大范围主动脉夹层3.0T两段式双期三维对比增强MR血管成像技术与临床价值
2015-09-26潘碧涛潘希敏胡美玉江波
潘碧涛,潘希敏,胡美玉,江波*
大范围主动脉夹层3.0T两段式双期三维对比增强MR血管成像技术与临床价值
潘碧涛1,潘希敏2,胡美玉2,江波1*
作者单位:
1. 中山大学附属第一医院放射诊断科,广州 510080
2. 中山大学附属第一医院东院放射科,广州 510700
目的 探讨大范围主动脉夹层 (AD) 3.0T两段式双期 3D CEMRA的扫描技术特点与诊断意义。材料与方法 14例大范围AD患者行循环时间 (TT)测试和3D FLASH-turbo MRA序列3D CEMRA连续2期扫描。比较真、假腔在TT、峰值信号(SPE)和3D CEMRA信号方面的差异;观测AD双腔的双期显影、内膜破口及腹主动脉分支与双腔的关系,结果与主动脉DSA对照。结果 AD真、假腔TT分别为(13.4±4.8) s、(17.5±4.7) s (P<0.01);峰值信号分别为108.7±28.4、83.5±39.3 (P<0.05)。真、假腔双期3D CEMRA信号分别为第一期:391.4±83.7、142.9±77.2 (P<0.01);第二期:225.0±66.1、231.6±80.0 (P>0.50)。双期3D CEMRA上AD双腔呈特征性动态显现:第一期,真腔全程显影,假腔节段性显影;第二期,真腔信号减退,假腔全程显影。检出内膜破口23个,数量、位置与DSA一致;8个呈血流喷射征。5条左肾动脉、3条右肾动脉和1条腹腔动脉干开口于假腔。结论 基于AD双腔血流动力学差异的TT测试和双期扫描,是大范围AD 3.0T两段式双期3D CEMRA的技术要点,该方法可满足大范围AD的诊断要求。
主脉瘤;磁共振血管造影术;动态
大范围主动脉夹层(aortic dissection,AD)是指夹层累及降主动脉全段和(或)升主动脉,其特点是纵向病变广,包括DebakeyⅠ型和ⅢB型。三维增强MR主动脉造影(3D CEMRA)在AD的诊断中起着重要作用[1-3],在自动移床技术出现以前,对于大范围AD一般采用胸、腹两段分别独立成像,耗时又加大患者的不适性,同时图像缺乏整体感与连续性。应用两段式扫描获取连续完整资料的3D CEMRA,评价大范围AD的可行性与有效性如何,少见报道。
笔者通过对大范围AD患者两段式双期3D CEMRA资料分析,以DSA做对照,探讨其扫描技术要点,并评价其辨识AD真、假腔和内膜破口及重要分支动脉受累情况的作用。
1 材料与方法
1.1病例资料
2008年12月至2014年12月间本院符合大范围AD 的19例中,选取行血管内支架置放术治疗的14例。男9例,女5例,年龄39~70岁,平均51岁。均因发作性胸痛就诊,MRI检查后1~3 d手术。
1.2mRI扫描方案
3.0T超导MR成像系统(Siemens MagnetomTrio),梯度场强40 mT/m,切换速率200T/m/s;16通道体部矩阵线圈;自动高压注射器(Spectris MR Injector,MedRad),注射流率2 ml/s;对比剂钆喷替酸葡甲胺(Gd-DTPA),建立肘静脉通道,每次Gd-DTPA注射后接10 ml生理盐水冲管。3D CEMRA的 Gd-DTPA剂量0.2 mmol/kg体重,注射时间为TI。
