高频电刀应用对心血管植入型电子器械囊袋血肿发生率的影响
2016-11-11徐白鸽梁延春高阳焉晓蕾于海波刘荣许国卿王娜王祖禄韩雅玲
徐白鸽 梁延春 高阳 焉晓蕾 于海波 刘荣 许国卿 王娜 王祖禄 韩雅玲
·临床研究·
高频电刀应用对心血管植入型电子器械囊袋血肿发生率的影响
徐白鸽梁延春高阳焉晓蕾于海波刘荣许国卿王娜王祖禄韩雅玲
目的探讨心血管植入型电子器械(CIED)植入术中应用高频电刀能否降低CIED囊袋血肿的发生率。方法回顾性分析在沈阳军区总医院接受新植入或更换CIED的患者3884例。CIED植入术中应用高频电刀的患者归为电刀组(3115例),而未应用高频电刀的患者归为对照组(769例)。两组患者各自又分为出血倾向亚组和无出血倾向亚组;出血倾向亚组再分为肝素桥接组和直接手术组。统计各组患者CIED囊袋血肿发生率。结果电刀组与对照组患者的基线资料均衡。CIED植入后1周共发生囊袋血肿86例(2.2%,86/3884),未发生CIED囊袋感染;而远期囊袋感染或破裂患者9例(10.5%,9/86)。电刀组囊袋血肿发生率显著低于对照组[1.5%(46/3115)比5.2%(40/769),P<0.001];电刀组中出血倾向亚组[1.8%(4/218)比11.5%(6/52),P=0.004]、无出血倾向亚组[1.4%(42/2897)比4.7%(34/717),P<0.001]和出血倾向亚组中的肝素桥接组[2.0%(2/100)比11.5%(6/52),P=0.020]CIED囊袋血肿发生率分别较对照组相应各亚组显著降低,差异均有统计学意义。对照组中出血倾向亚组CIED囊袋血肿发生率[11.5%(6/52)比4.7%(34/717),P=0.046]高于无出血倾向亚组,差异有统计学意义。而电刀组中出血倾向亚组与无出血倾向亚组的CIED囊袋血肿发生率比较,差异无统计学意义(P=0.560);电刀组出血倾向亚组中的肝素桥接组与直接手术亚组的CIED囊袋血肿发生率比较,差异亦无统计学意义(P=1.000)。结论 CIED植入术中应用高频电刀能降低囊袋血肿的发生率,并降低口服抗凝或抗血小板药物对囊袋血肿发生率的影响。
心血管植入型电子器械;高频电刀;囊袋;血肿
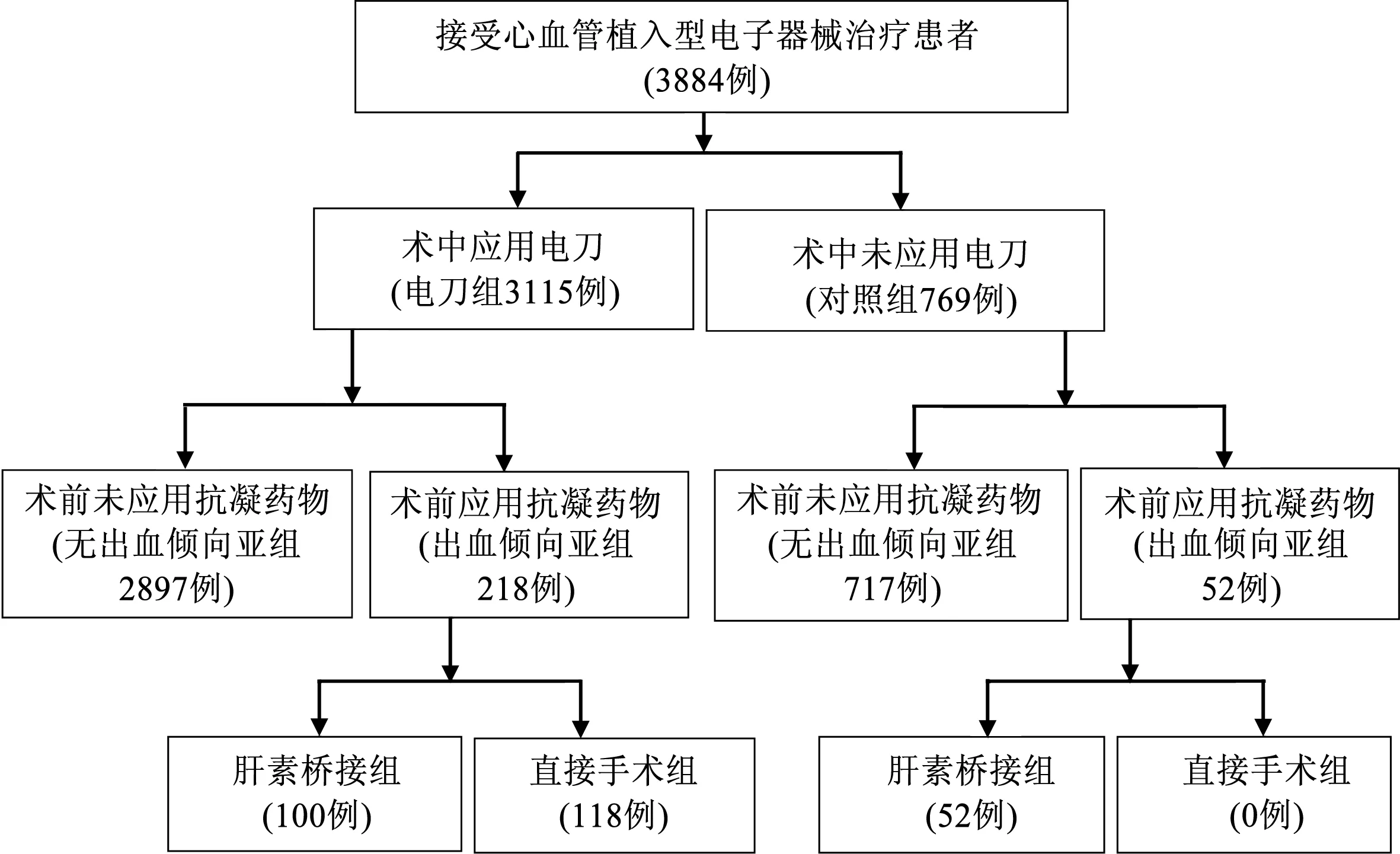
