血压变异性与高血压小卒中患者急性期神经功能恶化的关系
2015-11-18王渝朱炬张哲成张静田丽王玉文孙弦
王渝,朱炬,张哲成,张静,田丽,王玉文,孙弦
血压变异性与高血压小卒中患者急性期神经功能恶化的关系
王渝,朱炬,张哲成△,张静,田丽,王玉文,孙弦
目的探讨血压变异性(BPV)与高血压小卒中患者急性期神经功能恶化的关系。方法选取高血压小卒中患者200例,根据患者是否发生急性期神经功能恶化分为稳定组(182例)和恶化组(18例),比较2组患者24 h动态血压监测的BPV,24 h收缩压血压变异系数(24 h CVSBP)、24 h舒张压血压变异系数(24 h CVDBP)、白昼收缩压血压变异系数(dCVSBP)、白昼舒张压血压变异系数(dCVDBP)、夜间收缩压血压变异系数(nCVSBP)、夜间舒张压血压变异系数(nCVDBP)。采用Binary Logistic回归分析高血压小卒中患者急性期神经功能恶化的BPV相关因素。结果与稳定组比较,恶化组24 h CVSBP为17.75%(17.54%,19.26%)vs 12.78%(10.67%,14.39%)、24 h CVDBP为25.48%(20.77%,27.87%)vs 17.95%(14.88%,21.46%)、dCVSBP为18.61%(17.65%,20.65%)vs 12.30%(10.10%,14.75%)、dCVDBP为25.65%(21.25%,29.78%)vs 17.76%(14.89%,22.19%)均升高,差异有统计学意义(均P<0.01)。Binary Logistic回归分析显示24 h CVSBP、dCVSBP是高血压小卒中患者急性期神经功能恶化的危险因素。结论24 h BPV和白昼BPV增加可能与高血压小卒中患者急性期神经功能恶化有关,在卒中急性期和二级预防中应关注BPV。
脑梗死;高血压;监护;血压测定;脑缺血发作,短暂性;卒中;预后;血压变异性
缺血性卒中患者在发病后数小时至数天内常发生急性神经功能恶化,其发生率为12%~42%[1]。小卒中在症状达峰时患者仅表现为轻微稳定的神经功能缺损[2],易被患者和临床医生所忽视。中国国家卒中登记(CNSR)研究显示小卒中急性期神经功能恶化的风险高达15.2%[3],而高血压是小卒中近期恶化的重要危险因素[4]。备受国际关注的急性脑出血强化降压试验2(INTERACT2)研究结果提示血压变异性(blood pressure variability,BPV)与出血性卒中的预后相关[5]。皮层下小卒中二级预防(SPS3)研究提示降压有减少卒中风险的趋势[6]。因此,探讨国人BPV与高血压小卒中急性期神经功能转归的关系意义重大。本文通过检测不同神经功能转归的高血压小卒中患者的BPV,旨在研究其与小卒中急性期神经功能恶化的关系。
1 资料与方法
1.1 一般资料选取2012年12月—2013年12月于我科住院的高血压小卒中患者(发病24 h之内)200例,经头颅CT或MRI证实为脑梗死,美国国立卫生院脑卒中量表(NIHSS)评分≤3分,有明确原发性高血压病史或入院后2次测量血压收缩压≥140 mmHg(1 mmHg=0.133 kPa)和(或)舒张压≥90 mmHg。获得患者本人或家属知情同意。根据患者是否发生急性期神经功能恶化分为神经功能稳定组(稳定组)和急性期神经功能恶化组(恶化组)。其中稳定组182例(91.0%),男120例,女62例,年龄(69.85±5.02)岁;恶化组18例(9.0%),男10例,女8例,年龄(71.56±5.58)岁;2组患者性别(χ2=0.776)、年龄(t=1.364)差异无统计学意义。排除标准:(1)继发性高血压。(2)有明确的心源性栓子来源(房颤或心脏瓣膜病变)或由于血管畸形造成的卒中。(3)已经发生的严重痴呆(MMSE<22分)、严重抑郁(HAMD≥24分)或严重失语影响随访评价。(4)正在参加其他临床试验研究。急性期神经功能恶化定义为出院时或住院第14天时NIHSS评分增加2分或以上[3]。
1.2 方法记录患者的入院血压,是否吸烟、饮酒,有无冠心病、糖尿病,检测总胆固醇(TC)及血浆总同型半胱氨酸(tHcy)水平,计算入院NIHSS评分。观察研究期间指导受试者按照目前指南[7]实施规范抗血小板聚集、控制血压、控制血糖、调节血脂、戒烟、限制饮酒等措施。
1.3 BPV监测与评价住院第3~7天患者采用非瘫痪侧上臂佩带日本A&D CO.LTD公司TM-2430型无创便携式动态血压监测仪进行24 h动态血压监测。血压测量从7:00—22:00,每30 min测量1次,从22:00至次日7:00,每60 min测量1次,记录24 h动态血压值。有效测量范围为收缩压70~260 mmHg,舒张压40~150 mmHg,有效血压测量值数不少于应测次数的80%,否则视为无效。记录24 h收缩压血压变异系数(24 h CVSBP)、24 h舒张压血压变异系数(24 h CVDBP)、白昼收缩压血压变异系数(dCVSBP)、白昼舒张压血压变异系数(dCVDBP)、夜间收缩压血压变异系数(nCVSBP)、夜间舒张压血压变异系数(nCVDBP)。
