脑血管反应性与尤瑞克林治疗急性脑梗死预后的相关性:随机单盲对照研究
2015-09-14翟明明黄丽娜闫俊强邵艳敏
翟明明,黄丽娜,闫俊强,邵艳敏
脑血管反应性与尤瑞克林治疗急性脑梗死预后的相关性:随机单盲对照研究
翟明明,黄丽娜,闫俊强,邵艳敏
目的探讨脑血管反应性与尤瑞克林治疗急性脑梗死预后的相关性。方法采用随机、单盲、对照试验,选择河南科技大学第一附属医院神经内科2011年12月—2014年5月收治的194例右侧大脑中动脉供血区急性脑梗死患者,利用经颅多普勒超声(TCD)结合屏气试验检测梗死同侧大脑中动脉(MCA)的屏气指数(HBI),治疗组(89例)给予常规治疗+尤瑞克林治疗15 d,对照组(105例)给予常规治疗15 d。治疗前和治疗第16天,评估记录两组患者的美国国立卫生研究院脑卒中量表(NIHSS)评分和改良残疾程度量表(mRS)评分,分析HBI与NIHSS评分及mRS评分降幅的相关性。结果与治疗前比较,治疗第16天对照组和治疗组NIHSS评分与mRS评分均下降,差异有统计学意义(P<0.05);治疗第16天时,对照组和治疗组NIHSS评分、mRS评分比较,差异均有统计学意义(P<0.05)。相关性分析显示,治疗第16天时,治疗组HBI与NIHSS评分降幅、mRS评分降幅均呈正相关(r=0.427、0.620,P<0.001)。治疗第16天时,对照组HBI与NIHSS评分降幅呈正相关(r=0.618,P<0.001);对照组HBI与mRS评分降幅无直线相关性(r=0.191,P>0.05)。结论对于急性脑梗死患者,TCD评价下的脑血管反应性与尤瑞克林治疗急性脑梗死的短期预后呈正相关。
脑梗死;脑血管循环;尤瑞克林;预后;相关性
翟明明,黄丽娜,闫俊强,等.脑血管反应性与尤瑞克林治疗急性脑梗死预后的相关性:随机单盲对照研究[J].中国全科医学,2015,18(32):3910-3913.[www.chinagp.net]
Zhai MM,Huang LN,Yan JQ,et al.Correlation between cerebrovascular reactivity and the prognosis of patients with acute cerebral infarction treated by urinarykallid:a randomized,single-blind and control study[J].Chinese General Practice,2015,18(32):3910-3913.
脑血流储备受损是脑梗死的独立危险因素[1],可利用经颅多普勒超声(TCD)结合屏气试验检测血管反应性而评价脑动脉功能状态及定量检测脑血流储备[2-3];尤瑞克林虽有改善脑血流储备的潜在价值,但脑梗死患者脑血流储备不同意味着病理生理特点和状态不同,可能对尤瑞克林的治疗效果产生不同的影响。本研究就脑梗死患者脑血流储备与尤瑞克林治疗效果之间的关系进行探讨。
1 资料与方法