图1 本研究中植入心血管植入型电子器械人群分组示意图
心血管植入型电子器械(cardiac implantable electronic device, CIED)包括心脏起搏器、植入式心律转复除颤器(implantable cardioverter defibrillator,ICD)以及心脏再同步化治疗(cardiac resynchronization therapy,CRT)起搏器。CIED植入后囊袋血肿是植入永久起搏器术后最常见的早期并发症,是囊袋感染的重要危险因子[1-2]。高频电刀可同时进行切割和凝血,外科术中应用高频电刀使手术操作简单且止血效果好[3-4]。本研究探讨CIED植入术中应用高频电刀能否降低CIED囊袋血肿的发生率。
1 对象与方法
1.1研究对象
回顾性分析1998年1月至2016年3月于沈阳军区总医院接受新植入或更换CIED的患者(3884例)。本中心在2006年1月以后所有患者CIED的植入或更换手术均应用高频电刀。将应用高频电刀的患者归为电刀组(3115例),而未应用高频电刀的患者归为对照组(769例)。两组患者又根据是否应用抗凝药物又分为出血倾向亚组和无出血倾向亚组。出血倾向亚组再进一步细分为肝素桥接组和直接手术组(图1)。
1.2出血倾向亚组的入组标准及肝素桥接方案
出血倾向亚组患者的纳入标准:(1)患者入院时已连续服用华法林或新型抗凝药物超过4周;(2)已连续服用1或2种以上抗血小板药物超过4周。出血倾向亚组患者植入CIED围术期的肝素桥接方案:(1)应用抗血小板药物患者,于术前3 d停用,每12 h皮下注射低分子肝素1次桥接替代,至手术当日停用,术后12~24 h恢复原抗血小板药物方案治疗;(2)应用华法林或新型抗凝药物患者,于术前3 d停用,每12 h皮下注射低分子肝素1次桥接替代,当国际标准化比值(international normalized ratio,INR)<1.6时,进行CIED植入手术,并于手术当日停用低分子肝素,术后12 h恢复使用,如无出血倾向,术后3 d恢复服用华法林或新型抗凝药物,并与低分子肝素重叠应用到INR达标至2~3后停用低分子肝素。出血倾向亚组的直接手术亚组围术期不停用抗血小板药物或抗凝药物,仅调整药物剂量使INR在2~3即直接进行CIED植入或更换手术。
1.3CIED植入术中囊袋处理方法
