Prostate cancer volume associates with preoperative plasma levels of testosterone that independently predicts high grade tumours which show low densities(quotient testosterone/tumour volume)
2016-04-27AntonioPorroAloPetrozzielloMtteoBrunelliFilippoMiglioriniGiovnniCimniDvieDeMrhiNioloLuykIreneTmniniBetrieCrusoMriCerrutoCluioGhimentonWlterArtini
Antonio B.Porro*,Alo Petrozziello,Mtteo Brunelli, Filippo MiglioriniGiovnni CimniDvie De Mrhi Niolo’e LuykIrene TmniniBetrie Cruso, Mri A.CerrutoCluio Ghimenton,Wlter Artini
aClinica Urologica,Ospedale Policlinico ed Ospedale Civile Maggiore,Azienda Ospedaliera Universitaria Integrata,Verona,Italy
bMedicina Interna/Endocrinologia,Ospedale Policlinico ed Ospedale Civile Maggiore,Azienda
Ospedaliera Universitaria Integrata,Verona,Italy
cAnatomia Patologica,Ospedale Policlinico ed Ospedale Civile Maggiore,Azienda Ospedaliera
Universitaria Integrata,Verona,Italy
dMedicina di Laboratorio,Ospedale Policlinico ed Ospedale Civile Maggiore,Azienda Ospedaliera Universitaria Integrata,Verona,Italy
Prostate cancer volume associates with preoperative plasma levels of testosterone that independently predicts high grade tumours which show low densities(quotient testosterone/tumour volume)
Antonio B.Porcaroa,*,Aldo Petrozziellob,Matteo Brunellic, Filippo Migliorinia,Giovanni Cacciamania,Davide De Marchia, Nicolo’de Luyka,Irene Tamaninia,Beatrice Carusod, Maria A.Cerrutoa,Claudio Ghimentonc,Walter Artibania
aClinica Urologica,Ospedale Policlinico ed Ospedale Civile Maggiore,Azienda Ospedaliera Universitaria Integrata,Verona,Italy
bMedicina Interna/Endocrinologia,Ospedale Policlinico ed Ospedale Civile Maggiore,Azienda
Ospedaliera Universitaria Integrata,Verona,Italy
cAnatomia Patologica,Ospedale Policlinico ed Ospedale Civile Maggiore,Azienda Ospedaliera
Universitaria Integrata,Verona,Italy
dMedicina di Laboratorio,Ospedale Policlinico ed Ospedale Civile Maggiore,Azienda Ospedaliera Universitaria Integrata,Verona,Italy
Total testosterone;
Tumour volume;
Prostate-specific
antigen;
Prostate cancer;
Pathology Gleason score
Objective:To investigate potential associations of preoperative total testosterone (TT)with tumor volume(TV)and grade of prostate cancer(PCa).
Methods:Patients who were under medications impacting on the hypothalamic-pituitaryadrenal-testis-prostate axis were excluded.TT was measured preoperatively at least 1 month after biopsies and TV was calculated on the removed prostate specimen.Other continuous variables included total prostate specific antigen(PSA),percentage of positive cores(P+)and weight(W)of the removed prostate.Patients were categorized according to the pathologic Gleason score(pGS)in 3 groups(pGS 6,7 and>7).Invasion of the seminal vesicles was coded as seminal vesicle invasion(SVI).
Results:The median levels of TT were significantly and increasingly higher from pGS 6(14.7 nmol/L)to pGS 7(15.0 nmol/L)and pGS>7(18.8 nmol/L).The median values of TV were also detected significantly and increasingly higher from pGS 6(5.6 mL)to pGS 7(8.1 mL)and pGS>7(14.8 mL).The median preoperative levels of PSA were also increasing from pGS 6(5.9 μg/L)to pGS 7(6.2 μg/L)and pGS>7(7.7 μg/L).There was a significant and positive correlation of TV to PSA,TT and P+.Multiple linear regression analysis showed that TV was significantly an d independently predicted by TT,PSA and P+.High grade PCa(p GS>7) independently associated with TV,TT,P+and SVI.The median density values of TT relative to TV(quotient TT/TV)significantly decreased from pGS 6(2.6 nmol/L/mL)to p GS 7 (1.9 nmol/L/mL)and pGS>7(1.4 nmol/L/mL).The median density values of PSA relative to TV(quotient PSA/TV)also significantly decreased from pGS(1.1 μg/L/mL)to p GS 7 (0.7 μg/L/mL)and pGS>7(0.6 μg/L/mL).