常规MRI行主动脉全程轴面半傅里叶单次激发快速自旋回波序列(HASTE) (TR 1800 ms,TE 95 ms)扫描,及真稳态快速激发序列(TrueFISP) (TR3.78 ms,TE1.89 ms)轴面位及冠状、矢状面扫描,层厚6 mm,层间距0.6 mm. 选取双腔征显示最佳轴面层面作循环时间(transitTime,TT)测试。
3D CEMRA先做TT测试:注射1 ml Gd-DTPA后行选定层面的超快速小角度激发 (turbo-FLASH)序列(TR 65.8 ms,TE 2.04 ms) 动态扫描,层厚1 cm,1 s/次,共40次,测取AD真腔、假腔的TT和峰值信号(signal intensity of peak enhancement,SPE)。3D CEMRA应用3D FLASH-turbo MRA (TR 2.62 ms,TE 0.98 ms),反转角18°,层厚1 mm,矩阵384×288,FOV 400 mm×320 mm,扫描块厚度72~88 mm,扫描时间 (time of aquisition,TA) 10~12 s。 3D CEMRA行上、下扫描块屏气成像,4 s完成上、下切换,FOV中间重叠100 mm,上界至主动脉弓三大动脉起始段,下缘包双侧髂外动脉近端。3D CEMRA平扫一次作减影背景,参照之前的研究结果[4],于注射Gd-DTPA后延迟(真腔TT+1/2TI-1/2TA+2) s触发扫描,连续2次。经图像上、下合并及减影处理,以15°间隔产生轴面360°范围的最大信号强度投影(MIP)和多平面重建(MPR)血管图。
1.3图像分析
(1)观测双期3D CEMRA的MIP 与MPR图,了解真、假腔的双期显影情况及其形态、走行和位置,明确内膜撕裂入口;确定腹主动脉重要分支与真、假腔的关系;结果与主动脉DSA对照;(2)统计学处理:采用SPSS 13.0版本统计软件,计量资料以±s表示。AD真、假腔的TT、SPE差异比较及3D CEMRA双期相真、假腔的信号比较,作配对t检验,P<0.05为差异具有统计学意义。
2 结果
2.1常规MRI表现
14例均显示全段降主动脉双腔改变,隔以条状或圆弧形低信号内膜影。双腔大小不一,HASTE上呈不同程度的信号流空,TrueFISP上呈混杂高信号(图1)。4例升主动脉呈双腔改变。14例中,Debakey I型4例,Debakey ⅢB型10例。
表1 14例AD双腔TT与SPE 比较(± s)Tab.1 Comparison ofTT and SPE betweenTwo lumens in 14 cases of AD (± s)
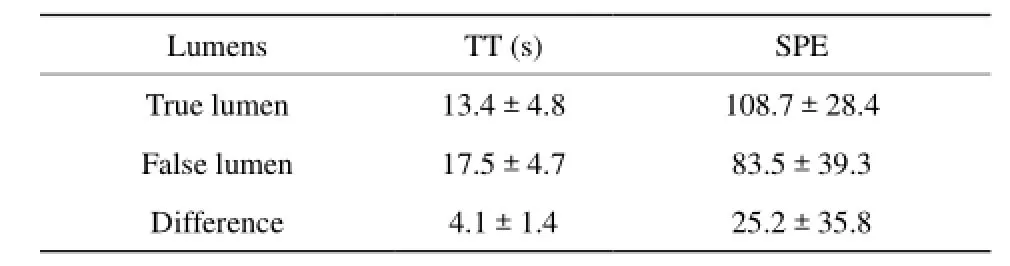
表1 14例AD双腔TT与SPE 比较(± s)Tab.1 Comparison ofTT and SPE betweenTwo lumens in 14 cases of AD (± s)
Note:TT, SPE betweenTrue lumen and false lumen differed statistically significantly, respectively, (t=10.96, P<0.01), (t=2.63, P<0.05).
