Observation on therapeutic effect of electroacupuncture plus acupoint-injection for nerve root sciatica
2015-05-18LiKai,XuXin-yin,DingDe-guang
Observation on therapeutic effect of electroacupuncture plus acupoint-injection for nerve root sciatica
Objective: To observe the clinical effects of electroacupuncture (EA) plus acuoint-injection for nerve root sciatica.
Acupuncture Therapy; Electroacupuncture; Hydro-acupuncture; Acupoint-injection; Sciatica
Sciatica is a common clinical symptom, mainly manifested by radiating pain along the innervations of the sciatic nerve, predominantly at the lower back, buttocks, posterior side of the thigh, posterior and lateral side of the leg and lateral side of the dorsum of foot[1]. Clinically, it is divided into the nerve root type and the nerve trunk type. The nerve root type is often caused by lumbar disc herniation, tuberculosis or deformity of lumbar vertebrae, intraspinal tumor and lumbar spinal stenosis, mostly by lumbar disc herniation[2-3]. The long-term and repeated pain seriously influences the patients’ quality of life. Therefore, it is of great significance to explore an effective treatment protocol for this disease. In recent years, sciatica induced by lumbar disc herniation was treated by electroacupuncture in our clinic. Now, the report is given as follows.
1 Clinical Data
1.1 Diagnostic criteria
The diagnosis was confirmed in reference to the diagnostic criteria of sciatica in the Clinical Diagnostic Basis and Criteria for Cure and Improvement of Disease[4]: radiating pain in the innervations of the sciatic nerve, pain aggravated by cough and sneezing in the pathological change of the nerve root, frequent lateral curvature of the spinal column in relieving pain, flexed kneed when lying on the bed; tenderness on the innervations of the sciatic nerve, such as low back (lateral side) spot, hip spot, buttock spot, popliteal spot,fibular spot and ankle spot; and often positive sciatic nerve-involved sign, such as Kerning sign, Laseque sign, Bonnet sign, Neri sign, Sicard sign, etc.; motor and sensory reflection and autonomic nerve dysfunction in varying degrees in the innervations of the sciatic nerve, commonly seen as weakness in dorsiflexion of the toes in the sick limb, hypaesthesia on the lateral side of the leg, disappearance of ankle tendon reflex and decrease of the gluteal muscle tension, etc.
The differential diagnosis of nerve roots sciatica and trunk sciatica was processed in reference to Practical Neurology[5]: in nerve root sciatica, pain aggravated and in radiating nature by cough, sneezing and in holding breath and exertion, most obvious tenderness at the spinous process and transverse protrusion of the lumbar vertebrae; in trunk sciatica, no induced pain in cough, sneezing and in holding breath and exertion, no obvious tenderness at the spinous process and transverse protrusion of the lumbar vertebrae, obvious tenderness at various spots along the pathway of the sciatic nerve, and decreased muscle tension and slight atrophy of the muscle in the innervations of the sciatic nerve.
1.2 Inclusion criteria
In conformity with the diagnostic criteria of nerve root sciatica; aged from 18 to 70 years old; no mental disorder; no severe cardiac, hepatic and renal diseases; able to cooperate with inspection and treatment; willing to participate in this study and stop other relevant therapy during this treatment.
1.3 Exclusion criteria
Not in conformity with the diagnostic criteria or inclusion criteria; sciatica caused by other reasons, such as lumbosacral deformity, tuberculosis of lumbar vertebrae, tumor of spinal column, intraspinal tumor, lumbar spinal stenosis, lumbar spondylolisthesis, ankylosing spondylitis, pelvic outlet stenosis of sciatic nerve, piriformis syndrome; those with compression of cauda equina, mental unconsciousness; those with primary diseases in the cardiovascular, hepatic, renal, digestive and hemopoietic system; those with mental disorder or severe osteoporosis, or infection and hemorrhage; and women in pregnancy or planning pregnancy, or lactation.
1.4 Statistical methods
All data were processed with the SPSS 17.0 software for windows for statistical analysis. The Chi-square test was for the comparison of rate, and the enumeration data were processed by Ridit analysis. A P value <0.05 indicates a statistical significance。
1.5 General data
Totally, 114 cases of the patients were recruited, including 52 males and 62 females, with the age of 35-70 years old, and were divided into two groups by the digital table. There were 57 cases in the treatment group, including 23 males and 34 females, with the duration ranging from 3-46 months. There were 57 cases in the control group, including 29 males and 28 females, with the duration ranging from 2-43 months. The two groups were not significantly different in the gender, age and duration (P > 0.05) and were comparable (Table 1) .

