EORTC危险评分系统对T1期非肌层浸润性膀胱癌患者的预后评价
2016-09-06林瑞杜君张艳辉陈倩倩李宏蕾姚欣
林瑞 杜君 张艳辉 陈倩倩 李宏蕾 姚欣
EORTC危险评分系统对T1期非肌层浸润性膀胱癌患者的预后评价
林瑞杜君张艳辉陈倩倩李宏蕾姚欣
目的:评价欧洲癌症研究与治疗组织(EORTC)膀胱癌预后风险评分表对T1期非肌层浸润性膀胱癌(non-muscle-invasive bladder cancer,NMIBC)患者预后判断的准确性。分析T1期NMIBC复发进展相关因素,探讨更适用于T1期NMIBC的危险分层方法。方法:回顾性分析2011年1月至2013年6月天津医科大学肿瘤医院108例行经尿道膀胱肿物电切术的T1期NMIBC患者的临床病理资料。根据患者不良预后指标进行评分,应用ROC曲线获取临界值重新进行危险分层,建立新的危险评分模型。结果:108例患者中男性90例(83%)、女性18例(17%),中位年龄65(24~88)岁,21例(19.4%)复发,11例(10.2%)进展。结论:EORTC评分系统对T1期NMIBC患者复发进展预测效能不准确。肿瘤大小及既往复发概率为肿瘤复发的独立性预后因素,肿瘤分级及既往复发概率为肿瘤进展的独立性预后因素。应用新的危险评分模型能够更准确的预测T1期NMIBC患者的复发进展风险。
T1期非肌层浸润性膀胱癌复发进展独立预后因素
膀胱癌为一类生物学特性多样且复发进展率较高的肿瘤[1],是泌尿系统最常见的恶性肿瘤之一。在美国,男、女性膀胱癌发病率分别占恶性肿瘤第4、第9位,且其新发病例数呈逐年增长趋势[2]。在我国,男性膀胱癌发病率位居恶性肿瘤第7位、女性居第10位以上[3]。近年来,我国部分城市膀胱癌的发病率有增高趋势。
T1期膀胱癌具有较大异质性,部分患者病情恶化较快,肿瘤的复发进展为影响其预后的主要问题,进展为肌层浸润性膀胱癌的预后极差[4]。如何早期识别该部分患者,是临床亟待解决的难题。因此,发现T1期非肌层浸润性膀胱癌(non-muscle-invasive bladder cancer,NMIBC)复发进展的风险预测有效指标可对T1期膀胱癌患者的预后产生重要意义。
1 材料与方法
1.1材料
回顾性分析2011年1月至2013年6月天津医科大学肿瘤医院108例行经尿道膀胱肿物电切术的T1 期NMIBC患者的临床病理资料及术后随访资料,108例患者中男性90例(83%)、女性18例(17%)。年龄为24~88岁,中位年龄65岁。所有病理切片由同一位病理科专家复习,排除Ta及T2期以上患者。
1.2方法
复发进展时间为患者手术时间至肿瘤第1次复发或进展为肌层浸润性膀胱癌的时间,分析患者临床病理资料,评价欧洲癌症研究与治疗组织(EORTC)膀胱癌预后风险评分表的预后效能。根据患者不良预后指标进行评分,应用ROC曲线获取临界值重新进行危险分层,建立新的危险评分模型。
1.3统计学分析
采用SPSS 22.0软件进行数据统计学处理。单因素分析采用Kaplan-Meier法,组间比较采用Log rank检验,多因素分析采用Cox风险回归模型。以P<0.05为差异具有统计学意义。
2 结果