1.1临床资料选择河南科技大学第一附属医院神经内科2011年12月—2014年5月收治的194例右侧大脑中动脉供血区急性脑梗死患者,结合病史和临床表现,经颅脑CT检查排除脑出血,经颅脑磁共振弥散加权成像明确诊断。
病例排除标准:(1)合并右侧大脑中动脉供血区以外其他部位急性脑梗死者;(2)合并其他神经系统疾病者;(3)因神经系统疾病有后遗症者;(4)不能配合屏气试验者;(5)有尤瑞克林应用禁忌证者;(6)行溶栓治疗或血管内介入治疗者。
随机分组:采用随机、单盲、对照设计。患者均签署知情同意书,由1名神经内科专家负责试验的质量监控,使用与患者一对一的不同编码的密封信封,并被随机分为治疗组(n=89)和对照组(n=105),由另外2名神经内科医师各自独立在单盲状态下进行试验原始数据的收集。
治疗组在常规治疗的同时给予尤瑞克林治疗15 d,对照组给予常规治疗15 d。两组患者基线资料比较,差异均无统计学意义(P>0.05,见表1)。

表1 两组基线资料比较Table 1 Comparison of basic data between the two groups
1.2检测指标
1.2.1神经功能和预后评价分别采用美国国立卫生研究院脑卒中量表(NIHSS)和改良残疾程度量表(mRS)对两组患者治疗前和治疗第16天的神经功能和残疾程度进行评价和对比分析。
1.2.2血管反应性评价
1.2.2.1 TCD采用经颅多普勒超声仪,型号为德国DWL公司生产的Multi dopT2。患者取仰卧位,并在平静状态下涂适量耦合剂于颞窗,手持2 MHz脉冲探头水平置于右侧颞窗,方向指向对侧,稍加压力于探头,在检测深度为40~65 mm时可检测到血流方向朝向探头的右侧大脑中动脉(RMCA)的清晰血流信号,冻结并记录平均血流速度(Vm)。
1.2.2.2屏气试验[4]患者在完成常规TCD检测后,在原条件不变的情况下于自然呼吸末屏气30 s时,再次冻结并记录Vm。计算屏气指数(HBI),HBI=(屏气后Vm-屏气前Vm)/屏气前Vm×100/屏气秒数,HBI>0.69为正常,否则为异常[5]。
1.3治疗方法常规治疗:口服氯吡格雷(75 mg/d)和拜阿司匹林(100 mg/d)二联抗血小板、口服阿托伐他汀钙片强化降脂(40 mg/d)、丹参注射液(20 m l+ 0.9%氯化钠溶液250 m l)及胞磷胆碱注射液(0.75 g +0.9%氯化钠溶液250 m l)静脉滴注,调控血压、血糖及对基础病的治疗。在此基础上,治疗组患者从入院第1天起同时给予尤瑞克林0.15 PNA单位/d+100 ml 0.9%氯化钠溶液,30~40滴/min,静脉滴注,连续15 d。
1.4统计学方法所有试验数据输入SPSS17.0统计软件包进行统计分析,计量数据以(±s)表示,两组间比较采用t检验,组内比较采用配对t检验;计数资料的分析采用χ2检验;相关性分析采用Pearson相关分析。以P<0.05为差异有统计学意义。
2 结果
