Unusual case of nephrocutaneous fistula-Our experience
2016-04-27RajeevThekumpadamPuthenveetilDebajitBaishyaSasankaBaruaDebangaSarma
Rajeev Thekumpadam Puthenveetil*,Debajit Baishya, Sasanka Barua,Debanga Sarma
Department of Urology,Gauhati Medical College Hospital,Guwahati,Assam,India
Unusual case of nephrocutaneous fistula-Our experience
Rajeev Thekumpadam Puthenveetil*,Debajit Baishya, Sasanka Barua,Debanga Sarma
Department of Urology,Gauhati Medical College Hospital,Guwahati,Assam,India
Renal calculus;
A rare case of nephrococutaneous fistula due to spontaneous expulsion of renal calculi is described.A 45-year-old man presented with urinary leakage from an ulcer over the left lumbar region for the last 3 months after a history of spontaneous expulsion of stones from this area.Ultrasonography abdomen revealed a small contracted kidney with multiple calculi in the kidney and renal pelvis,sinus tract from the lower pole of the left kidney with a ruptured calyceal calculus in the sinus tract.CT urography revealed a non excreting left kidney with multiple renal calculi,with hyperdense collection in the renal parenchyma extending to the subcutaneous tissue and left lung suggesting a xenthogranulomatous pyelonephritis (XGP).We performed a left-sided simple nephrectomy with excision of the fistulous tract.Histopathological examination revealed XGP.There have been a few case reports of XGP forming nephrocutaneous fistula in the back.
ⓒ2016 Editorial Office of Asian Journal of Urology.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
1.Introduction
Xanthogranulomatous pyelonephritis(XGP)is an atypical, chronic inflammatory disease of the kidney.Although the pathogenesis of XGP is still unclear,the primary factors are urolithiasis,urinary tract obstruction and infection[1]. Proteus species and Escherichia coli are the organisms most commonly isolated in XGP[2].Although the inflammatory process is usually diffuse and can extend beyond the kidney,nephrocutaneous fistula formation is a very rare presenting sign[3].Gastrointestinal system,adjacent urinary organs and skin are the most commonly involved structures. Nephrectomy and primary excision of fistula is usually curative.
2.Case history
A 45-year-old male came with a history of intermittent discharge from an ulcer over the left-side of back since thelast 3 months.This was preceded with on and off pain in the left flank,fever with chill and rigor for 6 months which progressed to thinning and reddening of skin over left-side of the back and sudden bursting out with expulsion of 2-3 small calculi,following which he got relieved of his symptoms leaving behind an ulcer over that region through which clear urine leaked intermittently.
Per abdominal examination revealed two ulcers of size 1 cm×1 cm and 1.5 cm×2 cm on the left-side of the back, just lateral to posterior axillary line,below the 12th rib.It was pale red in color and did not bleed to touch(Fig.1). The margins were inverted and occasional discharge of clear urine could be seen.
Laboratory investigation revealed a normal leukocyte count(8.89×109/L),haemoglobin of 83 g/L.Urinalysis showed the presence of more than 10 leukocytes per highpower microscopic field,but no bacterial growth was observed.Culture from the fistulous discharge showed no growth.
Ultrasonography abdomen(USG-KUB)revealed a small contracted kidney with multiple calculiin the leftkidney and renal pelvis,sinus tract from the lower pole with a ruptured calyceal calculus in the sinus tract(Fig.2).CT-IVU was done which revealed a non excreting left kidney with multiple renal calculi,with hyperdense collection in the renal parenchyma extending to the subcutaneous tissue and the left lung suggesting XGP(Fig.3).Preoperative ulcer biopsy showed increased granulation and collagenous tissue.
Nephrectomy was done by thoracolumbar incision (Fig.4).Intraoperatively,it was noticed that the renal fistula extended to the lung parenchyma and skin.Fistulectomy was successfully performed with excision of the surrounding granulation tissue involving the renal and lung parenchyma.A 24 Fr chest tube was placed and removed subsequently after full expansion of the left lung on the 5th postoperative day.Histopathological examination revealed chronic granulomatous inflammation of the left kidney with diffuse infiltration of lipid-laden histiocytes,consistent with the diagnosis of XGP.
3.Discussion
XGP is a rare chronic inflammation of the kidney and constitutes less than 1%of chronic pyelonephritis.It was first described by Schlagenhaufer in 1916[4].It is characterized by destruction of renal parenchyma and its replacement with granulomatous tissue,abscesses and collection of lipid laden macrophages(xanthoma cells)[5,6].Females are more affected than males with a ratio of 1:4,and with a mean age varying from 45 to 55 years[6,7].Though the exact mechanism of XGP is not clear,a number of predisposing factors have been implicated.The two most common predisposing factors are obstruction and infection of the genitourinary system.Calculi are frequently staghorn type(47%-100%).The organisms most commonly isolated in XGP are Proteus species and E.coli[1,2].Although many XGP patients have shown pyuria,bacterial growth in their urine has only been demonstrated in two-thirds probably because urinary obstruction blocks contaminated urine to reach the bladder.Rather,the unidentified organism could be revealed by renal tissue cultures taken during surgery.
There are two forms of XGP.The diffuse or global form (85%)is more common than the localized,focal or segmental form(15%).Based on the severity of the disease XGP has been described in three stages[8].In stage I the lesion is confined to kidney,in stage II the lesion extends toGerota’s fascia and in stage III extends to the paranephric space and other retroperitoneal structures.