Conclusion:The investigation shows that TT relates to volume and grade of PCa;moreover,the density of TT relative to TV inversely associates with rate of increase of cancer that depends on the grade of the tumour.
ⓒ2016 Editorial Office of Asian Journal of Urology.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
1.Introduction
Biology of the prostate depends on the endocrine system which includes the hypothalamus,the pituitary gland,the adrenals and testes in which Leydig’s interstitial cells are responsible for the production of 95%of all circulating androgen in the form of testosterone.Androgens,estrogens and pituitary hormones regulate prostate physiology.
Actually,prostate cancer(PCa)is the most studied endocrine tumour which needs further clinical research in order to explore etiology and physiopathology factors relating to its natural history.The disease depends on the androgens[1]and increases the levels of prostate-specific antigen(PSA)[2,3].Since the pioneering work of Higgins and Hodges[1],androgens have been universally considered pivotal in the regulation of normal function and malignant growth of the prostate.Moreover,pretreatment total testosterone(TT)serum levels have been detected abnormal in the PCa population[4-7].It has also been hypothesized that PCa might produce a substance that alters the normal function of the pituitary-testicular-prostate axis which responds by abnormal luteinizing hormone(LH) and follicle-stimulating hormone(FSH)serum levels[4-11]. It has also been suggested that the impact of the disease on the hypothalamic-pituitary-testis-prostate axis may be more profound in high-grade tumours[11];however,the hypothesis has not been confirmed[12].The association of pretreatment TT levels with pathological Gleason score (pGS),which represents the most effective factor for predicting the natural history of the disease(biochemical recurrence,development of metastases and PCa specific mortality)[13-16],is still a controversial and unsettled subject area[4-7,10-12,17-29]which requires further research[30].
In PCa patients,the volume of the tumour(TV)has been related to metastasis,seminal vesicle invasion and loss of histological differentiation[31];moreover,high grade tumours(Gleason pattern 4 or 5)showed the highest rate to metastasize[31].As a consequence,the association of high grade PCa with TV might express the highest potential of aggressive disease.Actually,the potential association of preoperative TT with both TV and high grade PCa remains an unexplored area of clinical research which is subject of the present investigation.
2.Materials and methods
2.1.Patients
The present analysis was part of a study aimed at evaluating a potential link between PCa and the hypothalamic-pituitary-testis-prostate axis.The data of 220 operated patients were retrospectively reviewed.Standard retro-pubic radical prostatectomy(RRP)was the surgical procedure performed with or without limited local lymph node dissection(LND).All patients had not previously received 5α-reductase inhibitors,LH-releasing hormone analogues or testosterone replacement treatment.The 14-core transrectal ultrasound scan(TRUS)guided prostate biopsy technique was routinely used and additional cores were taken when a lesion on either TRUS or digital rectal examination was evident.The biopsy Gleason score(bGS) of positive cores was assessed and percentage of positive cores(P+)was computed.After informed signed consent, pretreatment simultaneous serum samples of TT and PSA were obtained from a cubital vein,at least 1 month after TRUS biopsy,between 8:00-8:30 a.m.The samples were analyzed at our laboratory.TT(normal range,9-29 nmol/L) and PSA(normal range,2-4 μg/L)were measured by immunochemiluminescent test performed by ADVIA Centaur XP Immunoassay System(Siemens Company, Munich,Germany).The study obtained Institutional Review Board approval.