2.1两组治疗前后NIHSS评分和mRS评分比较与治疗前比较,对照组和治疗组治疗第16天NIHSS评分mRS评分均下降,差异有统计学意义(P<0.05);治疗第16天,对照组和治疗组NIHSS评分、mRS评分比较,差异有统计学意义(P<0.05,见表2)。
表2 两组患者治疗前后NIHSS评分和mRS评分比较±s,分)Table 2Comparison of NIHSS and mRS scores between the two groups before and after treatment
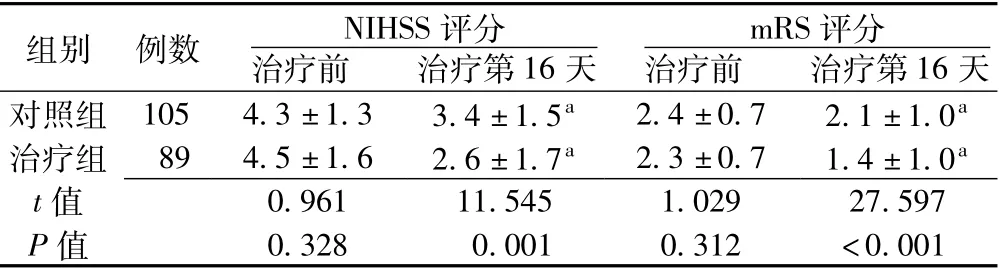
表2 两组患者治疗前后NIHSS评分和mRS评分比较±s,分)Table 2Comparison of NIHSS and mRS scores between the two groups before and after treatment
注:与组内治疗前比较,aP<0.05
组别例数NIHSS评分mRS评分治疗前治疗第16天治疗前治疗第16天对照组1054.3±1.33.4±1.5a2.4±0.72.1±1.0a治疗组894.5±1.62.6±1.7a2.3±0.71.4±1.0at 值0.96111.5451.02927.597 P值0.3280.0010.312<0.001
2.2相关性分析治疗第16天,治疗组HBI与NIHSS评分降幅、mRS评分降幅均呈正相关(r=0.427、0.620,P<0.001,见图1、2)。治疗第16天,对照组HBI与NIHSS评分降幅呈正相关(r=0.618,P<0.001,见图1),对照组HBI与mRS评分降幅无直线相关性(r=0.191,P>0.05)。
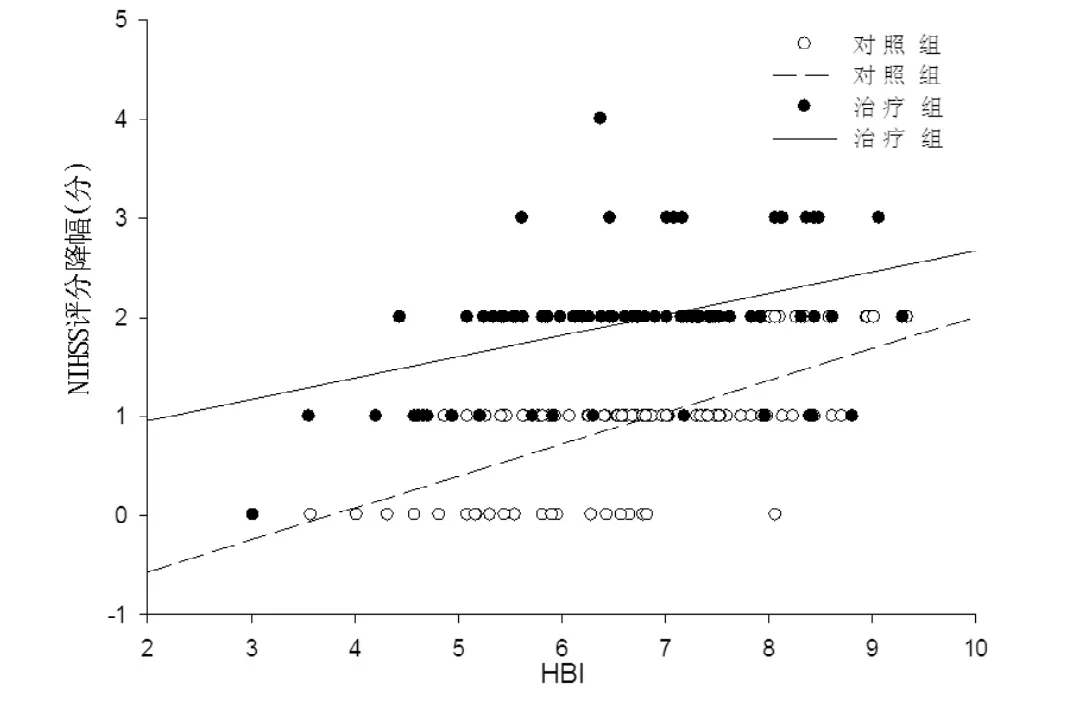
图1 治疗第16天两组HBI与NIHSS评分降幅的相关性Figure 1Correlation between HBI and reduction of NIHSS scores in control group and in treatment group on 16 days during treatment
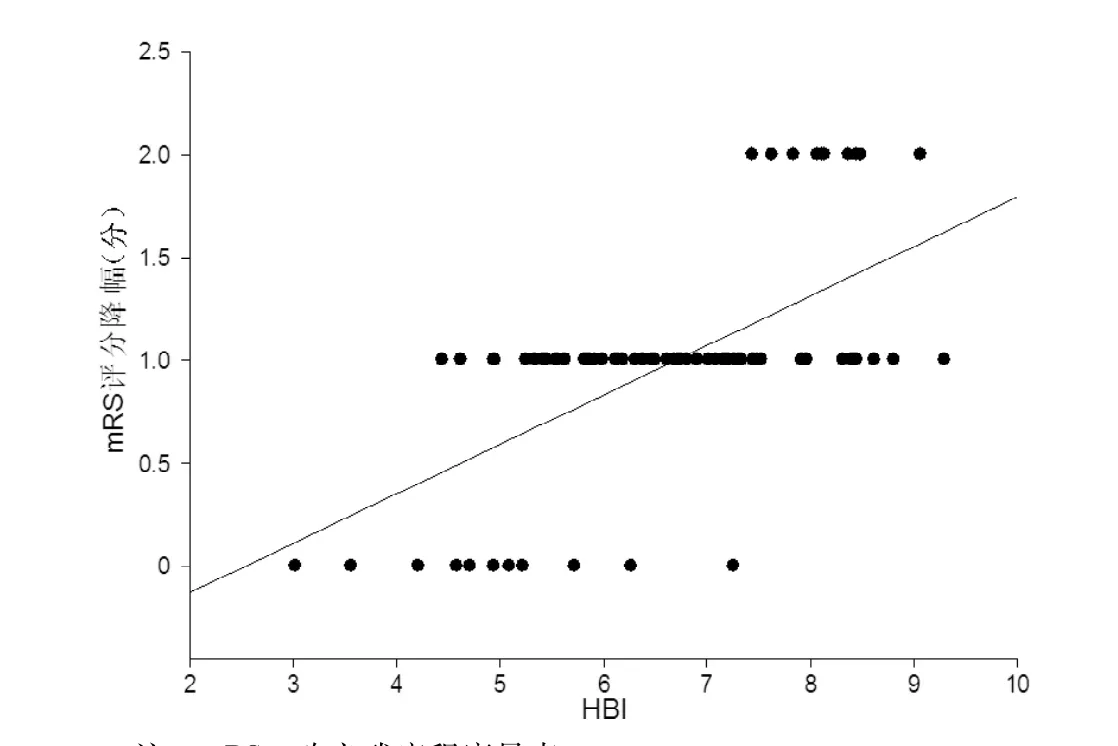
图2 治疗第16天治疗组HBI与mRS评分降幅的相关性Figure 2Correlation between HBI and reduction of mRS scores in treatment group on 16 days during treatment
3 讨论
血管反应性主要用于评价脑血流动力学的改变,间接反映脑血管储备能力。而脑血管储备功能对缺血性卒中预后的判断具有重要价值,脑梗死早期脑血管储备功能损伤与早期神经功能缺损的发生密切相关,脑血管储备功能降低的患者预后较差[6]。鉴于无创、简便和耐受性好等优点,利用TCD结合屏气试验检测脑血管反应性已得到广泛的临床应用[7]。尤瑞克林作为组织型激肽原酶,能使激肽原释放激肽与其相应受体结合激活,触发广泛的生物效应,发挥提高脑血管储备、抑制炎性反应等作用[8-9],对急性脑梗死的治疗具有积极意义。