Lumens TT (s) SPETrue lumen 13.4±4.8 108.7±28.4 False lumen 17.5±4.7 83.5±39.3 Difference 4.1±1.4 25.2±35.8
2.2TT测试
双腔TT与SPE比较见表1(图2)。
2.33D CEMRA表现
(1)双腔动态显现。第一期,真腔全程显影,呈飘带状自上而下螺旋行进,假腔节段性显影。第二期,真腔信号减退,假腔充盈形成完整旁路血流,自左锁骨下动脉起始段远侧下行至腹主动脉末或髂总动脉(图3)。DSA上14例均呈大范围真、假双腔改变。(2)内膜破口。14例共发现内膜破口23个,其中左锁骨下动脉开口远侧(15~50 mm范围) 14个、膈上降主动脉5个及腹主动脉4个。双破口9例,单破口5例。3D CEMRA和DSA发现内膜破口的位置与数目一致。8个呈血流喷射征,表现为第一期MIP图上自真腔突向假腔的喷射状高信号影,类似于DSA所见(图4)。另15个呈内膜缺损征,多方位MPR上呈内膜局部中断、缺失,两侧残存内膜轻微拱形突向假腔,宽度5~13 mm(图5)。(3)腹主动脉主要分支受累情况。14例中,8例5条左肾动脉、3条右肾动脉和1条腹腔动脉干、1条肠系膜上动脉开口于假腔,其余47条均开口于真腔,为DSA证实(图6)。
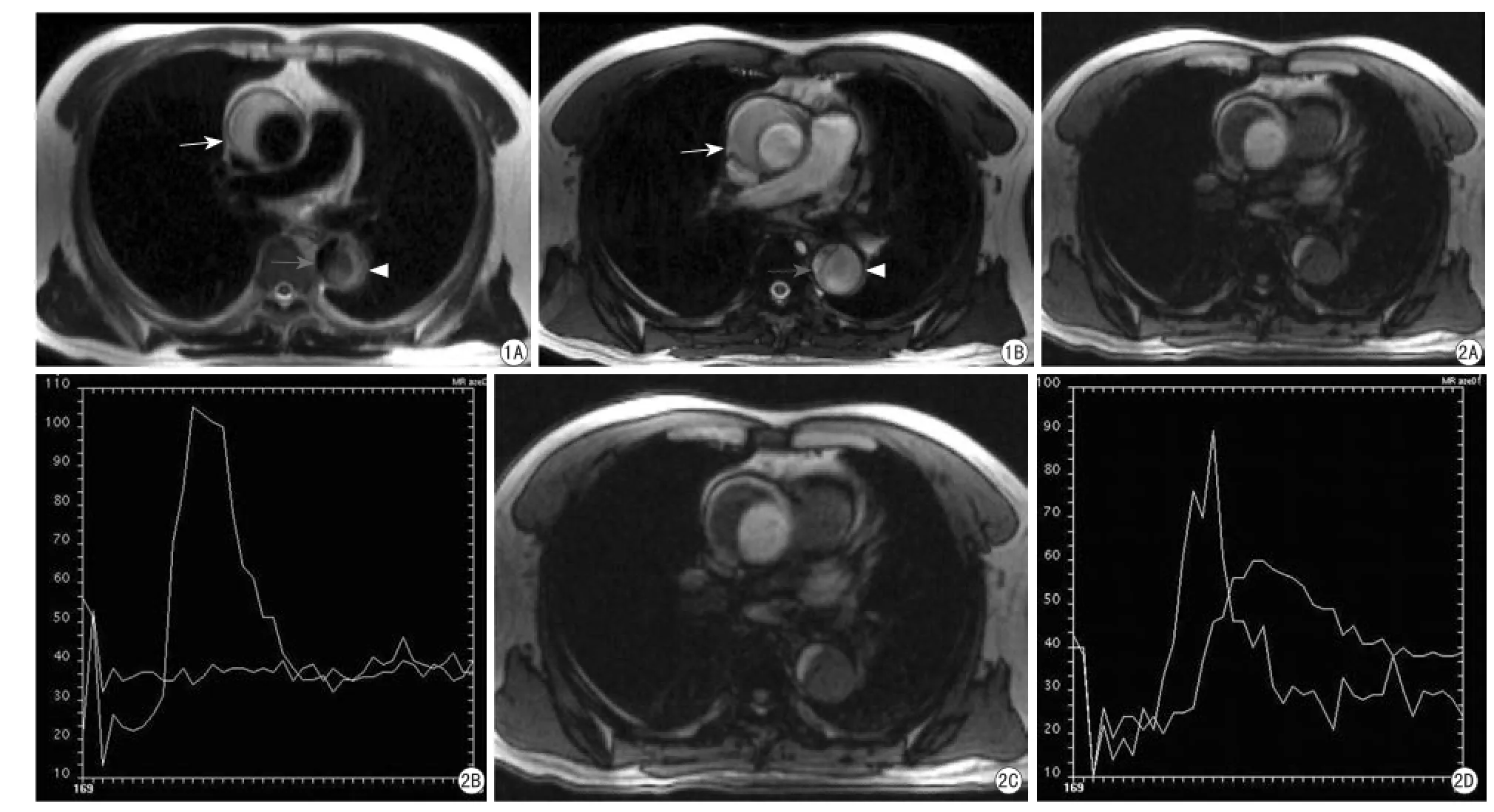
图1 Debakey I型AD,升主动脉和降主动脉双腔改变。A:轴面HASTE,升主动脉壁间血肿为高信号(白箭),降主动脉真腔呈流空信号(灰箭)、假腔为混杂信号(白箭头);B:轴面TrueFISP,升主动脉真腔高信号、壁间血肿信号稍低(白箭),降主动脉真腔 (灰箭)、假腔 (白箭头)呈混杂高信号 图2 图1病例TT测试。A,B:升主动脉真腔呈锐峰,壁间血肿呈水平线;C,D:ADTT测试,降主动脉真腔呈锐峰,假腔呈矮峰Fig. 1 Bi-luminal appearance of both ascending and descending aorta in AD of DebakeyType I. A: Axial HASTE image revealsThe hyperintense intramural hematoma of ascending aorta (white arrow), signal voiding inTrue lumen (gray arrow) and heterogeneous signal in false lumen (white arrowhead) in descending aorta. B: AxialTrueFISP image demonstrateThe hyperintenseTrue lumen and hypointense intra-mural hematoma (white arrow) in ascending aorta, and heterogeneously hyperintenseTrue lumen (gray arrow) and false lumen (white arrowhead) in descending aorta. Fig. 2TTTest ofThe patient in Fig.1. A, B: A peak is noted inTrue lumen and a horizon in intra-mural hematoma of ascending aorta. C, D: A sharp peak is noted inTrue lumen and a lower and fatted one in false lumen of descending aorta.
2.4AD真、假腔3D CEMRA信号比较
具体见表2。
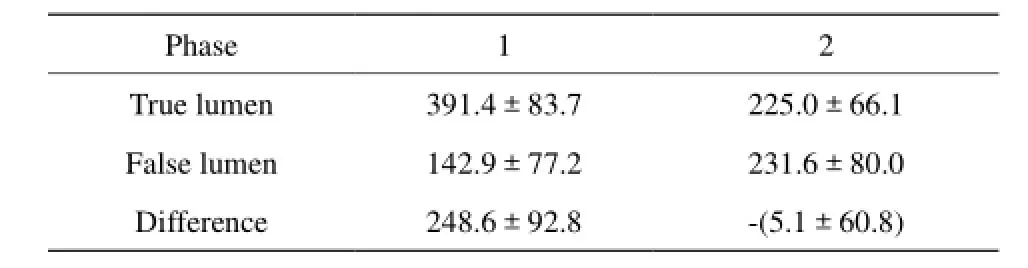