Table 1. Comparison of general data between the two groups
2 Therapeutic Methods
2.1 Treatment group
2.1.1 EA treatment
Acupoints: Jiaji (EX-B 2) points, Zhibian (BL 54) and Huantiao (GB 30) on the affected side.
Operation: The patients with sciatica on unilateral side took a lateral position on the healthy side, with the healthy lower limb straightened underneath, and the sick lower limb flexed above in 90°, and with a pillow underneath the knee joint of the sick limb. The patients with sciatica on the bilateral sides took the prone position, with a pillow underneath the chest. In accordance with results of CT scan or MRI exam, Jiaji (EX-B 2) points of the corresponding pathological segments at the lumbar region were selected. After the acupoint area was disinfected routinely, filiform needles of 0.35 mm in diameter and 75 mm in length were inserted into various acupoints. In puncturing Huantiao (GB 30), the lightening-like radiating sensation was requested to go along the pathway of the patient’s nerve downward. After the needling sensation appeared in various acupoints, the positive and negative electrodes were respectively connected to Jiaji (EX-B 2) points and Huantiao (GB 30) with 1-2 Hz frequency of continuous wave, by the intensity within the patient’s tolerance. The needles were retained for 30 min.
2.1.2 Acupoint-injection
Acupoint: Bilateral Shenshu (BL 23).
Operation: Disposable 5 mL syringe and No.5 needle were used to draw 3 mL physiological saline and 1.5 mg Cobamamide. After the skin of the acupoint area was disinfected routinely and without withdrawal of blood, the needle was inserted and 1.5 mL liquid was injected into each acupoint.
2.2 Control group
2.2.1 Oral medications
Diclofenac Sodium Sustained-release Tablets, 75 mg,
2.2.2 Muscle injection
Disposable 5 mL syringe and No.5 needle were used to draw 3 mL physiological saline and 1.5 mg Cobamamide for muscle injection at the buttocks.
2.3 Treatment course
The treatment group and control group were treated continuously for seven sessions as one course. The therapeutic effects were observed after a course of treatment.
3 Therapeutic Effects
3.1 Outcome measurements
Pain was assessed by visual analogue scale (VAS). In a straight line of 10 cm, with 1 cm interval between the marks, the left starting spot was labeled 0, representing no pain, and the right ending spot was labeled with 10, representing serious pain. The patients were told to mark the appropriate spots on the straight line to present their pain, and then the examiners measured the distance number from the left to the right, i.e. VAS score of pain intensity.
3.2 Criteria of therapeutic effects
The therapeutic effects were evaluated by Nimodipine method. The clinical effects were assessed by the index of therapeutic effect.
Index of therapeutic effect = (VAS score before treatment – VAS score after treatment) ÷ VAS score before treatment × 100%.
Cure: Index of therapeutic effects was ≥90%.
Remarkable effect: Index of therapeutic effect was≥55%, but <90%.
Effect: Index of therapeutic effect was ≥20% but <55%.
Failure: Index of therapeutic effect was less than 20%.
3.3 Therapeutic results
3.3.1 Comparison of clinical effect between the two groups
By statistical management of the total effective rate between the two groups, the difference was not statistically significant (P>0.05). The curative rate was higher in the treatment group than that in the control group, with a significant difference (P<0.05), (Table 2).

Table 2. Comparison of clinical effect between the two groups (case)
3.3.2 Comparison of VAS score between the two groups
Before treatment, there was no statistical difference in VAS score between the two groups (P>0.05). After treatment, VAS scores in the two groups obviously decreased, and with statistical differences in comparison of those before treatment (P<0.05). The VAS score in the treatment group was remarkably lower than that in the control group, with a statistical difference (P<0.05), (Table 3).

Table 3. Comparison of VAS score before and after treatment between the two groups (x ±s, point)
3.3.3 Comparison of recurrence rate between the two groups
On the fourth day after treatment, the follow-up was given to the patients in the two groups except the failed cases. Fifty-two cases were followed up in the treatment group and 48 cases were followed up in the control group. In comparison of recurrent rate between the two groups, the difference was statistically significant (P<0.05), (Table 4).