3.1尤瑞克林有助于改善脑梗死患者预后尤瑞克林可在短时间内通过改善脑梗死缺血区的血流灌注而改善脑梗死患者预后[10],其减轻脑梗死炎性反应、缩小梗死面积、抑制水肿以及抑制核因子(NF)-kB通路并激活MAPK/ERK通路的神经保护作用,也使患者获益[9,11]。本研究显示,经过15 d的治疗,治疗组和对照组NIHSS评分和mRS评分均较治疗前明显下降,且治疗组NIHSS评分和mRS评分均明显低于对照组,神经功能和残疾程度均较对照组明显改善,显示出尤瑞克林治疗脑梗死的有效性,与相关临床研究结果一致[12],进一步证实了尤瑞克林治疗脑梗死安全、有效。
3.2血管反应性影响尤瑞克林的疗效本研究显示,对照组HBI与mRS评分降幅间无直线相关性,对照组NIHSS评分降幅、治疗组NIHSS评分降幅和mRS评分降幅均与患者HBI呈正相关。分析原因如下:一方面,血管反应性本身可能与脑梗死患者的预后呈正相关;另一方面,尤瑞克林对脑梗死的治疗作用也与血管反应性呈正相关,对血管反应性正常的脑梗死患者的治疗作用更显著。尤瑞克林可通过激活内皮细胞上的B1和B2受体促进脑梗死后的血管生成和脑灌注[13],建立侧支循环,为保护脑梗死半暗带和促进神经功能恢复提供了更好的基础条件[14],脑血管储备能力得到提高,短期治疗作用较明显。
3.3血管反应性和尤瑞克林治疗脑梗死的研究展望
对于脑梗死的远期预后,尤瑞克林的治疗价值是潜在的,尽管有结合磁共振功能成像的小样本研究显示尤瑞克林可于脑梗死6个月时改善皮质运动功能的重建[15],但尤瑞克林发挥促进血管、神经修复以及内皮样神经细胞再生等治疗作用时需要较长时间才能显现[16-17],同时也会引起包括肥胖、糖尿病、高血压等可降低血管反应性因素的负面影响[18-20]。为了能更全面、更有效地评估脑梗死病情并更有针对性地制定个体化治疗方案,对于包括有意识障碍的危重患者、后循环脑梗死、脑梗死的不同阶段、不同血管状况的卒中患者,有关血管反应性和尤瑞克林的基础和临床研究需要进一步完善。
本文要点:
(1)血管反应性与尤瑞克林治疗效果呈正相关。
(2)HBI可作为治疗脑梗死选用尤瑞克林的一项依据,从而有助于制定治疗脑梗死的个体化方案以及节约医疗成本和患者的住院经济成本。
[1]Ogasawara K,Ogawa A,Terasaki K,et al.Use of cerebrovascular reactivity in patientswith symptomaticmajor cerebralartery occlusion to predict5-year outcome:comparison of xenon-133 and iodine-123-IMP single-photon emission computed tomography[J].JCereb Blood Flow Metab,2002,22(9):1142-1148.