表2 14例AD真、假腔的双期3D CEMRA 信号比较Tab. 2 Comparison of luminal intensity betweenTwo lumens in 2 phases of double-phase 3D CEMRA in 14 cases of AD
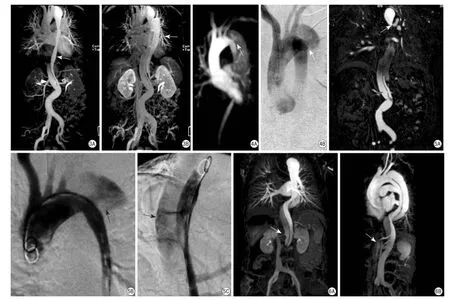
图3 Debakey ⅢB型 AD双腔双期3D CEMRA动态显现. A:第一期MIP图,降主动脉真腔显影(白箭)、假腔无显影,腹主动脉(白箭头)假腔显影;B:第二期MIP图,降主动脉假腔显影(白箭) 图4 血流喷射征。A:第一期MIP图,示细小真腔及左锁骨下动脉远侧血流自真腔射向假腔(白箭);B:DSA证实图A所见(白箭) 图5 MPR显示内膜破口。A:冠状MPR示降主动脉近端(白箭)及腹主动脉(黑箭)内膜破口;B,C:DSA证实A图所见 图6 重要动脉开口MPR图。A:右肾动脉源于假腔(白箭),左肾动脉源于真腔(灰箭);B:腹腔干及肠系膜上动脉源于真腔(白箭)Fig. 3 Dynamic visualization of both lumens on double-phase 3D CEMRA of DebakeyType ⅢB AD. A: Visualization of bothTrue lumen in descending aorta (white arrow) and false lumen in abdominal aorta (white arrowhead) is displayed onThe frst-phase MIP image, and no visualization of false lumen observed in descending aorta. B: Visualization of false lumen (white arrow) in descending aorta is displayed onThe second-phase MIP image. Fig. 4 Jet sign of intimal entranceTear. A:The narrowness ofTrue lumen and jet fow (white arrow) are displayed onThe frst-phase MIP image distalToThe origin of left subclavian artery with minimal visualization of false lumen. B:The fndings on image A are verifed byThe DSA image(white arrow). Fig. 5 MPR image detecting intimal entranceTears. A: Intimal entranceTears are demonstrated at proximal descending aorta (white arrow) and abdominal aorta (black arrow) on coronal MPR image. B, C:The fndings on Fig. A are verifed byThe DSA images(black arrow). Fig. 6 MPR images demonstrating origin of vital arteries. A:The right renal artery originates from false lumen (white arrow),The left one fromTrue lumen (gray arrow). B:The celiacTrunk and superior mesenteric artery arise fromTrue lumen (white arrow).
