规律运动>2次/周并>30 min/次、吃快餐次数>3次/周、饮酒<22 g/次、睡眠的影响因素(P<0.05)。PCI后6个月时,两组心肌梗死发生率比较,差异有统计学意义(P<0.05);PCI后12个月时,两组心肌梗死、靶目标血运重建(TLR)发生率比较,差异有统计学意义(P<0.05)。结论 以社区为单位开展PCI后建档管理,有利于冠心病的二级预防。社区医生对PCI后患者的有效管理可以减少不良心血管事件及其危险因素。
血管成形术,气囊,冠状动脉;社区健康教育;主要不良心血管事件;心血管疾病;危险因素
黄冠华,闫旭龙,王增帅,等.经皮冠状动脉介入治疗后患者社区管理效果研究[J].中国全科医学,2016,19(33):4061-4066.[www.chinagp.net]
HUANG G H,YAN X L,WANG Z S,et al.Effect of community management of patients after PCI on cardiovascular events and risk factors[J].Chinese General Practice,2016,19(33):4061-4066.
我国经皮冠状动脉介入治疗(PCI)始于1984年[1],是冠心病的主要治疗手段。越来越多的冠心病患者接受了PCI[2]。行PCI出院后,绝大部分患者不知道该怎样调理自己的身体,美国和欧洲发达国家已经开展了对冠心病等心血管疾病的社区干预[3-6]。目前,我国部分城市已经实现了PCI患者出院后回到社区接受社区全科医生的照顾与管理[7-8]。但PCI后的社区管理对心血管不良事件及危险因素的影响如何,国内报道较少。本研究旨在探讨适宜的社区管理模式对PCI后患者不良心血管事件及危险因素的防治效果。
1 资料与方法
1.1 入选与排除标准 入选标准:成功行PCI的冠心病患者;年龄>18周岁;同意参与本研究。排除标准:合并恶性肿瘤、严重呼吸系统疾病或自身免疫性疾病者;肝、肾功能不全者;无自理能力者。
1.2 临床资料 选择2014年在包头医学院第二附属医院心内科诊治的符合入选标准的PCI后患者87例,其中回到社区接受社区医生管理者为干预组(47例),无法回到社区接受社区医生管理者为对照组(40例)。对照组男24例、女16例,平均年龄(63.0±8.8)岁;干预组男27例、女20例,平均年龄(64.0±7.8)岁;两组患者的性别构成和年龄间差异均无统计学意义(χ2=0.058,P=0.810;t=-0.147,P=0.890)。
1.3 干预方法
1.3.1 对照组 在患者PCI后6、12个月时由项目专家组成员进行电话随访,社区医生不予任何干预。
1.3.2 干预组
1.3.2.1 社区医生培训 项目专家组成员接受原卫生部心血管病防治研究中心的培训后,再对具体管理PCI后患者的社区医生进行培训。采用《2013年中华医学会冠心病康复与二级预防中国专家共识》[9]作为规范化培训教材,在技术层面进行统一培训。确保患者得到安全和有效的治疗,PCI后患者回归社区,出现如下情况时应及时由社区医生转诊至上级医院治疗:(1)心绞痛;(2)可疑心肌梗死;(3)心力衰竭;(4)出现逐渐恶化的慢性心力衰竭;(5)需要再次行PCI或冠状动脉旁路移植术(CABG)治疗;(6)患者要求转诊。
1.3.2.2 社区医生管理 在患者PCI后1、3、6个月时,干预组每例患者与社区医生有1 h的个人咨询时间,社区医生主动进行指导,内容包括:心血管病危险因素控制情况、服药情况、生活方式、介入社会情况等。此外,干预组患者如有任何心血管相关问题可以与社区医生面对面或通过电话咨询。心血管病危险因素包括:体质指数(BMI)、收缩压(SBP)、舒张压(DBP)、三酰甘油(TG)、低密度脂蛋白胆固醇(LDL-C)、高密度脂蛋白胆固醇(HDL-C)、糖化血红蛋白(HbA1c)。生活方式包括:吸烟、体力活动、日常饮食、睡眠及心理状态。
1.4 随访 两组患者均在PCI后6、12个月时由项目专家组成员进行电话随访,随访内容包括:了解患者自觉症状,记录心血管病危险因素、服药情况,评估患者生活方式、主要不良心血管事件。本研究中最好的生活方式为:(1)不吸烟;(2)进行体力活动(规律运动>2次/周并>30 min/次,散步或运动>1 h/d);(3)日常饮食良好〔进食速度不快,睡前2 h不吃晚餐,吃快餐(预先做好的能够迅速供应的饭食)次数<3次/周,不吃早餐次数<3次/周,不每天饮酒,饮酒量<22 g/次〕;(4)睡眠好〔能在卧床后10~20 min入睡,入睡时间长期<10 min;睡眠中不醒或偶尔醒来(如小便)后能在5 min内入睡,直至第2天早晨;夜间睡眠无惊梦,做梦醒后很快忘记;睡眠中没有或很少出现噩梦、异常行为等;早晨睡醒后精力充沛,无疲劳感,工作效率高〕;(5)心理状态良好(无烦躁、抑郁)。主要不良心血管事件包括心肌梗死、靶目标血运重建(TLR)和全因死亡。