1.3 统计学方法采用SPSS 21.0统计软件进行分析。计数资料以例(%)表示,采用χ2检验;正态分布计量资料以均数±标准差表示,采用t检验;偏态分布资料采用M(P25,P75)表示,组间比较采用Mann-Whitney检验。影响因素分析采用条件Binary Logistic回归逐步法分析。P<0.05为差异有统计学意义。
2 结果
2.1 2组患者一般资料比较2组患者吸烟史、饮酒史、冠心病史、TC、tHcy、入院NIHSS评分、入院收缩压、入院舒张压差异均无统计学意义(均P>0.05)。恶化组有糖尿病史患者比例较稳定组高,差异有统计学意义(P<0.05),见表1。
2.2 2组患者BPV比较见表2。恶化组患者24 h CVSBP、24 h CVDBP、dCVSBP、dCVDBP较稳定组升高,差异有统计学意义(均P<0.01),2组患者nCVSBP、nCVDBP差异无统计学意义(均P>0.05)。
2.3 BPV影响因素的回归分析以患者是否存在急性期神经功能恶化为应变量(恶化=1,未恶化= 0),以24 h CVSBP、24 h CVDBP、dCVSBP、dCVDBP、nCVSBP、nCVDBP为自变量,采用非条件Binary Logistic回归逐步法筛选自变量,结果显示24 h CVSBP、dCVSBP为急性期神经功能恶化的危险因素,见表3。

Tab.1 Comparison of general data between stable group and deterioration group表1 稳定组和恶化组患者一般资料比较

Tab.2 Comparison of BPV parameters between stable group and deterioration group表2 稳定组和恶化组患者BPV比较[%,M(P25,P75)]
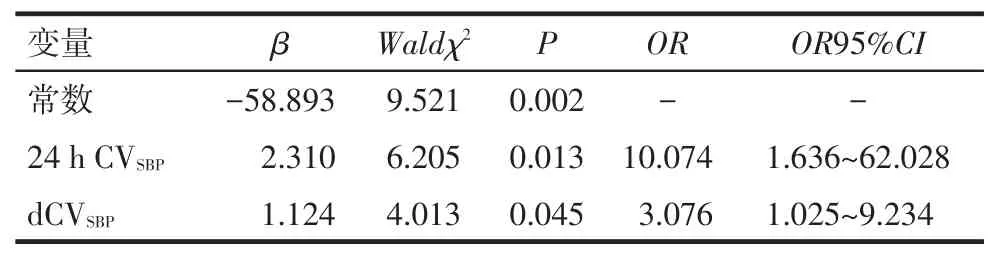
Tab.3 Results of binary logistic regression analysis of the BPV factors affecting neurological deterioration during the acute phase表3 急性期神经功能恶化BPV相关因素的Binary Logistic回归分析结果
3 讨论
小卒中属于急性非致残性脑血管事件,主要以NIHSS≤3分作为其定义标准[2]。实践证实小卒中患者是早期神经功能恶化乃至残障卒中的高危人群[8]。小卒中发生早期神经功能恶化的预测因素包括高血压、糖尿病、合并急性感染、心脏失代偿等,恶化组合并糖尿病患者比例较稳定组高,与先前研究结果相一致[4]。然而关于强化降压与预后的INTERACT2和SPS3两大国际多中心研究并未降低主要终点事件,但事后亚组分析强烈提示BPV与卒中预后可能有关[5-6],故靶向研究卒中后BPV对卒中预后的影响十分重要。
不同研究中小卒中发生早期神经功能恶化的风险不同。Ferrari等[4]对奥地利卒中单元登记库中的8 291例小卒中和短暂性脑缺血发作患者研究发现小卒中患者在卒中单元期间(平均2.97 d)发生早期神经功能恶化风险为4.5%。中国国家卒中登记(CNSR)研究显示,小卒中急性期神经功能恶化的风险高达15.2%[3]。而本研究显示高血压小卒中患者发生急性期神经功能恶化率为9.0%。所选人群、基线神经功能缺损程度、样本量大小、评价神经功能恶化的时间点不同导致了神经功能恶化风险的差异。
在ASCOT-BPLA研究中,随诊期间收缩压变异系数和24 h动态血压中的dCVSBP均能够很好地预测卒中发生的风险[9]。2011年Geeganage等[10]回顾性分析TAIST病例数据发现收缩压BPV与发病第10天卒中神经功能恶化相关。Buratti等[11]对颈内动脉闭塞的急性缺血性卒中患者的BPV进行研究显示缺血性卒中急性期BPV与发病后3个月的改良Rankin量表不良预后有关。目前国内关于BPV与小卒中早期神经功能恶化的关系尚少见报道。本研究发现恶化组患者24 h CVSBP、24 h CVDBP、dCVSBP、dCVDBP较稳定组升高,Binary Logistic回归分析显示24 h CVSBP、dCVSBP是高血压小卒中患者急性期神经功能恶化的危险因素,提示高血压小卒中患者急性期24 h BPV和白昼BPV增加,特别是24 h CVSBP、dCVSBP增加可能与急性期神经功能恶化有关。其机制可能为在缺血性卒中急性期,脑血流自身调节功能受损,脑血流完全依赖体循环血压,血压波动对脑缺血区域造成不良影响,尤其在小血管结构或功能受损时更加明显[11];BPV增加可导致血管结构和功能受损,增加颈动脉内膜中层厚度,从而导致靶器官损害和脑卒中发生[12]。此外,还可能与高血压患者清晨BPV异常增加,形成了血压晨峰和异常血压昼夜节律有关[13]。高血压治疗的目的是预防和逆转靶器官损害,因此,对于高血压小卒中患者,在急性期和二级预防中,不仅要使患者血压达标,还要更多地去关注血压的波动程度以及血压昼夜节律的变化,实现长期平稳降压,恢复正常血压昼夜变化,从而能更好地减少靶器官损害事件的发生[14]。临床医生可以通过结合动态血压监测,选择长效降压药,合理联合用药来实现24 h长效平稳降压,从而降低患者急性期神经功能恶化的风险。