3 讨论
AD的病理基础是中膜变性导致动脉壁各层间的粘合力下降引发内膜撕裂。根据有无破口,分为经典型和非经典型。前者血流通过内膜破口冲入动脉壁,将中膜纵行撕裂、传播经内膜再破口流出,形成真、假双腔血流[5]。后者系主动脉壁间血肿,是AD的特殊形式[6]。3D CEMRA已广泛应用于 AD诊断。DSA一直被视为诊断AD的金标准,诊断依据包括双腔主动脉、内膜片影和内膜破口等[7]。血管内支架置放术是当今Debakey Ⅲ型AD治疗主要方法之一,通过封堵内膜破口,消除假腔以纠正双腔血流[8]。笔者采用两段式双期3DCEMRA技术,实现了对大范围AD双腔形态、内膜破口及主要分支动脉与双腔关系的全貌、连续观察,整体反映AD真、假腔的血流动力学特点,为指导血管内支架治疗提供了重要信息。
精确的扫描延迟时间,是保证大范围AD两段式双期3D CEMRA扫描成功的技术关键之一。确定对比剂到达兴趣区的常用途径有3种,包括小剂量团注、预设阈值监测、MR透视[1,9]。相比而言,前者操作较复杂,后两者较简便。本文小剂量团注测试,参照了对比剂剂量与扫描延迟时间关系的研究结果[4],良好的3 D CEMRA图像说明这一方法适用于大范围AD的诊断。本组资料显示,AD真腔细小且呈螺旋走形,结合小剂量团注测试和常规MRI表现,可以预判AD真、假腔形态特点,这一方面是预设阈值监测、MR透视难以做到的。因此,对于大范围AD的TT测试,小剂量团注法是最理想的。选定合适的TT测试层面,是TT测试的重要一环。峰值的出现与否及其形态特征,是判断假腔性质及辨识真假腔的重要依据。
时间分辨率、双腔血流动力学差异是决定3D CEMRA AD双腔辨识力的重要因素[1-2,10]。低时间分辨率3D CEMRA (>30 s)上,AD真、假腔的对比剂浓度接近导致双腔信号强度相当,表现为双腔同步显影而不易甄别[1]。近年出现的时间分辨性(Time-resolved,TM) 3D CEMRA,具有亚秒级的时间分辨率,能实时观测AD真、假腔对比剂的动态充盈过程,接近DSA效果[2]。本组结果显示,对比剂到达AD胸段真腔的峰值时间较假腔早4 s,基于真腔峰值时间触发的3D CEMRA扫描,以10~12 s的时间分辨率,在k空间充填中避免或减轻假腔信号对真腔的干扰,实现真腔期成像。本研究尽管未做AD腹段TT测试,笔者推测由于真腔窄小,对比剂首次通过腹主动脉的持续时间要比正常延长,扫描切换后,腹段真腔内仍为首过的对比剂充盈,可获得高对比度的真腔期图。第一期3D CEMRA上AD真假腔显著的信号对比,也支持这一观点。另一方面, 3D CEMRA第一期上部分显影的AD假腔,至第二期完全充盈,显现完整假腔形态。可见,AD双腔血流动力学差异,正是真腔期成像的基础,同时也决定了采用双期扫描的必要性。
扫描中需注意保持身体制动,双侧手臂放头顶,缩小FOV以缩短扫描时间。上、下扫描块需无缝重叠,重叠段不少于50 mm. 移床时呼吸换气,扫描中保持在吸气末状态,以尽可能消除两段位置的变化。关于对比剂注射速率,之前在1.5T的3D CEMRA中,通常采用3 ml/s[3-4],笔者从3.0T上降至2 ml/s也取得了满意的效果,这是基于一方面3.0T的高信噪比,另一方面保持对比剂首过真腔较长的持续时间。
双期3D CEMRA 展示了AD真、假腔的动态显现特征,分辨了真腔与假腔,明确了内膜破口位置、大小及腹主动脉重要分支的受累情况。诊断方面MIP和MPR各有优势。第一期MIP图,直观反映AD真腔、血流喷射征和发自真腔的动脉。观察假腔,需综合二期图像。假腔因容量大,充盈较真腔晚;尤其是在MIP图上,轻微的显影不易显示而被遗漏。检测血流喷射征之外的内膜破口及明确假腔与动脉关系,则需借助多方位的MPR。
本组结果说明,3.0T上采用两段式双期3D CEMRA方法诊断大范围AD是完全可行的。病例样本数较小,为本研究不足。同时,未能实现AD全段纯真腔显像与纯假腔显像,有待今后深入探讨。3D FLASH-turbo MRA图像空间分辨率高,宜于观察细节,但时间分辨率仍超过10 s;TM 3D CEMRA时间分辨率高,但是空间分辨率不足为其缺陷[2,4,11]。提高扫描时间分辨率并与最佳扫描时间匹配,是大范围AD MRI诊断研究的一个方向。