2 结果
2.1 基本资料及服药率比较 两组患者出院时基本资料及服药率比较,差异均无统计学意义(P>0.05,见表1)。
2.2 心血管病危险因素比较 PCI后6、12个月时,两组BMI、SBP、TG比较,差异均有统计学意义(P<0.05),其他指标比较,差异无统计学意义(P>0.05,见表2)。
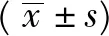
2.3 服药率比较 PCI后6个月时,两组钙离子拮抗剂(CCB)、硝酸盐类药物服药率比较,差异均有统计学意义(P<0.05);PCI后12个月时,两组CCB、β-受体阻滞剂、他汀类药物服药率比较,差异均有统计学意义(P<0.05,见表3)。
2.4 生活方式的影响因素分析 排除年龄和性别的混杂因素,以生活方式为因变量(赋值:规律运动>2次/周并>30 min/次=1,未达到规律运动>2次/周并>30 min/次=0;吃快餐次数>3次/周=1,未达到吃快餐次数>3次/周=0;饮酒<22 g/次=1,未达到饮酒<22 g/次=0;睡眠好=1,睡眠不好=0;烦躁=1,无烦躁=0;抑郁=1,无抑郁=0),以组别为自变量(赋值:干预组=0,对照组=1),进行Logistic回归分析,结果显示,组别是PCI后6个月睡眠、烦躁、抑郁的影响因素(P<0.05,见表4),组别是PCI后12个月规律运动>2次/周并>30 min/次、吃快餐次数>3次/周、饮酒<22 g/次、睡眠的影响因素(P<0.05,见表5)。
2.5 主要不良心血管事件发生率比较 PCI后6、12个月时,两组主要不良心血管事件发生率比较,差异均无统计学意义(P>0.05);其中PCI后6个月时,两组心肌梗死发生率比较,差异有统计学意义(P<0.05);PCI后12个月时,两组心肌梗死、TLR发生率比较,差异有统计学意义(P<0.05,见表6)。

表1 两组患者出院时基本资料及服药率比较Table 1 Comparison of basic information when out of hospital and medication rate between two groups

表2 两组患者PCI后6、12个月时心血管病危险因素比较Table 2 Comparison of cardiovascular risks between two groups at 6 months and 12 months after PCI
表3 两组患者PCI后6、12个月时服药率比较〔n(%)〕Table 3 Comparison of medication rate between two groups at 6 months and 12 months after PCI

表6 两组患者主要不良心血管事件发生率比较〔n(%)〕Table 6 Comparison of incidence rate of major adverse cardiovascular events between two groups

表4 组别对PCI后6个月生活方式影响的Logistic回归分析Table 4 Logistic regression analysis of the influence on life style at 6 months after PCI

表5 组别对PCI后12个月生活方式影响的Logistic回归分析Table 5 Logistic regression analysis of the influence on life style at 12 months after PCI
3 讨论
冠心病是中国人群的主要死因。PCI是我国目前治疗急性冠脉综合征的主要措施。我国2005年行PCI者达15万例,且以每年30%~40%的速度增加[10]。虽然先进的治疗技术已经提高了患者的生存率,但冠心病患者PCI后仍有较高的心血管事件发生风险。
3.1 社区管理对PCI后患者生活方式的影响 生活方式的调整包括对吸烟、饮酒、睡眠、饮食及体育锻炼的调整。规律的体育锻炼是生活方式管理的主要组成内容,其能增加运动耐力,降低危险因素,改善生活质量[11]。基于运动的心脏恢复较单纯的治疗可以促进心脏恢复,减少心血管病发生率和全因死亡率[12]。持续的体育锻炼能改善心血管病的危险因素,特别是降低总胆固醇、TG和SBP[13],本研究结果与之一致。