2.2.Data collection
The prostatectomy specimens were fixed in toto overnight (10%neutral buffered formhaldeyde),coated with India ink and then weighted(W).Tissue sections of 4 μm wereprepared in standard fashion and stained with hematoxylin and eosin.Patients were classified according to primary tumour stage,lymph node and metastatic status,using the TNM categories recommended by the 1997 International Union Against Cancer TNM classification system[32].Seminal vesicle invasion(SVI)was defined as tumour involvement of the muscolar wall(pT3b).Bladder neck invasion was staged as pT3a.Surgical margins(R)were stated as free(R0)or involved by cancer(R1).Tumours were graded according to the Gleason grading system and the Gleason score was computed after summing up the two patterns, prevalent and secondary,structuring the tumour.High grade PCa was defined as pGS>7.The percentage of cancer volume(V+)was not directly measured but calculated by the experienced and dedicated pathologists.Overall V+ was related to the volume of the removed prostate(PV,mL) which was computed as the quotient W(prostate tissue specific weight=1.05).TV(mL)was calculated by multiplying PV and V+.It was also assessed the tumour rate which was defined as the median rate of increase of the mass(volume)of the tumour related to each unit increase of the pGS.
2.3.Statistical methods
Data on continuous variables are presented as medians with their respective ranges,and differences between groups analysed with the Mann-Whittney U test and Kruskal Wallis test.Data on categorical variables are presented as proportions,and differences between groups analysed with Pearson’s chi-squared or Fishers’exact test as appropriate. The association of TV was assessed by univariate and multivariate linear regression analysis which was preceded by evaluation of co-linearity of the covariates which included age,PSA,TT,P+and W.The associations of high grade PCa was investigated by the logistic regression model in which all variables were entered as continuous variables expect for SVI which was dichotomous(1=positive, 0=negative);moreover,the variables were grouped as clinical(PSA,TT,P+)and pathologic(TV,SVI).All tests are two-sided with p<0.05 considered to indicate statistical significance.

Table 1Variables in the PCa population and their association with pGS groups.
3.Results
Part of the clinical and pathologic characteristics of the cohort of cases has already been reported elsewhere [33,34].Table 1 reports the clinical and pathological factors of the cohort of patients who have been stratified according to the pGS.The clinical characteristics of the patient population are presented in Table 1.At the time of presentation,190 patients(98.2%)had clinically organconfined disease,the median(range)levels of PSA and TT were 6.2(1.2-44.2)μg/L and 15.5(5.5-40.7)nmol/L, respectively.The distribution of pGS was 6 in 88(40.0%),7 in 109(49.5%)and>7 in 23(10.5%)cases,and the median (range)of TV was 7.4(0.6-47.6)mL.
The clinical and pathological characteristics of the different pGS groups are also reported in Table 1 which shows increasing median values of PSA(p=0.056),TT (p=0.015),TV(p<0.0001),P+(p<0.0001)and decreasing values of W(p=0.001).The proportions of cT, bGS,pT,R and pN were also significantly different (p<0.0001).
As shown in Table 2,TV correlated with PSA(r=0.345, p<0.0001),TT(r=0.158,p=0.019)and P+(r=0.388, p<0.0001)which also correlated with PSA(r=0.215, p=0.001)and W(r=-0.302,p=0.0001).As reported in Table 3,multivariate linear regression analysis showed that PSA(p=0.0001),TT(p=0.012)and P+(p=0.0001)were independent predictors of TV.The functional relations of TV to TT and PSA are depicted in Fig.1(A)and(B),respectively.
Table 4 describes logistic regression results which showed that high grade cancer(pGS>7)independently associated with preoperative variables including PSA (p=0.023),TT(p=0.010)and P+(p=0.016)as well as with postoperative covariates including pT3b(p<0.0001) and TV(p=0.025).