综上所述,24 h BPV和白昼BPV增加可能与高血压小卒中患者急性期神经功能恶化有关。本研究例数较少,仅探讨了高血压小卒中患者急性期神经功能恶化与短时BPV的关系,未监测长时BPV,尚有不足之处,BPV与高血压小卒中患者急性期神经功能恶化的关系尚需更大规模的临床研究。
[1]Tei H,Uchiyama S,Ohara K,et al.Deteriorating ischemic stroke in 4 clinical categories classified by the Oxfordshire Community Stroke Project[J].Stroke,2000,31(9):2049-2054.doi:10.1161/01. STR.31.9.2049.
[2]Fischer U,Baumgartner A,Arnold M,et al.What is a minor stroke[J]?Stroke,2010,41(4):661-666.doi:10.1161/STROKEAHA.109.572883.
[3]Ju Y,Zhao XQ,Wang CX,et al.Neurological deterioration in the acute phase of minor ischemic stroke is an independent predictor of poor outcomes at 1 year:results from the China National Stroke Reg⁃istry(CNSR)[J].Chin Med J(Engl),2013,126(18):3411-3416.doi:10.3760/cma.j.issn.0366-6999.20130634.
[4]Ferrari J,Knoflach M,Kiechl S,et al.Early clinical worsening in pa⁃tients with TIA or minor stroke:the Austrian Stroke Unit Registry[J].Neurology,2010,74(2):136-141.doi:10.1212/WNL.0b013e31 81c9188b.
[5]Manning L,Hirakawa Y,Arima H,et al.Blood pressure variability and outcome after acute intracerebral haemorrhage:a post-hoc anal⁃ysis of INTERACT2,a randomised controlled trial[J].Lancet Neu⁃rol,2014,13(4):364-373.doi:10.1016/S1474-4422(14)70018-3.
[6]SPS3 Study Group,Benavente OR,Coffey CS,et al.Blood-pressure targets in patients with recent lacunar stroke:the SPS3 randomised trial[J].Lancet,2013,382(9891):507-515.doi:10.1016/S0140-6736(13)60852-1.
[7]Ischemic Stroke Second Prevention Guidelines Writing Group in Chinese Society of Neurology Cerebrovascular Disease Group.Chi⁃nese guidelines for the secondary prevention of ischemic stroke and transient ischemic attack 2010[J].Chin J Neurol,2010,43(2):1-7.[中华医学会神经病学分会脑血管病学组缺血性脑卒中二级预防指南撰写组.中国缺血性脑卒中和短暂性脑缺血发作二级预防指南2010[J].中华神经科杂志,2010,43(2):1-7].doi:10.3760/ cma.j.issn.1006-7876.2010.02.
[8]Coutts SB,Modi J,Patel SK,et al.What causes disability after tran⁃sient ischemic attack and minor stroke?Results from the CT and MRI in the Triage of TIA and minor Cerebrovascular Events to Iden⁃tify High Risk Patients(CATCH)Study[J].Stroke,2012,43(11):3018-3022.doi:10.1161/STROKEAHA.112.665141.