108例患者的中位年龄为65岁,83%(90/108)为男性,74%(80/108)肿瘤大小<3 cm,62%(67/108)为单发,75%(81/108)为初发,15%(16/108)伴有原位癌(carcinoma in situ,CIS)。108例患者中肿瘤复发为21例(19%),复发时间为4.2~47.9个月;进展为肌层浸润性膀胱癌为11例(10%),进展时间为8.5~25.3个月。根据EORTC评分系统对108例患者进行评分,其中复发中危组为98例(91%)、高危组为10例(9%),进展中危组为23例(21%)、高危组为85例(79%)。Kaplan-Meier法单因素分析结果显示,肿瘤大小与分级分别为肿瘤复发与进展的影响因素,而肿瘤数目与既往复发概率同为肿瘤复发进展的不良预后指标(P<0.05,表1)。EORTC评分系统对本研究T1期NMIBC患者复发预测效能较好(图1A),对于进展预测较差(图1B)。Cox风险回归模型多因素分析结果显示,肿瘤大小及既往复发概率为肿瘤复发风险的独立性预后因素,而肿瘤分级及既往复发概率为肿瘤进展的独立性预后因素(P<0.05,表2)。
本研究采用现有数据对T1期NMIBC患者重新进行危险评分。根据不良预后的指标对患者进行评分,肿瘤大小为1~2分,既往复发概率为0~2分,肿瘤分级为1~3分。应用ROC曲线获得复发进展评分的临界值,复发风险评分临界值为2分、进展风险评分临界值为3分,应用Kaplan-Meier生存分析进行评估,发现新的危险分层更适合预测T1期NMIBC的预后(图2)。
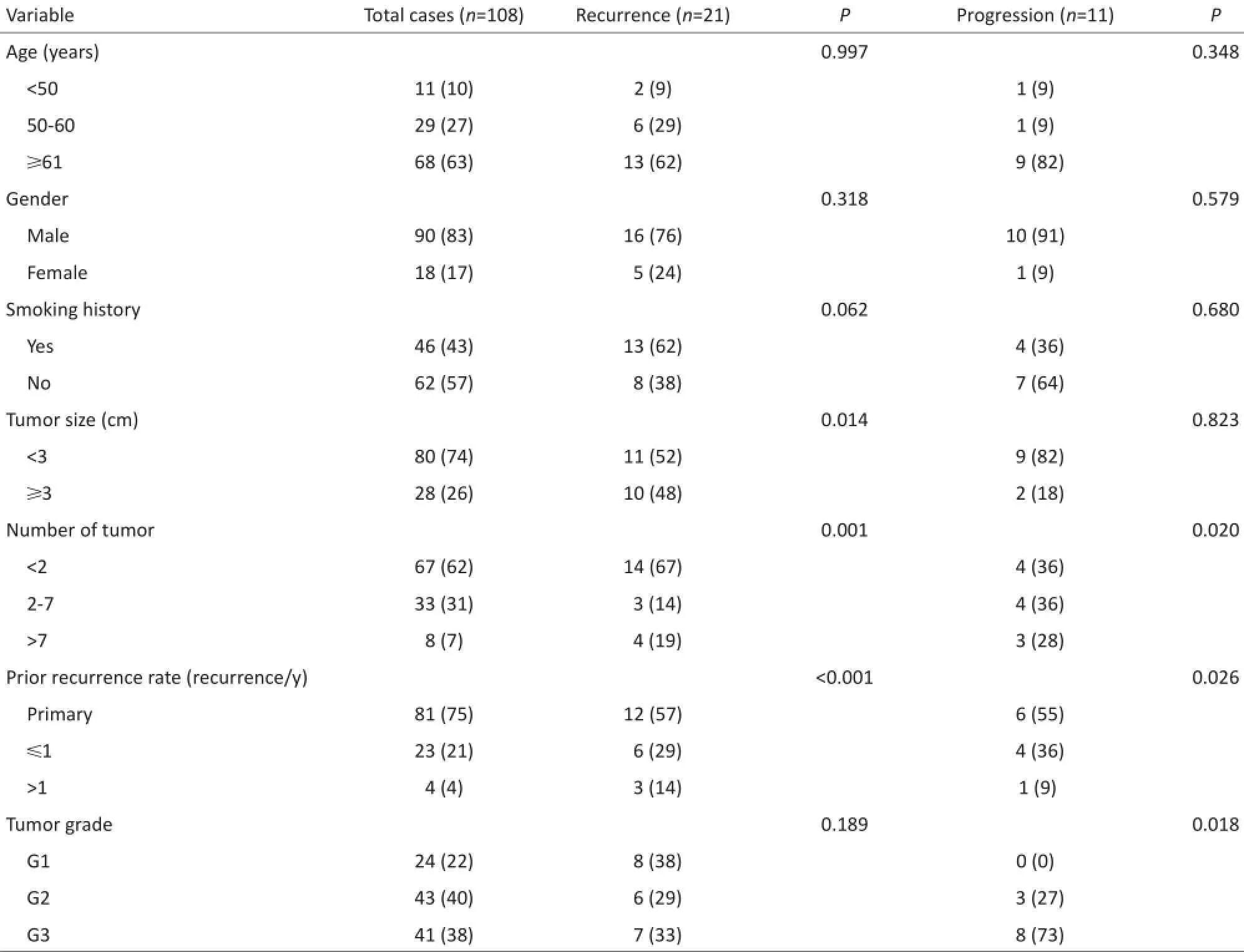
表1 108例患者基本临床病理特征及影响患者预后的单因素分析Table 1 Clinicopathologic data and univariate analysis of the prognosis of 108 patients

表1 108例患者基本临床病理特征及影响患者预后的单因素分析(续表1)Table 1 Clinicopathologic data and univariate analysis of the prognosis of 108 patients

图1EORTC评分系统对T1期NMIBC患者预后的预测效能Figure 1 Prognosis prediction of T1 NMIBC patients using EORTC

表2 影响患者预后的多因素分析Table 2 Multivariate analysis of patient prognosis

图2 新的危险评分模型对T1期NMIBC患者预后的预测效能Figure 2 Prognosis predictions for T1 NMIBC patients using the new risk scoring model
3 讨论