To explore the association of both PSA and TT with tumour grade,we estimated the amount of PSA and TT produced per unit volume of tumour tissue,the quotients PSA/TV and TT/TV,by Gleason score in the 220 RRP specimens.As shown in Table 5,TV was closely related to pGS with median TV almost increasing three times from pGS 6 to pGS>7(p<0.0001).Although the increases of the median levels of TT,as shown in Fig.1(C),were significant (p=0.015),more than PSA(p=0.056),the rate of rise was less than TV,such that with increasing tumour rate,the amount of TT and PSA relative to unit volume of tumour dropped significantly(p<0.0001).

Table 2Correlations of TV in the operated prostate
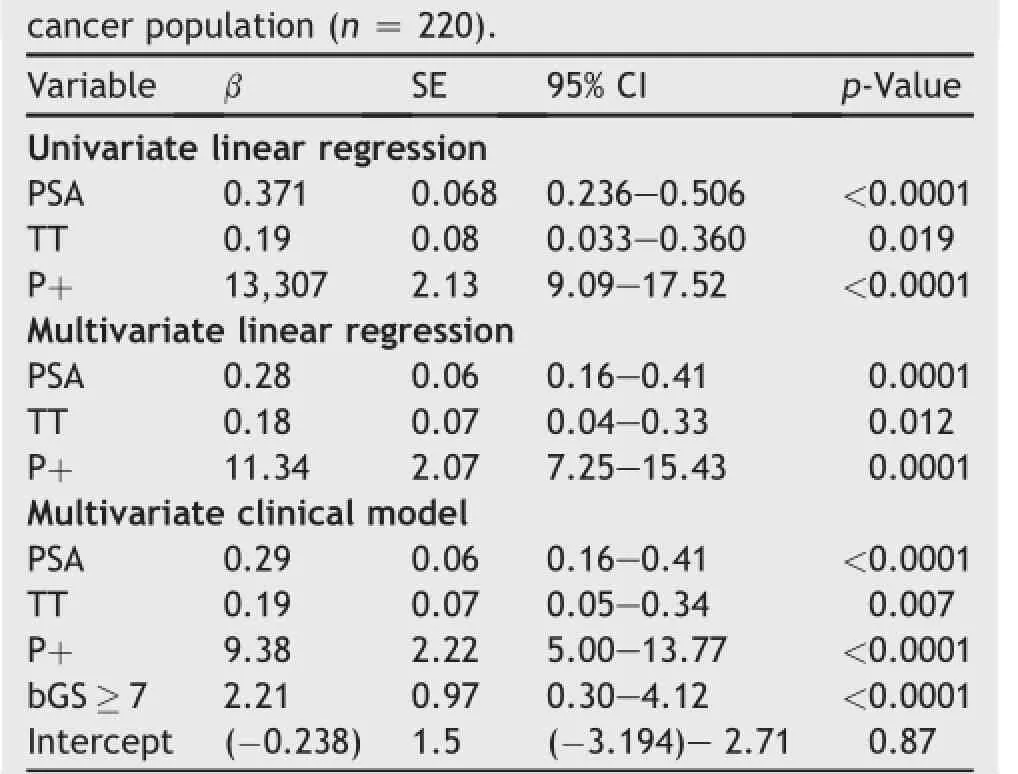
Table 3Covariates associating with TV in the prostate
4.Discussion

Figure 1The associations of TV with TT(A),TV with PSA(B),and TV as a function of the density(TT/TV)(C)are stratified by pGS groups.TV,tumour volume;TT,total testosterone;pGS,pathologic Gleason score;PSA,prostate specific antigen.