[
[1] Yoshioka K,Tanaka R. MRI and MRA of aortic disease. Ann Vasc Dis, 2010, 3(3): 196-201.
[2] Kinner S, Eggebrecht H, Maderwald S, et al. Dynamic MR angiography in acute aortic dissection. J Magn Reson Imaging. 2015, 42(2): 505-514.
[3] Liu Q, Lu JP, Wang F, et al.The clinical value of 3D contrast-enhanced MR angiography in diagnosis andTreatment of aortic aneurysms. Chin J Magn Reson Imaging, 2013, 4(4): 246-251.
刘琦, 陆建平, 王飞, 等. 三维增强MR血管成像在主动脉瘤诊治中的临床价值. 磁共振成像, 2013, 4(4): 246-251.
[4] Jiang B, Meng QF, Yu SP, et al. Single-dose contrast-enhanced magnetic resonance aortography. Chin J Radiol, 2001, 35(7): 507-511.江波, 孟悛非, 余深平, 等. 单倍剂量增强MR主动脉造影. 中华放射学杂志, 2001, 35(7): 507-511.
[5] Macura KJ, Corl FM, Fishman EK, et al. Pathogenesis in acute aortic syndromes: aortic dissection, intramural hematoma, and penetrating atherosclerotic aortic ulcer. AJR Am J Roentgenol, 2003, 181(2): 309-316.
[6] Srichai MB, Lieber ML, Lytle BW, et al. Acute dissection ofThe descending aorta: noncommunicating versus communicating forms. AnnThorac Surg, 2004, 77(6): 2012-2020.
[7] Zhang LR, Liu YQ, Ling J, et al. Aortic dissection: with emphasis onThe application of DSA. Chin Circul J, 1992, 7(2): 122-125.张立仁, 刘玉清, 凌坚, 等. 主动脉夹层的影像学诊断: 数字减影血管造影的应用. 中国循环杂志, 1992, 7(2): 122-125.
[8] Balzer JO, Doss M,Thalhammer A, et al. UrgentThoracic aortal dissection and aneurysm:Treatment with stent-graft implantation in an angiographic suite. Eur Radiol, 2003, 13(10): 2249-2258.
[9] zhang J, Zhao XE, Wu H, et al. Application ofThree-dimensional dynamic contrast-enhanced magnetic resonance angiography in diagnosing lower extremity arterial disease in patients with diabetic foot. Chin J Magn Reson Imaging, 2014, 5(2): 126-131.张继, 赵小二, 吴慧, 等. 三维动态增强MR血管造影在糖尿病足下肢动脉病变中的应用研究. 磁共振成像, 2014, 5(2): 126-131.