膀胱癌最常见的病理类型为尿路上皮癌,根据2002年国际抗癌协会TNM分期(第六版)[5],膀胱癌分为非肌层浸润性膀胱癌(non-muscle invasive bladder cancer,NMIBC)和肌层浸润性膀胱癌(muscle invasive bladder cancer,MIBC)。约75%膀胱癌患者初诊时为NMIBC,在NMIBC患者中70%为非浸润性尿路上皮癌(Ta期)、20%浸润黏膜层(T1期)、10%为CIS。T1期NMIBC确诊率较高,但约50%患者两年内复发,且近25%患者进展为肌层浸润性膀胱癌[6]。当T1期NMIBC患者进展为肌层浸润性膀胱癌,即使行膀胱全切术,预后也是不理想[7]。因此T1期膀胱癌患者治疗方案的选择存在风险,一方面保守治疗有可能导致肿瘤进展甚至死亡;另一方面若选择膀胱全切术,对于未进展的患者则为过度治疗。如果能有一些预测指标可更早的指导分辨易于进展的患者,以采取更为密切的检测或者积极的治疗,对于提高患者预后有较大的意义。
NMIBC的预后与临床病理特征之间的关系已进行较多的研究[6,8-10]。目前临床最常用的为EORTC风险表[8],此表是通过多因素分析而得出6个临床病理指标来预测肿瘤复发进展率。但这种预测工具在临床工作中的应用并不广泛,其中一个原因就是其在临床应用中并不能精确的指导治疗方案的制定[11],且此表是针对所有NMIBC患者进行评估,而非进展风险较大、预后较差的T1期膀胱癌患者。
本研究分析108例T1期NMIBC患者的临床病理特征,发现EORTC评分系统对于T1期非肌层浸润性膀胱癌的复发风险预测性较好,而对进展风险的预测性则较差,并进行单因素及多因素分析发现肿瘤大小及既往复发概率为肿瘤复发风险的独立性预后因素,而肿瘤分级及既往复发概率为肿瘤进展的独立性预后因素。根据研究结果对患者重新进行危险评分,结果显示新的危险评分模型能够更准确的预测T1期NMIBC患者的复发进展风险。本研究的新的危险评分模型更加简单易行,对于T1期NMIBC的预测效能更加准确,更适用于临床预后分析。但本研究属于回顾性分析,样本量较少,尚需更大样本量的临床资料的验证。此外,近年关于T1期NMIBC预后指标的研究越来越多,临床病理资料结合生物标志物等将以期发现更加精准的T1期非肌层浸润性膀胱癌预后体系,也将为以后的研究指明方向。
[1] Burger M,Catto JW,Dalbagni G,et al.Epidemiology and risk factors of urothelial bladder cancer[J].Eur Urol,2013,63(2):234-241.
[2]Aldousari S,Kassouf W.Update on the management of non-muscle invasive bladder cancer[J].Can Urol Assoc J,2010,4(1):56-64.
[3]Stein AN,Britt H,Harrison C,et al.Herpes zoster burden of illness and health care resource utilization in the Australian population aged 50 years and older[J].Vaccine,2009,27(4):520-529.