Figure 1Fistulous tract.
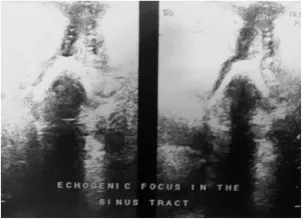
Figure 2Ultrasonography abdomen showing sinus tract with a ruptured calyceal calculus in the sinus tract.

Figure 3CT urography showing non excreting left kidney with multiple renal calculi,with hyperdense collection of the renal parenchyma extending to subcutaneous tissue.
Fistula formation is an unusual presenting sign in XGP. Gastrointestinal system,adjacent urinary organs and skin are the most commonly involved structures.There is a tendency of perirenal inflammation to spread superiorly along the lines of fusion of renal fascial planes that tend to direct the exudates within the retroperitoneal compartment.The lumbocostal triangle,a relatively weak area of diaphragm,can transmit infection into the thoracic cavity which may cause nephrobronchial fistulas and lung abscess [9].Cutaneous fistula occurs mostly into ipsilateral flank region,but unusual localizations such as knee were previously reported[10].XGP presented with spontaneous expulsion of renal calculi is extremely rare.
XGP itself is an infiltrating disease and together with an obstructing stone in the renal pelvis may cause pyonephrosis and perinephric abscess.Later,it may burst out through the overlying skin.
Radiological diagnosis of XGP can be challenging as it is often difficult to differentiate it from primary renal neoplasms,pyonephrosis and other retroperitoneal mesenchymal tumors.USG-KUB is usually the first investigation during evaluation of such cases.CT is the imaging modality of choice as it not only suggests the diagnosis but also shows the extrarenal extent of the disease.
Nephrectomy and primary excision of fistula is curative in diffuse renal destruction[10].
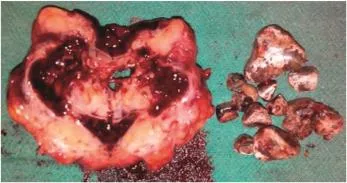
Figure 4Post operative nephrectomy specimen with multiple calculi.
Conflicts of interest
The authors declare no conflict of interest.
[1]Gregg CR,Rogers TE,Munford RS.Xanthogranulomatous pyelonephritis.Curr Clin Top Infect Dis 1999;19:287-304.
[2]Korkes F,Favoretto RL,Bro´glio M,Silva CA,Castro MG, Perez MD.Xanthogranulomatous pyelonephritis:clinical experience with 41 cases.Urology 2008;71:178-80.
[3]Loffroy R,Guiu B,Watfa J,Michel F,Cercueil JP,Krause´D. Xanthogranulomatous pyelonephritis in adults:clinical and radiological findings in diffuse and focal forms.Clin Radiol 2007;62:884-90.
[4]Khalid S,Zaheer S,Zaheer S,Ahmad I,Khalid Mohd.Xanthogranulomatous pyelonephritis:rare presentation of a rare disease.South Asian J Cancer 2013;2:4.
[5]Yoshino T,Moriyama H.Case of the diffuse form of xanthogranulomatous pyelonephritis.Case Rep Urol 2013;2013. 936035.
[6]Goyal S,Gupta M,Goyal R.Xanthogranulomatous pyelonephritis:a rare entity.N Am J Med Sci 2011;3:249-50.
[7]Li L,Parwani AV.Xanthogranulomatous pyelonephritis.Arch Pathol Lab Med 2011;135:671-4.
[8]Khalid M,Ahmad M,Siddiqui MA,Khalid S.Diagnostic diff iculties in diffuse xanthogranulomatous pyelonephritis:a case report and review of the literature.Kidney Int 2010;19:73-5.
[9]Evans JA,Meyers MA,Bosniak MA.Acute renal and perirenal infections.Semin Roentgenol 1971;6:276-91.
[10]Arango O,Rosales A,Gelabert A.Xanthogranulomatous pyelonephritis with nephrocutaneous fistula at the knee.Br J Urol 1991;67:654-5.
Received 27 April 2015;received in revised form 11 October 2015;accepted 16 October 2015
Available online 7 November 2015
*Corresponding author.
E-mail address:guwa1986@gmail.com(R.T.Puthenveetil).
Peer review under responsibility of Shanghai Medical Association and SMMU.
http://dx.doi.org/10.1016/j.ajur.2015.10.005
2214-3882/ⓒ2016 Editorial Office of Asian Journal of Urology.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Nephrocutaneousfistula;
Xenthogranulomatouse
pyelonephritis
杂志排行

Asian Journal of Urology的其它文章
- A case of giant prostatic hyperplasia
- Tumour lysis syndrome:A rare acute presentation of locally advanced testicular cancer-Case report and review of literature
- Who needs further evaluations to diagnose upper urinary tract urothelial cancers among patients with abnormal findings by enhanced CT?
- Can intravesical prostatic protrusion predict bladder outlet obstruction even in men with good flow?
- Zoledronic acid combined with androgendeprivation therapy may prolong time to castration-resistant prostate cancer in hormone-naïve metastatic prostate cancer patients-A propensity scoring approach
- Prostate cancer volume associates with preoperative plasma levels of testosterone that independently predicts high grade tumours which show low densities(quotient testosterone/tumour volume)