Prostate cancer volume has been related to grade and stage [35]as well as to PSA[2],PSA density(PSAD,quotient PSA/ prostate volume)and to the quotient PSA/TV[35].However,the relation of TV to TT serum levels has not yet been investigated.The present study shows functional relationships of PCa.Interestingly,TV was independently predicted by the preoperative covariates including PSA,TT and P+.Although significantly higher median values of both TT and PSA were detected in the pGS groups,the density of TT and PSA relative to TV(quotients TT/TV and PSA/TV) were inversely related to pGS.Indeed,in the pGS groups, the rate of rise of both PSA and TT was less than TV,such that with increasing tumour rate,the amount of TT and PSA relative to unit volume of tumour dropped significantly(see Fig.1(C)).As a consequence,high grade tumours,although associating with increased median levels of TT and PSA, express low TT and PSA densities relative to mass of the tumour.Probably,the three important steps in the natural history of PCa are:(i)the development of microfoci of incidental cancer,(ii)the progression from occult to significant localized disease,and(iii)metastasis to lymph nodes,bones or other organs.The progression of PCa from occult to clinically significant disease might be related to multiple genetic hits which are necessary for transformation into clinically significant cancer.The molecular biology that underlies the maintenance of androgen receptor (AR)activity in the early stages of PCa progression might be related to endocrine androgen dependence(state 1)and intracrine androgen dependence(state 2);indeed,in both states the drivers of AR pathway are androgens which are produced by the testes in state 1 and by PCa cells either from adrenal precursors or trough de novo metabolism in state 2[36].As a theory,the high TT/TV density of pGS 6 might be related to state 1(endocrine androgen dependence)and the low density of pGS 7 and>7 to state 2 (intracrine androgen dependence).Moreover,PSA is the ultimate androgen responsive gene and its incremental decline production in less differentiated tumours(low PSA/TV density)might also be related to intracrine androgen dependence.In our opinion,the present study gives evidence of how TV relates to pGS groups.
Tumour grade is the best predictor of PCa natural history after RP[13-16].The topic dealing with the association of preoperative TT levels and tumour grade is controversial. Indeed,studies investigating on the potential relation of TT to tumour grade have shown that the former might or might not be associated with the latter;moreover,when the relation was significant,both lower and higher mean serum levels of TT related to high grade tumours as well[30].Ourstudy showed that higher median levels of TT were detected in high grade PCa(pGS>7),but it is difficult to compare with other studies showing the opposite.Indeed,the results of studies stating that significantly lower levels of TT are detected in high grade tumours have to be evaluated by the criteria employed to group the patient population.For example,Zhang et al.[27]demonstrated that significantly lower levels of TT were detected in high grade PCa tumours;however if we consider the methodological criteria which were employed,we see that tumour grades were assessed according to the limitations of the bGS,also,high grade tumours included 8-9 groups and“moderate cancers”included bGS 5-7.In our opinion,before trying tofind out significant associations of lower serum levels with high grade tumours,an evident and independent association between TT serum levels and the GS groups has to be assessed.The present investigation shows the close association of TT with both volume and grade of the tumour. Although low and high levels of TT may be assessed in the pGS groups,the levels of TT which may be low or high, relate differently to TV measurements in the p GS groups. Indeed,tumours having same volume measurements associate with different serum levels of TT in the pGS groups.For example,PCa related to TV of 10 mL associate with lower TT levels in high-intermediate cancers compared to pGS 6 tumours.As a theory,TT is closely related to the tumour phenotype,while PSA is the product of the ultimate responsive gene depending on TTwhich is a stimulatory growth factor for the cancer cell population. Tumour grading related to both TT and TV might identify different degrees of hormone dependence in the pGS groups;indeed,low-intermediate grade tumours probably contain a higher proportion of androgen dependent cancer cells in their population and high grade groups might include a cancer population which is predominantly androgen independent.The findings of the present study might explain why higher levels of calculated FT,which depends on TT,were associated with an increased risk of aggressive PCa among older men[37].The study also stresses the importance of preoperative serum TT along the hypothalamic-pituitary-testis-prostate axis in which hormonal and PSA dynamics will change after radical prostatectomy[4-11].

Table 4Covariates associating with pGS>7.

Table 5Analysis of PSA and TT production per unit volume of tumour by Gleason grade.
There are several limitations to the present investigation.Firstly,although the data were collected prospectively,it was analyzed retrospectively.In addition,the volumes measured by TRUS were incomplete,and so PSAD was not included in the analysis;however,results related to PSAD could have been confirmatory of what has been widely reported from the literature.