局麻下,在左锁骨下静脉或腋静脉穿刺点下方2 cm处做一平行于锁骨的切口。对照组使用普通手术刀逐层切开皮下组织直至肌筋膜,对小动脉喷射状出血采用4号线结扎,对术区渗血及小出血点采用压迫止血。电刀组使用高频电刀(北京中科科仪技术发展有限责任公司YT70高频电刀,浙江舒友仪器设备有限公司生产的电刀笔,电刀电切输出能量50 W,电凝止血输出能量50 W)逐层电切割皮下组织至肌筋膜,对于术区渗血及小出血采用电凝止血,对于小动脉喷射状出血采用钳夹后电凝止血,必要时辅以4号线结扎。两组患者均于囊袋内放置纱布填塞止血20 min以上。对照组在CIED植入囊袋后如仍有渗血及小出血,予以排除积血后封闭囊袋继续加压包扎结束手术;电刀组在CIED植入囊袋后如仍有渗血及小出血,继续予以电凝止血,直至观察术区无渗血至少2 min后,关闭囊袋。两组患者CIED囊袋术区均常规加压包扎24~48 h。
1.4围术期CIED囊袋血肿定义
CIED植入术后1周内,患者自觉起搏器术区局部肿胀疼痛,CIED囊袋部位皮肤呈红色或青紫色肿胀,或可触及波动感。囊袋内压力明显增加时,如无菌穿刺抽出暗红色血液,细菌学检查排除囊袋感染即诊断为CIED囊袋血肿。
1.5统计学分析

2 结果
2.1电刀组与对照组患者的基线资料情况比较(表1)
两组患者的年龄、性别、糖尿病、肾功能不全、充血性心力衰竭、术前服用抗凝药物和(或)抗血小板药物、手术时间>3 h等比较,差异均无统计学意义(均P>0.05)。电刀组患者ICD(8.4%比1.7%,P<0.001)及CRT(8.0%比3.5%,P<0.001)植入率显著高于对照组,而单腔起搏器植入率(27.5%比42.5%,P<0.001)显著低于对照组,差异均有统计学意义。
2.2总体CIED囊袋血肿发生及转归情况
所有3884例患者中,CIED植入后1周内发生囊袋血肿86例(2.2%)。其中77例患者仅经加压包扎保守处理后血肿自行吸收;7例患者经严格无菌消毒穿刺抽吸出囊袋内积血后结合加压包扎处理血肿吸收;因血肿较大囊袋张力高,患者疼痛明显而经再次手术清除囊袋血肿并止血的患者2例,此2例患者均为对照组患者(1例为出血倾向亚组患者,另1例为无出血倾向亚组患者)。所有囊袋血肿患者术后1周内均未发生CIED囊袋感染,但远期(术后6个月以上)合并CIED囊袋感染或囊袋破裂者9例(10.5%),其中4例患者行CIED、起搏导线移除及择期对侧植入术,5例患者行囊袋清创修补术。