肥胖与心血管病病死率的增加、心脏功能恶化、心血管危险因素增加有关[14]。体质量增加根据BMI分为肥胖和超重。医生根据每次随访的体质量提供减重方案。通过体育锻炼和合理的饮食可以保持正常的体质量。戒烟可以减少心血管病患者全因死亡率[15-16]。心肌梗死或心脏术后戒烟可以减少1/3的病死率[15-16]。心肌梗死后患者抑郁的发病率是普通人群的3倍[17-18]。抑郁与心肌梗死后1、2年不良心血管事件的高发生率相关[19]。改善这些心血管病危险因素可以减少不良心血管事件发生率。
本研究定义的最好的生活方式行为是:不吸烟,规律运动>2次/周并>30 min/次,散步或运动>1 h/d,进食速度不快,睡前2 h不吃晚餐,吃快餐次数<3次/周,不吃早餐次数<3次/周,不每天饮酒,饮酒<22 g/d,睡眠好,无烦躁、抑郁。社区医生对PCI后患者进行生活方式的管理时应从以上方面进行管理。
3.2 社区管理对PCI后患者服药率的影响 阿司匹林被推荐用于所有冠心病二级预防患者,抗血小板治疗可以减少1/4的再发心血管事件[20-21]。β-受体阻滞剂能够减少心肌梗死的再发、猝死和心肌梗死后的病死率,所以也被推荐[22]。他汀类药物可以稳定斑块,血管紧张素Ⅱ受体拮抗剂(ARB)/血管紧张素转换酶抑制剂(ACEI)有益于心血管病的心脏恢复。本研究干预组管理后部分药物的服用率高于对照组。
3.3 社区管理对PCI后患者主要不良心血管事件的影响 社区医生在降低不良心血管事件及危险因素方面发挥关键作用[23]。本研究两组患者成功行PCI后出院时基本资料与服药率间无明显差异,但PCI后6、12个月时,干预组BMI、SBP和TG较对照组明显下降,PCI后12个月时,干预组心肌梗死发生率和TLR发生率均较对照组明显降低。说明经过社区医生的干预,能有效降低主要不良心血管事件的危险因素。
总之,有效的社区干预可以减少冠心病患者PCI后不良心血管事件的发生率,减少病死率,提高患者的生活质量[24]。开展针对社区医务人员的PCI后冠状动脉再狭窄防治知识的培训,能够有效提高防治冠状动脉狭窄的防治效果,有利于冠状动脉再狭窄的防治,并降低心血管病的发病率。
作者贡献:黄冠华进行研究设计与实施、资料收集整理、撰写论文、成文并对文章负责;王增帅、闫红进行研究实施、评估、资料收集;闫旭龙进行质量控制及审校。
本文无利益冲突。
本文不足之处:
(1)本研究对社区医生培训的覆盖面小,仅包括包头医学院第二附属医院周边的7个社区,所以入选对象为7个社区内的患者,限制了样本量;(2)随访时间较短,样本量小,无法绘制生存曲线。今后,继续扩大社区医生培训面,使更多居民分享当今冠心病防治的研究成果。
[1]高润霖.全国首次冠心病介入性治疗病例注册登记资料分析[J].中华心血管病杂志,1998,26(1):24-29. GAO R L.A data analysis of the First National Coronary Intervention Registry[J].Chin J Cardiol,1998,26(1):24-29.
[2]刘仁树,黄建群,史以钰.现代急症内科学[M].北京:人民卫生出版社,2005:559-563.
[3]何翠芳.康复护理干预对冠心病冠状动脉介入治疗患者生活质量的影响[J].辽宁医学院学报,2013,34(1):91-93. HE C F.Effect of rehebilitation on the quality of life for patients with CHD after PCI[J].Journal of Liaoning Medical University,2013,34(1):91-93.
[4]郑淑梅,杨秀兰,吕烨辉,等.延续性自我管理教育在冠心病介入治疗患者心脏康复中的应用[J]中华护理杂志,2012,47(4):297-300. ZHENG S M,YANG X L,LYU Y H.Effects of a continued self-management education program in the heart rehabilitation of patients after percutaneous coronary intervention therapy[J].Chinese Journal of Nursing,2012,47(4):297-300.