The third limit might be related to the methodology employed to measure TV;however,the computation is simple and reproducible and the results are close to what has been reported in the literature[31,32].The measurement of V+is standard in daily pathology practice and it was computed by experienced pathologists;moreover,it was related to tumour volume according to the methodology described.The analysis confirmed that the computations were reliable and significantly related to the preoperative and pathologic variables.We did not directly measure TV by sophisticated and complex methodologies which are also difficult to reproduce in clinical practice because the main goalofthe study was assess thisparameter indirectly in order to be reproducible in each urologic unit that has dedicated pathologists and there is each other feed-back in approaching prostate cancer.However,TV and pT both independently associated with pGS which is the strongest predictor PCa natural history.Fourth,although there were only 23 with pGS>7 which is 10%ofthe cohort,the group that was classified by pGS>7 was really the high grade group of the cohort according to the new classification system of PCa that has been proposed by the International Society of Urologic Pathology(ISUP)Consensus Conference[38].
Although our multivariate models might be unstable because of wide confidence intervals,confirmatory studies of our results are required.However,multiple analyses have been computed in order to show that the pathologic variables including TV and pT as well as the clinical factors including TT,PSA and P+independently associated with pGS which is the strongest recognized predictor of the natural history of prostate cancer.Finally,comparing and confirmatory studies are missing.However,in our opinion, the topic has been approached in an advanced way and the results are interesting for evaluating and managing clinical PCa.
In summary,we have determined that preoperative TT relates to volume and grade of PCa;moreover,the quotient TT/TV(density)inversely associates with the rate of increase of the tumour that also associates with PCa grade.TT might be a potential marker for assessing preoperatively the volume and grade of PCa.These findings might have obvious implications in clinical practice;however,confirmatory studies are required in this controversial research area.
Conflicts of interest
The authors declare no conflict of interest.
[1]Huggins C,Hodges CV.Studies on prostate cancer.I:the effect of castration,of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate.Cancer Res 1941;1:293-7.
[2]Stamey TA,Yang N,Hay AR,McNeal JE,Freiha FS,Redwine E. Prostate-specific antigen as a serum marker for adenocarcinoma of the prostate.N Engl J Med 1987;317:909-16.
[3]Armbruster DA.Prostate-specific antigen:biochemistry, analytical methods,and clinical application.Clin Chem 1993; 39:181-95.
[4]Miller LR,Partin AW,Chan DW,Bruzek DJ,Dobs AS,Epstein JI, et al.Influence of radical prostatectomy on serum hormone levels.J Urol 1998;160:449-53.
[5]Olsson M,Ekstrom L,Schulze J,Kjellman A,Akre O,Rane A, et al.Radical prostatectomy:influence on serum and urinary androgen levels.Prostate 2010;70:200-5.
[6]Harper ME,Pierrepoint CG,Griffiths K.Carcinoma of the prostate:relationship of pretreatment hormone levels to survival.Eur J Cancer Clin Oncol 1984;20:477-82.
[7]Chen SS,Chen KK,Lin AT,Chang YH,Wu HH,Chang LS.The correlation between pretreatment serum hormone levels and treatment outcome for patients with prostatic cancer and bony metastasis.BJU Int 2002;89:710-3.
[8]Hammond GL,Kontturi M,Maattala P,Puukka M,Vihko R. Serum FSH,LH and prolactin in normal males and patients with prostatic diseases.Clin Endocrinol 1977;7:129-35.
[9]Kumar VL,Wafhwa SN,Kumar V,Farooq A.Androgen,estrogen,and progesterone receptor contents and serum hormone profiles in patients with benign hypertrophy and carcinoma of the prostate.J Surg Oncol 1990;44:122-8.
[10]Hilz H,Graefen M,Noldus J,Hammerer P,Knabbe C,Huland E, et al.Advanced prostate cancer is associated with a decrease in serum luteinizing hormone.Eur Urol 2000;38:243-9.