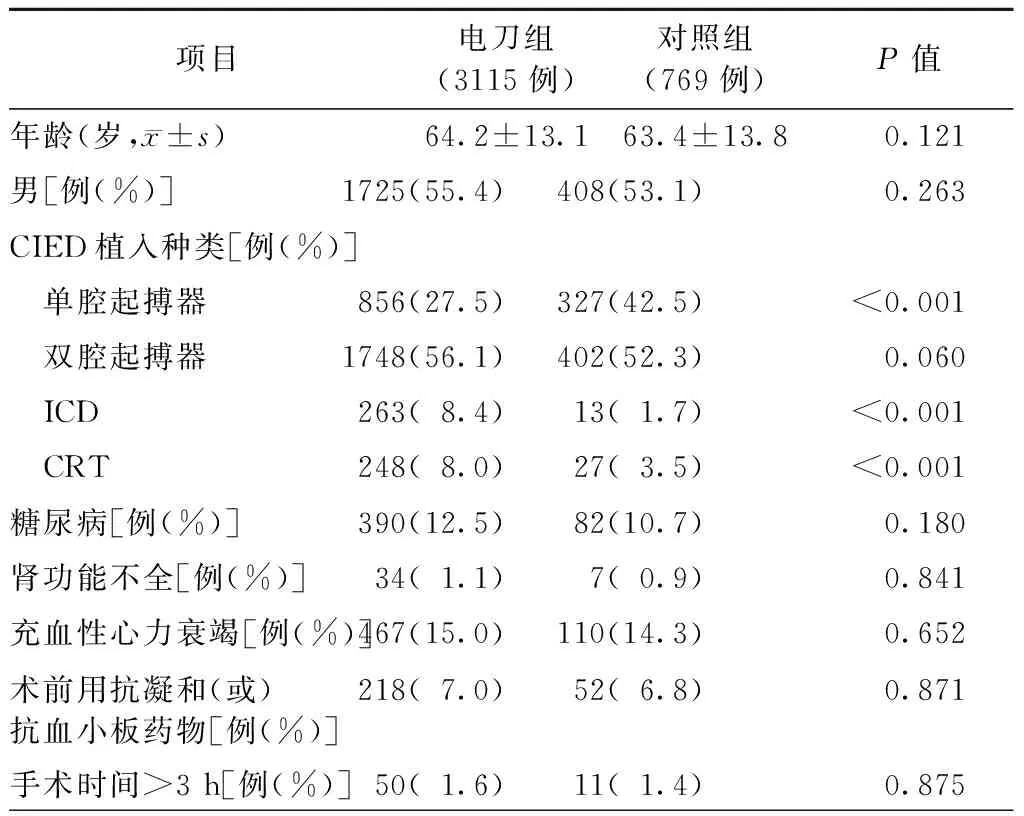
表1 电刀组与对照组患者的基线资料比较
注:ICD,植入式心律转复除颤器;CRT,心脏再同步治疗(包括有除颤功能的CRT);CIED,心血管植入型电子器械
2.3电刀组与对照组中各亚组组间及组内CIED囊袋血肿发生率比较
CIED植入术中电刀组囊袋血肿发生率显著低于对照组(1.5%比5.2%,P<0.001),差异有统计学意义;电刀组中出血倾向亚组(1.8%比11.5%,P=0.004)、无出血倾向亚组(1.4%比4.7%,P<0.001)和出血倾向亚组中的肝素桥接组(2.0%比11.5%,P=0.020)CIED囊袋血肿发生率分别较对照组相应各亚组显著下降,差异有统计学意义。对照组中出血倾向亚组CIED囊袋血肿发生率高于无出血倾向亚组(11.5%比4.7%,P=0.046),差异有统计学意义。而电刀组中出血倾向亚组与无出血倾向亚组的CIED囊袋血肿发生率比较,差异无统计学意义(P>0.05);电刀组出血倾向亚组中的肝素桥接组与直接手术组的CIED囊袋血肿发生率比较,差异亦无统计学意义(P>0.05,图2)。
3 讨论
CIED囊袋血肿是CIED植入术后最常见的早期并发症之一,文献报道其发生率为2.3%~5.1%[1]。
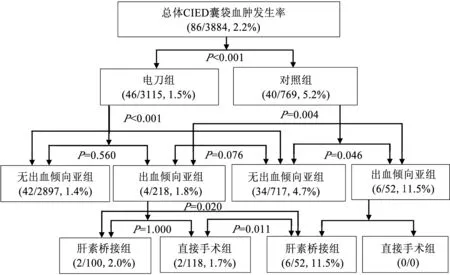
CIED,心血管植入型电子器械 图2 电刀组与对照组及各亚组组间和组内心血管植入型电子器械囊袋血肿发生率比较结果
囊袋血肿的形成与以下因素有关:(1)术中操作粗糙、止血不彻底、创伤大;(2)患者自身的凝血功能障碍或口服抗凝、抗血小板药物[2];(3)囊袋过大过深、位置不合适、胸壁皮肤松弛等。有文献报道围术期应用抗血小板药物或抗凝药物治疗患者发生囊袋出血风险增高[2]。目前,越来越多的患者接受抗凝和(或)抗血小板药物治疗,但如果为减少CIED囊袋血肿发生率而停用这些药物可能会导致卒中、瓣膜血栓、支架内血栓等更严重的并发症发生[5]。对于这类患者,曾经一度应用围术期肝素替代治疗,但实践证实该替代疗法不能降低CIED囊袋血肿发生率[6]。因此,有出血倾向的患者植入CIED如何减少囊袋血肿发生率对临床医生是个挑战。