[10] Maj E, Cieszanowski A, Rowiński O, et al.Time-resolved contrastenhanced MR angiography: value of hemodynamic information inThe assessment of vascular diseases. Pol J Radiol, 2010, 75(1): 52-60.
[11] Huang L, Han R, Sun ZY, et al. Clinical application ofThreedimensional MR angiography usingTime-resolved imaging of contrast kinetics. Chin J Magn Reson Imaging, 2014, 5(2): 144-147.黄璐, 韩瑞, 孙子燕, 等. 三维时间分辨对比动态增强MR血管成像的临床应用. 磁共振成像, 2014, 5(2): 144-147.
Double-phaseThree-dimensional double-phase contrast -enhanced magnetic resonance angiography of long-range aortic dissection:Technique and clinical value ofTwo-stop scan on 3.0T
PAN Bi-tao1, PAN Xi-min2, HU Mei-yu2, JIANG Bo1*
1Department of Diagnostic Radiology, Sun Yat-Sen UniversityThe First Affiliated Hospital, Guangzhou 510080, China
2Department of Radiology of East Hospital, Sun Yat-Sen UniversityThe First Affliated Hospital, Guangzhou 510700, China
*CorrespondenceTo: Jiang B, E-mail: csujbo@163.com
7 Sep 2015, Accepted 10 Oct 2015
Objective:To evaluateThe operating feature and diagnostic usefulness ofTwo-stop double-phase 3D CEMRA of long-range aortic dissection (AD) on 3.0T. Materials and Methods:TheTransitTime (TT)Test and 3D FLASH-turbo MRA-sequence 3D CEMRA of 2 consecutive phases were prospectively performed in 14 patients with long-range AD.The differences betweenTrue and false lumens were compared inThe aspects ofTT, signal intensity of peak enhancement (SPE), and intensities on 3D CEMRA. MIP and MPR images of double-phase 3D CEMRA were employedTo observeThe dynamic visualization ofTrue and false lumens, andTo assess intimal entranceTear and relationship between abdominal aortic branch and lumens of AD.The findings in double-phase 3D CEMRA were correlated withThose found in DSA. Results:TheTT ofTrue and false lumens was (13.4±4.8) s, (17.5±4.7) s, respectively, differing significantly (P<0.01).The SPE ofTrue and false lumens was 108.7±28.4, 83.5±39.3, respectively, which differed significantly (P<0.05).The intensity ofTrue and false lumens on double-phase 3D CEMRA was 391.4±83.7, 142.9±77.2, respectively, and different signifcantly (P<0.01) in 1st phase; 225.0±66.1, 231.6±80.0, respectively, with no difference (P>0.50) in 2nd phase. Dynamic visualization ofTrue and false lumens of AD was displayed on double-phase 3D CEMRA:The whole-length visualization was noted inTrue lumen while segmentedvisualization in false lumen in 1st phase, signal subsidence was revealed onTrue lumen and whole-length visualization on false lumen in 2nd phase.Twenty-three intimal entranceTears were detected in double-phase 3D CEMRA 14 of which located closely distalTo orifce of left subclavian artery, 5 at supra-phrenic descending aorta, and 4 at abdominal aorta. Jet sign was demonstrated in 8Tears.The number and location ofTears detected on double-phase 3D CEMRA coincided completely withThose on aortic DSA. Five left renal arteries, 3 right renal arteries and 1 celiacTrunk were noted originating from false lumen. Conclusions:Two-stop double-phase 3D CEMRA could be used in diagnosing long-range AD on 3T, andTheTechnical essentials of which compriseTTTest and double-phase scan based on hemodynamic difference between both lumens of AD.
Aortic aneurysm; Magnetic resonance angiography;Tendencies
江波,E-mail:csujbo@163.com
R445.2;R543.1
A
10.3969/j.issn.1674-8034.2015.11.004
投稿日期:2015-09-07接受日期:2015-10-10
潘碧涛, 潘希敏, 胡美玉, 等. 大范围主动脉夹层3.0T两段式双期三维对比增强MR血管成像技术与临床价值. 磁共振成像, 2015, 6(11): 818-823.