[2]Vernieri F,Pasqualetti P,Matteis M,et al.Effect of collateral blood flow and cerebral vasomotor reactivity on the outcome of carotid artery occlusion[J].Stroke,2001,32(7):1552-1558.
[3]Lavi S,Gaitini D,Milloul V,et al.Impaired cerebral CO2vasoreactivity:association with endothelial dysfunction[J].Am J Physiol Heart Circ Physiol,2006,291(4):H1856-1861.
[4]Silvestrini M,Vernieri F,Pasqualetti P,et al.Impaired cerebral vasoreactivity and risk of stroke in patients with asymptomatic carotid artery stenosis[J].JAMA,2000,283(16):2122-2127.
[5]SilvestriniM,Vernieri F,Troisi E,et al.Cerebrovascular reactivity in carotid artery occlusion:possible implications for surgical management of selected groups of patients[J].Acta Neurol Scand,1999,99(3):187-191.
[6]Widder B,Kleiser B,Krapf H.Course of cerebrovascular reactivity in patients with carotid artery occlusions[J].Stroke,1994,25 (10):1963-1967.
[7]Pánczél G,Bönöczk P,Nagy Z.Impairment of vasoreactivity in brainstem and hemispheral small vessel disease:comparative study[J].Ideggyogy Sz,2002,55(3/4):95-101.
[8]Gong XP.Mechanism of urinary kallidinogenase in improving the cerebrovascular reserve capacity[J].Chinese Journal of Stroke,2007,2(6):545-548.(in Chinese)龚浠平.尤瑞克林改善脑血管储备能力的研究[J].中国卒中杂志,2007,2(6):545-548.
[9]Chen ZB,Huang DQ,Niu FN,et al.Human urinary kallidinogenase suppresses cerebral inflammation in experimental stroke and downregulatesnuclear factor-kappaB[J].J Cerebral Blood Flow Metab,2010,30(7):1356-1365.
[10]Li J,Chen Y,Zhang X,et al.Human urinary kallidinogenase improves outcome of stroke patients by shorteningmean transit time of perfusion magnetic resonance imaging[J].J Stroke Cerebrovasc Dis,2015,24(8):1730-1737.
[11]Chen ZB,Huang DQ,Niu FN,et al.Human urinary kallidinogenase suppresses cerebral inflammation in experimental stroke and downregulates nuclear factor-kappaB[J].J Cereb Blood Flow Metab,2010,30(7):1356-1365.
[12]Zhang C,Tao W,Liu M,et al.Efficacy and safety of human urinary kallidinogenase injection for acute ischemic stroke:a systematic review[J].J Evid Based Med,2012,5(1):31-39.
[13]Han L,Li J,Chen Y,et al.Human urinary kallidinogenase promotes angiogenesis and cerebral perfusion in experimental stroke[J].PLoS One,2015,10(7):e0134543.doi:10.1371/ journal.pone.0134543.
[14]Lima FO,Furie KL,Silva GS,etal.The pattern of leptomeningeal collaterals on CT angiography is a strong predictor of long-term functional outcome in stroke patients with large vessel intracranial occlusion[J].Stroke,2010,41(10):2316-2322.
[15]Song X,Han L,Liu Y.Remodeling of motor cortex function in acute cerebral infarction patients following human urinary kallidinogenase:a functionalmagnetic resonance imaging evaluation after 6 months[J].Neural Regen Research,2012,7(11):867-873.