[4]van den Bosch S,Alfred Witjes J.Long-term cancer-specific survival in patients with high-risk,non-muscle-invasive bladder cancer and tumour progression:a systematic review[J].Eur Urol,2011,60(3):493-500.
[5] Piemonte M.TNM-classification of malignant tumors(VI edition-2002).Innovations in the classification of head and neck neoplasms [J].Acta Otorhinolaryngol Ital,2003,23(2):132-135.
[6]Babjuk M,Burger M,Zigeuner R,et al.EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder:update 2013[J]. Eur Urol,2013,64(4):639-653.
[7] Brausi M,Witjes JA,Lamm D,et al.A review of current guidelines and best practice recommendations for the management of nonmuscle invasive bladder cancer by the International Bladder Cancer Group[J].J Urol,2011,186(6):2158-2167.
[8]Sylvester RJ,van der Meijden AP,Oosterlinck W,et al.Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables:a combined analysis of 2596 patients from seven EORTC trials[J].Eur Urol,2006,49(3):466-477.
[9]Vedder MM,Márquez M,de Bekker-Grob EW,et al.Risk prediction scores for recurrence and progression of non-muscle invasive bladder cancer:an international validation in primary tumours[J].PLoS One,2014,9(6):e96849.
[10]Cambier S,Sylvester RJ,Collette L,et al.EORTC nomograms and risk group for predicting recurrence,progression,and disease-specific and overall survival in non-muscle-invasive stage Ta-T1 urothelial bladder cancer patients treated with 1-3 years of maintenance bacillus Calmette-Guérin[J].Eur Urol,2016,69(1):60-69.
[11]Kluth LA,Black PC,Bochner BH,et al.Prognostic and prediction tools in bladder cancer:a comprehensive review of the literature [J].Eur Urol,2015,68(2):238-253.
(2016-05-18收稿)(2016-07-14修回)
The use of European Organization of Research and Treatment of Cancer Risk Tables to predict the prognosis of patients with T1 non-muscle-invasive bladder cancer
Rui LIN,Jun DU,Yanhui ZHANG,Qinanqian CHEN,Honglei LI,and Xin YAO
Correspondence to:Xin YAO;E-mail:yaoxin1969@hotmail.com
Department of Genitourinary Oncology,Tianjin Medical University Cancer Institute and Hospital,National Clinical Research Center for Cancer,Tianjin Key Laboratory of Cancer Prevention and Therapy,Tianjin 300060,China
Objective:To assess the accuracy of the European Organization of Research and Treatment of Cancer(EORTC)Risk Tables in predicting the prognosis of patients with T1 non-muscle-invasive bladder cancer(NMIBC)treated in the Tianjin Medical University Cancer Institute and Hospital(TMUCIH).The prognostic factors of T1 NMIBC are also explored,and a new risk scoring model suitable for T1 NMIBC is determined.Methods:We retrospectively reviewed the clinicopathologic characteristics of 108 patients with T1 NMIBC who underwent transurethral resections in TMUCIH from January 2011 to June 2013.We scored patients based on the number of adverse factors.Afterwards,divided them into different risk groups by the limits determined using receiver operating characteristic curve (ROC)analysis,and created a new risk scoring model.Results:In a group of 108 patients,90(83%)were male and 18 were female (17%).The median age was 65 years old(ranging from 24 to 88).Furthermore,21 patients(19.4%)had a recurrence and 11 cases (10.2%)progressed to muscle-invasive disease.Conclusion:The EORTC cannot accurately predict the recurrence and progressive rate of T1 NMIBC.The most important prognostic factors for recurrence were tumor size and prior recurrence rate.Tumor grade and prior recurrence rate are independent prognostic factors for tumor progression.The new risk scoring model is more accurate in predicting the recurrence risk and progression of T1 NMIBC.
T1,non-muscle-invasive bladder cancer,recurrence,progression,independent prognostic factors

10.3969/j.issn.1000-8179.2016.15.578
天津医科大学肿瘤医院泌尿肿瘤科,国家肿瘤临床医学研究中心,天津市肿瘤防治重点实验室,天津市恶性肿瘤临床医学研究中心(天津市300060)
姚欣yaoxin1969@hotmail.com
林瑞专业方向为泌尿肿瘤临床及基础治疗。E-mail:linrui9114@126.com