[5]LE GRANDEA M R,MURPHYA B M,HIGGINSA R O,et al.Psysical activity and negative emotional re- sponse after percutaneous coronary intervention[J].Eur J Cardiovasc Prev Rehabil,2006,13(2):254-260.
[6]FRIGOLA-CAPELL E,VAN LIESHOUT J,MUOZ M A,et al.Community programmes for coronary heart disease in Spanish primary care[J].Int J Health Plann Manage,2016,31(1):87-96.
[7]ZHU B,HARUYAMA Y,MUTO T,et al.Evaluation of a community intervention program in Japan using Framingham risk score and estimated 10-year coronary heart disease risk as outcome variables:a non-randomized controlled trial[J].BMC Public Health,2013,13:219.DOI:10.1186/1471-2458-13-219.
[8]PENNANT M,DAVENPORT C,BAYLISS S,et al.Community programs for the prevention of cardiovascular disease:a systematic review[J].Am J Epidemiol,2010,172(5):501-516.
[9]中华医学会心血管病学分会.2013年中华医学会冠心病康复与二级预防中国专家共识[J].中华心血管病杂志,2013,41(4):267-275.
[10]吕树铮,宋现涛,陈韵岱,等.中国大陆2005年度经皮冠状动脉介入治疗登记调查研究结果初步分析[J].中华心血管病杂志,2006,34(11):966-970. LYU S Z,SONG X T,CHEN Y D,et al.Beyond the numerals:primary reports from Registry of PCI in China (ROP IC) [J].Chin J Cardiol,2006,34(11):966-970.
[11]THOMPSON P D,BUCHNER D,PINA I L,et al.Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease:a statement from the Council on Clinical Cardiology (Subcommittee on Exercise,Rehabilitation,and Prevention) and the Council on Nutrition,Physical Activity,and Metabolism (Subcommittee on Physical Activity)[J].Circulation,2003,107(24):3109-3116.
[12]LEON A S,FRANKLIN B A,COSTA F,et al.Cardiac rehabilitation and secondary prevention of coronary heart disease:an American Heart Association scientific statement from the Council on Clinical Cardiology (Subcommittee on Exercise,Cardiac Rehabilitation,and Prevention) and the Council on Nutrition,Physical Activity,and Metabolism (Subcommittee on Physical Activity),in collaboration with the American Association of Cardiovascular and Pulmonary Rehabilitation [J].Circulation,2005,111(3):369-376.
[13]LARCOMBE J H.Exercise based cardiac rehabilitation reduces all cause and cardiac mortality in coronary heart disease[J].Evid Based Med,2004,9(6):175.
[14]KLEIN S,BURKE L E,BRAY G A,et al.Clinical implications of obesity with specific focus on cardiovascular disease:a statement for professionals from the American Heart Association Council on Nutrition,Physical Activity,and Metabolism:endorsed by the American College of Cardiology Foundation[J].Circulation,2004,110(18):2952-2967.
[15]CRITCHLEY J A,CAPEWELL S.WITHDRAWN:Smoking cessation for the secondary prevention of coronary heart disease[J].Cochrane Database Syst Rev,2012,15(2):CD003041.DOI:10.1002/14651858.CD003041.pub3.
[16]CRITCHLEY J A,CAPEWELL S.Mortality risk reduction associated with smoking cessation in patients with coronary heart disease:a systematic review[J].JAMA,2003,290(1):86-97.
[17]LICHTMAN J H,BIGGER JT J R,Blumenthal J A,et al.Depression and coronary heart disease:recommendations for screening,referral,and treatment:a science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing,Council on Clinical Cardiology,Council on Epidemiology and Prevention,and Interdisciplinary Council on Quality of Care and Outcomes Research:endorsed by the American Psychiatric Association[J].Circulationg,2008,118(17):1768-1775.
[18]王志军,王伟,周建芝,等.冠心病患者心理抑郁状态及其对预后的影响[J].中国全科医学,2015,18(26):3148-3152. WANG Z J,WANG W,ZHOU J Z,et al.Depressive state of patients with coronary artery disease and its influence on prognosis[J].Chinese General Practice,2015,18(26):3148-3152.