[9]Rothwell PM,Howard SC,Dolan E,et al.Prognostic significance of visit-to-visit variability,maximum systolic blood pressure,and epi⁃sodic hypertension[J].Lancet,2010,375(9718):895-905.doi:10.1016/S0140-6736(10)60308-X.
[10]Geeganage C,Tracy M,England T,et al.Relationship between base⁃line blood pressure parameters(including mean pressure,pulse pressure,and variability)and early outcome after stroke:data from the Tinzaparin in Acute Ischaemic Stroke Trial(TAIST)[J].Stroke,2011,42(2):491-493.doi:10.1161/STROKEAHA.110.596163.
[11]Buratti L,Cagnetti C,Balucani C,et al.Blood pressure variability and stroke outcome in patients with internal carotid artery occlusion[J].J Neurol Sci,2014,339(1-2):164-168.doi:10.1016/j.jns.20 14.02.007.
[12]Chen Y,Yuan RY,Li GP,et al.The relationship between ambulato⁃ry arterial stiffness index and target organ damage in patients with primary hypertensive[J].Tianjin Med J,2014,42(5):899-902.[陈云,袁如玉,李广平,等.动态动脉硬化指数的相关因素及其对靶器官损害的研究[J].天津医药,2014,42(5):899-902].doi:10.3969/j.issn.0253-9896.2014.05.021.
[13]Kario K.Morning surge in blood pressure and cardiovascular risk:evidence and perspectives[J].Hypertension,2010,56(5):765-773. doi:10.1161/HYPERTENSIONAHA.110.157149.
[14]Li Q,Wu J.Development history of hypertension and stroke[J].Chin J Contemp Neurol Neurosurg,2015,15(1):5-9.[李青,武剑.高血压与脑卒中发展史[J].中国现代神经疾病杂志,2015,15(1):5-9].doi:10.3969/j.issn.1672-6731.2015.01.003.
(2014-12-16收稿2015-05-07修回)
(本文编辑魏杰)
The relationship between blood pressure variability and neurological deterioration during the acute phase in hypertensive minor ischemic stroke patients
WANG Yu,ZHU Ju,ZHANG Zhecheng,ZHANG Jing,TIAN Li,WANG Yuwen,SUN Xian
Department of Neurology,Tianjin Third Central Hospital,Tianjin 300170,China△
ObjectiveTo investigate the relationship between blood pressure variability(BPV)and neurological deteri⁃oration(ND)during the acute phase in patients with hypertensive minor ischemic stroke.MethodsA total of 200 hyperten⁃sive patients with acute minor ischemic stroke were recruited in this study.Patients were divided into two groups:stable group(n=182)and deterioration group(n=18)according to the neurological prognosis.Values of BPV in 24 h ambulatoryblood pressure,24 h systolic blood pressure variation coefficient(24 h CVSBP),24 h diastolic blood pressure variation coeffi⁃cient(24 h CVDBP),day time systolic blood pressure variation coefficient(dCVSBP),day time diastolic blood pressure variation coefficient(dCVDBP),night time systolic blood pressure variability(nCVSBP)and night time diastolic blood pressure variability(nCVDBP)were compared between two groups.The related factors of BPV were analyzed by binary logistic method in the acute phase of patients with hypertensive minor ischemic stroke.ResultsThere were significantly higher levels of 24 h CVSBP[17.75%(17.54%,19.26%)vs 12.78%(10.67%,14.39%)],24 h CVDBP[25.48%(20.77%,27.87%)vs 17.95%(14.88%,21.46%)],dCVSBP[18.61%(17.65%,20.65%)vs 12.30%(10.10%,14.75%)],dCVDBP[25.65%(21.25%,29.78%)vs 17.76%(14.89%,22.19%)]in deterioration group than those of stable group(P<0.01).Results of binary logistic regression analysis showed that values of 24 h CVSBPand dCVSBPwere risk factors for neurological deterioration in the acute phase of patients with hypertensive minor ischemic stroke.ConclusionThe increased 24 h BPV and day time BPV are correlated with neurologi⁃cal deterioration during the acute phase in hypertensive minor ischemic stroke patients.BPV should be concerned in the acute phase and secondary prevention in patients with ischemic stroke.
brain infarction;hypertension;custodial care;blood pressure determination;ischemic attack,transient;stroke;prognosis;blood pressure variability
R743.32
A
10.11958/j.issn.0253-9896.2015.09.014
天津市卫生局科技基金资助项目(2012KR03)
天津市第三中心医院神经内科(邮编300170)
王渝(1983),男,主治医师,硕士,主要从事脑血管病、神经电生理方面研究
△通讯作者E-mail:zzc0912@126.com