[11]Madersbacher S,Shatzl G,Bieglmayer C,Reiter BW, Gassner C,Berger P,et al.Impact of radical prostatectomy and TURP on the hypothalamic-pituitary-gonadal axis.Urology 2002;60:869-74.
[12]Fodstad P,Bjoro T,Torlakovic G,Fossa SD.No association of serum gonadal or pituitary hormone with prognostic parameters in stages T1 to T3 pN0M0 prostate cancer.J Urol 2002; 168:1188-92.
[13]Pound CR,Partin AW,Eisenberger M,Chan DW,Pearson JD, Walsh PC.Natural history of progression after PSA elevation following radical prostatectomy.J Am Med Assoc 1999;281: 1591-7.
[14]Hull GW,Rabbani F,Abbas FA,Wheeler TM,Kattan MW, Scardino PT.Cancer control with radical prostatectomy alone in 1,000 consecutive patients.J Urol 2002;167:528-34.
[15]Freedland SJ,Humphreys EB,Mangold LA,Eisenberger M, Dorey FJ,Walsh PC,et al.Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy.J Am Med Assoc 2005;294:433-9.
[16]Cuzik J,Fisher G,Kattan MW,Berney D,Oliver T,Foster CS, et al.Long-term outcome among men with conservatively treated localised prostate cancer.Br J Cancer 2006;95: 1186-94.
[17]Monda JM,Myers RP,Bostwick DG,Oesterling JE.The correlation between serum prostate-specific antigen and prostate cancer is not influenced by the serum testosterone concentration.Urology 1995;46:62-4.
[18]Ide H,Yasuda M,Nishio K,Saito K,Isotani S,Kamiyama Y, et al.Development of a nomogram for predicting high-grade prostate cancer on biopsy:the significance of serum testosterone levels.Anticancer Res 2008;28:2487-92.
[19]Anderson SO,Adami HO,Bergstrom R,Wide B.Serum pituitary and sex steroid hormone levels in the etiology of prostatic cancer-a population-based case control study.Br J Cancer 1993;68:97-102.
[20]Schatzl G,Madersbacher S,Thurridl T,Waldmuller J, Kramer G,Haitel A,et al.High-grade prostate cancer is associated with low serum testosterone levels.Prostate 2001; 47:52-8.
[21]Severi G,Morris HA,MacInnis RJ,English DR,Tilley W, Hopper JL,et al.Circulating steroid hormones and the risk of prostate cancer.Cancer Epidemiol Biomarkers Prev 2006;15: 86-91.
[22]Mikkola AK,Aro JL,Rannikko SA,Salo JO.Pretreatment plasma testosterone and estradiol levels in patients with locally advanced or metastatized prostate cancer.FINNPROSTATE group.Prostate 1999;39:175-81.
[23]Salonia A,Gallina A,Briganti A,Suardi N,Capitanio U, Abdollah F,et al.Circulating estradiol,but not testosterone is a signficant predictor of high-grade prostate cancer in patients undergoing radical prostatectomy.Cancer 2011;117: 5029-38.
[24]Sher DJ,Mantzoros C,Jacobus S,Regan MM,Lee GS,Oh WK. Absence of relationship between steroid hormone levels and prostate cancer tumour grade.Urology 2009;73:356-61.
[25]Takizawa I,Nishiyama T,Hara N,Isahaya E,Hoshii T, Takahashi K.Serum prostate specific antigen levels reflect the androgen milieu in patients with localized prostate cancer receiving androgen deprivation therapy:tumour malignant potential and androgen milieu.Prostate 2010;70:1395-401.
[26]Hoffman MA,Dewolf WC,Morgentaler A.Is low serum free testosterone a marker for high grade prostate cancer?J Urol 2000;163:824-7.
[27]Zhang PL,Rosen S,Veeramachaneni R,Kao J,Dewolf WC, Bubley G.Association between prostate cancer and serum testosterone levels.Prostate 2002;53:179-82.