[19]TAYLOR C B,YOUNGBLOOD M E,CATELLIER D,et al.Effects of antidepressant medication on morbidity and mortality in depressed patients after myocardial infarction[J].Arch Gen Psychiatry,2005,62(7):792-798.
[20]Antithrombotic Trialists′Collaboration.Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death,myocardial infarction,and stroke in high risk patients[J].BMJ,2002,324(7329):71-86.
[21]王斌,高矩.经皮冠状动脉介入术后双联抗血小板治疗,缩短还是延长?[J].中国全科医学,2015,18(23):2751-2753,2757. WANG B,GAO J.Dual anti-platelet therapy after percutaneous coronary intervention:should it be shortened or prolonged?[J].Chinese General Practice,2015,18(23):2751-2753,2757.
[22]GHEORGHIADE M,GOLDSTEIN S.Beta-blockers in the post-myocardial infarction patient[J].Circulation,2002,106(4):394-398.
[23]JOLLY K,TAYLOR R S,LIP G Y,et al.Home-based cardiac rehabilitation compared with centre-based rehabilitation and usual care:a systematic review and meta-analysis[J].Int J Cardiol,2006,111(3):343-351.
[24]SMITH SC J R,ALLEN J,BLAIR S N,et al.AHA/ACC guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease:2006 update:endorsed by the National Heart,Lung,and Blood Institute[J].Circulation,2006,113(19):2363-2372.
(本文编辑:赵跃翠)
Effect of Community Management of Patients after PCI on Cardiovascular Events and Risk Factors
HUANGGuan-hua,YANXu-long,WANGZeng-shuai,YANHong.DepartmentofCardiology,theSecondAffiliatedHospitalofBaotouMedicalColledge,Baotou014030,China
Correspondingauthor:YANXu-long,DepartmentofCardiology,theSecondAffiliatedHospitalofBaotouMedicalColledge,Baotou014030,China;E-mail:xlyan811@aliyun.com
Objective To investigate the feasible management mode and effect of patients with coronary heart disease after percutaneous coronary intervention(PCI) and enhance the community physicans′ability for preventing the adverse events,and reduce the risk factors.Methods In 2014,87 patients who were accepted PCI at Department of Cardiology,the Second Affiliated Hospital of Baotou Medical College and met the inclusion criteria were enrolled.These patients were divided into two groups:the intervention group (47) could return to community and accept the management of community doctors,and the control group (40) could not return to community and accept the management.After accepting training from the Cardiovascular Disease Prevention and Treatment Research Center of the former Ministry of Health,the experts of the study trained the community physicians to manage the intervention group.The intervention group accepted the management of community doctors,and the control group did not accet any intervention.All patients accepted phone-call follow up at 6 months and 12 months after PCI.The cardiovascular disease risk factors,drug use,lifestyle,and the major adverse cardiovascular events of the two groups were recorded.Results The body mass index (BMI),systolic blood pressure (SBP) and triglyceride (TG) in the intervention group were significantly lower than those in the control group at 6 months and 12 months after PCI(P<0.05).There were statistically significant differences in the usage of calcium ion antagonist (CCB) and nitrate between the two groups at 6 months after PCI(P<0.05).There were statistically significant differences in the usage of CCB,β-blockers and statins between the two groups at 12 months after PCI(P<0.05).Logistic regression analysis showed that the group was the influencing factor for sleep qulity,irritability and depression at 6 months after PCI(P<0.05);and group was the influencing factor for regular exercise >2 times/week and >30 min/time,fasting food > 3 times/week,drinking <22 g/time,and sleep qulity at 12 months after PCI(P<0.05).There was statistically significant difference in the incidences in myocardial infarction between the two groups at 6 months after PCI(P<0.05).There were statistically significant differences in the incidence of myocardial infarction and TLR between the two groups at 12 months after PCI(P<0.05).Conclusion The community as a unit to file management is beneficial to the secondary prevention of coronary heart disease after PCI.Effective management of patients after PCI by community doctors can reduce adverse cardiovascular events and risk factors.
Angioplasty,balloon,coronary;Community health education;Major adverse cardiovascular events;Cardiovascular diseases;Risk factors
014030内蒙古包头市,包头医学院第二附属医院心内科
闫旭龙,014030内蒙古包头市,包头医学院第二附属医院心内科;E-mail:xlyan811@aliyun.com
R 54
A
10.3969/j.issn.1007-9572.2016.33.008
2016-05-20;
2016-09-22)