[16]Ling L,Hou Q,Xing S,et al.Exogenous kallikrein enhances neurogenesis and angiogenesis in the subventricular zone and the peri-infarction region and improves neurological function after focal cortical infarction in hypertensive rats[J].Brain Res,2008,1206:89-97.doi:10.1016/j.brainres.2008.01.099.
[17]Ding DY,Lyu CZ,Ding MP,et al.A multicenter,randomized,
double-blinded and placebo-controlled study of acute brain infarction treated by human urinary kallidinogenase[J].Chinese Journal of Neruology,2007,40(5):306-310.(in Chinese)
丁德云,吕传真,丁美萍,等.人尿激肽原酶治疗急性脑梗死多中心随机双盲安慰剂对照试验[J].中华神经科杂志,2007,40(5):306-310.
[18]Fülesdi B,Limburg M,Bereczki D,et al.Cerebrovascular reactivity and reserve capacity in type II diabetes mellitus[J].J Diabetes Complications,2000,13(4):191-199.
[19]Rodríguez-Flores M,García-García E,Cano-Nigenda CV,et al.Relationship of obesity and insulin resistance with the cerebrovascular reactivity:a case control study[J].Cardiovasc Diabetol,2014,13(1):2.
[20]Zhao QC,Zhao JH,Zhao Z,et al.Transcranial color-coded duplex sonographic evaluation of cerebrovascular reactivity of type 2 diabetic patients with hypertension[J].Chinese Journal of Ultrasound in Medicine,2008,24(5):406-408.(in Chinese)赵庆春,赵金惠,赵真,等.经颅彩色双功超声评价2型糖尿病合并高血压患者脑血管反应性[J].中国超声医学杂志,2008,24(5):406-408.
(本文编辑:赵跃翠)
Correlation Between Cerebrovascular Reactivity and the Prognosis of PatientsW ith Acute Cerebral Infarction Treated by Urinarykallid:A Random ized,Single-blind and Control Study
ZHAIMing-ming,HUANG Li-na,YAN Jun-qiang,et al.Department of Neurology,the First Affiliated Hospital of He'nan University of Science and Technology,Luoyang 471002,China
Objective To investigate the correlation between cerebrovascular reactivity and the prognosis of patients with acute cerebral infarction treated by urinarykallid.M ethods In this randomized,single-blind and control study,we enrolled 194 patients with acute cerebral infarction in arterial blood supply area of right brain who were admitted into the Department of Neurology of the First Affiliated Hospital of He'nan University of Science and Technology from December 2011 to May 2014.Breath-holding index(HBI)of the middle cerebral artery(MCA)in the brain hemisphere with infarction was measured using transcranial doppler sonography(TCD)and breath-holding test.Treatment group(n=89)was given conventional therapy combined with urinarykallid for 15 days,and control group(n=105)was given conventional treatment for 15 days.Before treatment and 16 days after treatment,we recorded NIHSS and mRS scores of the two groups,and the correlation between HBIand the scoreswas analyzed.Results The two groups had lower(P<0.05)scores of NIHSSandmRS on 16 days after treatment than before treatment;16 days after treatment,the two groupswere significantly different(P<0.05) in the scores of NIHSS and mRS scores.The correlation analysis showed that,on 16 days during treatment,HBIwas positively correlated with reduction of NIHSS and mRS scores in treatment group(r=0.427,0.620,P<0.001);on 16 days during treatment,HBIwas positively correlated with reduction of NIHSS scores in control group(r=0.618,P<0.001),and HBI had no linear correlation with reduction ofmRS scores(r=0.191,P>0.05).Conclusion For patients with acute cerebralinfarction,there is positive correlation between the vascular reactivity evaluated by TCD and short-term prognosis of patients treated by urinarykallid.
Brain infarction;Cerebrovascular circulation;Urinarykallid;Prognosis;Correlation
R 743.33
A
10.3969/j.issn.1007-9572.2015.32.004
471002河南省洛阳市,河南科技大学第一附属医院神经内科
翟明明,471002河南省洛阳市,河南科技大学第一附属医院神经内科;E-mail:zmm810824@163.com
2015-03-10;
2015-09-15)