压迫止血是CIED植入术囊袋止血的传统方法,主要依靠压迫及自身凝血机制达到止血目的。但该传统术式的缺点是止血不彻底。此法对于凝血功能正常的患者比较有效,而对于服用抗凝和(或)抗血小板药物等有出血倾向的患者,容易囊袋血肿,甚至造成晚期囊袋感染等严重并发症发生[2]。高频电刀利用高密度的高频电流使组织或组织成分气化或爆裂,从而达到凝固或切割的目的,其止血过程与血小板及凝血因子无关。优点在于止血安全有效,显著减少了出血甚至可能不出血,有效降低术后囊袋血肿发生率,尤其适合有出血倾向的高危患者[3-4]。
本研究通过对CIED植入术中应用高频电刀和常规压迫止血法两组较大样本人群进行比较,认为使用高频电刀能显著降低CIED围术期囊袋血肿总发生率,该效果同样体现在有出血倾向的人群中。对有出血倾向患者如果使用高频电刀术中彻底止血,其CIED围术期囊袋血肿发生率与无出血倾向患者比较差异无统计学意义,而与对照组出血倾向患者相比,血肿发生率显著降低;即使与对照组无出血倾向患者相比,其血肿发生率亦有降低趋势,但差异无统计学意义,这可能与例数较少有关。CIED囊袋血肿是囊袋感染的重要危险因素[2],本研究中囊袋血肿患者中合并CIED囊袋感染或囊袋破裂者高达10.5%。提示围术期预防CIED囊袋血肿具有十分重要的意义,而高频电刀的应用对预防CIED囊袋血肿具有明确的价值。
[1] Gribbin GM,Mccomb JM,Bexton RS. Ventricular pacemaker upgrade:experience,complications and recommendations.Heart,1998,80(4):420.
[2] Wiegand UK, LeJeune D, Boguschewski F, et al. Pocket hematoma after pacemaker or implantable cardioverter defibrillator surgery: influence of patient morbidity, operation strategy, and perioperative antiplatelet/anticoagulation therapy. Chest,2004, 126(4): 1177-1186.