[28]Lane BR,Stephenson AJ,Magi-Galluzzi C,Lakin MM.low testosterone and risk of biochemical recurrence and poorly differentiated prostate cancer at radical prostatectomy. Urology 2008;72:1240-5.
[29]Kratzick C,Womastek I,Bieglmayer C,Schatzl G,Lackner J, Freibauer C,et al.Lower serum total testosterone is associated with lymph node metastases in radical prostatectomy cohort study.Anticancer Res 2011;31:3615-8.
[30]Klap J,Schmid M,Loughlin K.The relationship between total testosterone levels and prostate cancer:a review of the continuing controversy.J Urol 2015;193:403-14.
[31]McNeal JE,Bostwick DG,Kindrachuk RA,Redwine EA, Freiha F,Stamey TA.Patterns of progression in prostate cancer.Lancet 1986;1:60-3.
[32]Flemming ID,Cooper JS,Henson DE,Hutte RVP,Kennedy BJ, Murphy GP,et al.,editors.American joint committee on cancer staging manual.5th ed.Philadelphia:JP Lippincott; 1997.p.219-22.
[33]Porcaro AB,Petrozziello A,Ghimenton C,Migliorini F,Sava T, Caruso B,et al.Serum total testosterone is a significant preoperative variable independently contributing to separating the prostate cancer population into prostatectomy Gleason score groups.Urol Int 2013;91:55-61.
[34]Porcaro AB,Petrozziello A,Ghimenton C,Migliorini F,Sava T, Caruso B,et al.Associations of pretreatment serum total testosterone measurements with pathology-detected Gleason score cancer.Urol Int 2014;93:269-78.
[35]Corcoran NM,Casey RG,Hong MKH,Pedersen J,Connolly S, Peters J,et al.The ability of prostate-specific antigen(PSA) density to predict an upgrade in Gleason score between initial prostate biopsy and prostatectomy diminishes with increasing tumour grade due to reduced PSA secretion per unit tumour volume.BJUI 2011;110:36-42.
[36]Nelson PS.Molecular states underlying androgen receptor activation:a framework for therapeutics targeting androgen signaling in prostate cancer.J Clin Oncol 2012;30:644-6.
[37]Pierorazio PM,Ferrucci L,Kettermann A,Longo DL,Metter EJ, Carter HB.Serum testosterone is associated with aggressive prostate cancer in older men:results from the Baltimore longitudinal study of aging.BJUI 2009;105:824-9.
[38]Epstein JI,Egevad L,Amin MB,Delahunt B,Srigley JR, Humphrey PA,et al.The 2014 international sociaty of urologic pathology(ISUP)consensu conference on Gleason grading of prostate carcinoma.Definition of grading pattern and proposal for a new grading system.Am J Surg Pathol 2015 Oct 21 [Epub ahead of print].
Received 21 August 2015;received in revised form 9 September 2015;accepted 3 November 2015
Available online 30 November 2015
*Corresponding author.
E-mail address:drporcaro@yahoo.com(A.B.Porcaro).
Peer review under responsibility of Shanghai Medical Association and SMMU.
http://dx.doi.org/10.1016/j.ajur.2015.11.006
2214-3882/ⓒ2016 Editorial Office of Asian Journal of Urology.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
杂志排行

Asian Journal of Urology的其它文章
- Unusual case of nephrocutaneous fistula-Our experience
- A case of giant prostatic hyperplasia
- Tumour lysis syndrome:A rare acute presentation of locally advanced testicular cancer-Case report and review of literature
- Who needs further evaluations to diagnose upper urinary tract urothelial cancers among patients with abnormal findings by enhanced CT?
- Can intravesical prostatic protrusion predict bladder outlet obstruction even in men with good flow?
- Zoledronic acid combined with androgendeprivation therapy may prolong time to castration-resistant prostate cancer in hormone-naïve metastatic prostate cancer patients-A propensity scoring approach