[3] 蒋靖波,伍于斌,张伟,等.永久起搏器植入术中应用电灼术的临床观察.医学综述,2009,15(17):2707-2709.
[4] 赵迎新,周玉杰,聂斌,等.电灼术在永久起搏器植入术中的应用.首都医科大学学报,2006,27(5):660-662.
[5] Alkhadra AS.Implantation of pacemakers and implantable cardioverter defibrillators in orally anticoagulated patients.Pacing Clin Electrophysiol,2003,26(1 Pt 2):511-514.
[6] Milic DJ,Perisic ZD,Zivic SS,et al.Prevention of pocket related complications with fibrin sealant inpatients undergoing pacemaker implantation who are receiving anticoagulant treatment.Can J Psychology,2005,20(2):374-379.
Influence of high frequency electrosurgical equipment application in cardiac implantable electronic device implantation procedure on the rate of pocket hematoma
XUBai-ge,LIANGYan-chun,GAOYang,YANXiao-lei,YUHai-bo,LIURong,XUGuo-qing,WANGNa,WANGZu-lu,HANYa-ling.
DepartmentofCardiology,GeneralHospitalofShenyangMilitaryRegion,Shenyang110016,China
LIANGYan-chun,Email:liangyanchun@sina.com
ObjectiveTo investigate the influence of high frequency electrosurgical equipment (HFEE) application in cardiac implantable electronic device (CIED) implantation procedure on the rate of pocket hematoma. MethodsPatients who received CIED implantation in General Hospital of Shenyang Military Region were analyzed retrospectively. HFEE was applied during CIED implantation procedure in every patient who was classified into HFEE group. Other patients without HFEE application were classified as the control group. Patients with or without bleeding tendency were sub-classified into the bleeding tendency subgroup or non-bleeding tendency subgroup respectively. Bleeding tendency subgroup was further divided into heparin bridging group and direct implantation group. The occurance rate of CIED pocket hematoma was recorded in all groups. ResultsA total of 3884 patients were enrolled. There were 3115 patients in the HFEE group and 769 patients in the control group. The baseline data of two groups was similar. The overall rate of CIED pocket hematoma in the total patient population during perioperative period were 2.2% (86/3884), and the rate of long term pocket infection or rupture in patients with CIED pocket hematoma was 10.5% (9/8). In the HFEE group, the rate of pocket hematoma was lower than that in the control group (1.5%vs. 5.2%,P<0.001). The rates of CIED pocket hematoma in respective subgroups in the HFEE group including the bleeding tendency subgroup (1.8%vs. 11.5%,P=0.004), the non-bleeding tendency subgroup (1.4%vs. 4.7%,P<0.001) and the heparin bridging group (2.0%vs. 11.5%,P=0.046) were markedly decreased as compared with the corresponding subgroups in the control group. In the control group, the rate of CIED pocket hematoma in the bleeding tendency subgroup was higher than that in the non-bleeding tendency subgroup (11.5%vs. 4.7%,P=0.0046). In HFEE group, there was no significant difference in the rate of CIED pocket hematoma between bleeding tendency subgroup and non-bleeding tendency subgroup; and there was also no significant difference in the rate of CIED pocket hematoma between the heparin bridging group and the direct implantation group. Conclusion Application of HFEE in CIED implantation procedure could reduce the incidence of pocket hematoma, and there was no significant difference in the incidence of pocket hematoma in patients with or without oral anticoagulation or antiplatelet agents.
Cardiac implantable electronic device;High frequency electrosurgical equipment;Pocket;Hematoma
10.3969/j.issn.1004-8812.2016.09.005
辽宁省自然科学基金项目(2015020406)
110016辽宁沈阳,沈阳军区总医院心血管内科
梁延春,Email:liangyanchun@sina.com
R541.7
2016-05-19)