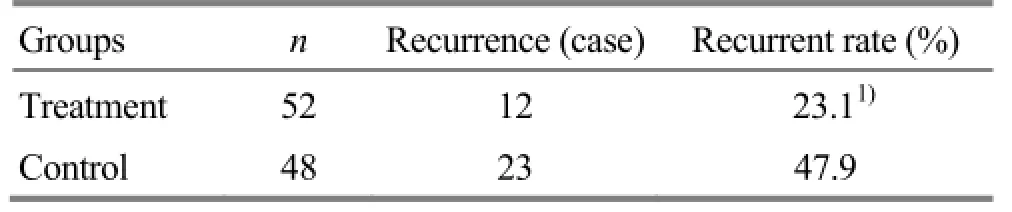
Table 4. Comparison of recurrence rate between the two groups
4 Discussion
There is no term of sciatica in the literature of traditional Chinese medicine (TCM). Sciatica is categorized into the scope of Bi-impediment syndrome and pain of low back and leg in TCM. The pathogenesis of this disease is deficiency in root cause and excess in the symptoms. The kidney dominates the bone, and the liver dominates the tendon. If the liver and kidney are deficient, and the tendon and bone are not nourished, the exogenous pathogens are easy to attack the bodyand influence the circulation of qi and blood. Pain appears when obstruction occurs. Therefore, this disease happens[6-8].
Jiaji (EX-B 2) points are located between the Governor Vessel and the Bladder Meridian of Foot Taiyang. Those two meridians all go through the low back. Huantiao (GB 30) is a crossing acupoint of the Bladder Meridian of Foot Taiyang and Gallbladder Meridian of Foot Shaoyang. More scholars believe that Huantiao (GB 30) is a crossing acupoint of three yang meridians of foot[9-11]. As the saying goes that an acupoint can treat the disorders where its meridian distributes, acupuncture at Jiaji (EX-B 2) points and Huantiao (GB 30) can dredge the meridian qi of the three yang meridians of the lower limb, soothe the tendon and stop pain. The connection of Jiaji (EX-B 2) points and Huantiao (GB 30) of the affected limb by positive and negative electrodes of EA can give a continuous electric stimulation on the sciatic nerve, intensify the needling sensation and enhance the therapeutic effects. Judging from the modern anatomy, the deep part of Huantiao (GB 30) is the main trunk of sciatic nerve. Acupuncture at Huantiao (GB 30) can stimulate the sciatic nerve, so as to improve the motor and sensation of its innervated lower limb. At the same time, EA creates a weak current field in the local area of damaged nerve, so as to improve the electrophysiological characteristics of nerve cells, promote the activity of the nerve cell body enzyme, improve the metabolism of nerve cells, and promote the regeneration and repair of the damaged nerves[12-13].
The therapeutic effect of acupoint-injection is closely related to the selection of acupoints and medications. Shenshu (BL 23) is the Back-Shu point of the kidney, and the low back is a house of the kidney. Shenshu (BL 23) is selected to consolidate the constitution and primary essence, strengthen the tendon and bone, and expel the pathogens[14-16]. Cobamamide has the effects to repair the damaged nerves and stop pain[17].
In summary, EA plus acupoint-injection for sciatica is free of side effect from medication and is an effective therapeutic method.
Conflict of Interest
There was no potential conflict of interest in this article.
Acknowledgments
This work was supported by the Special Fund for Key Special Clinic from State Administration of Traditional Chinese Medicine.
Statement of Informed Consent
All of the patients in the study signed the informed consent.
Received: 16 August 2014/Accepted: 20 September 2014
[1]Zhou GH, Liang GS, Zhong QS. Effect estimate in lumbar hernia of intervertebral discs and sciatica with therapy of electroacupuncture. Guangming Zhongyi, 2009, 24(2): 297-299.
[2]Liguo MH. Warm needling therapy for sciatica: a randomized controlled trial. J Acupunct Tuina Sci, 2011, 9(3): 193-195.
[3] Gao SZ. Acupuncture-moxibustion Science. Beijing: China Press of Traditional Chinese Medicine, 2012: 39.
[4]Sun CX. Clinical Diagnostic Basis and Criteria for Cure and Improvement of Disease. 2nd Edition. Beijing: People’s Military Medicine Press, 1999: 230, 233.
[5]Shi YQ. Practical Neurology. 3rd Edition. Shanghai Science and Technology Publishers, 2004: 287-289.
[6]Yuan T, Lu JS, Ma Y. Present application of vine herbs for treating orthopedics. Liaoning Zhongyiyao Daxue Xuebao, 2012, 14(9): 118-120.
[7]Zhao L, Guo Y, Yan LJ, Xiong J, Wang ZX, Wang W. Bibliometric analysis of literature on acupuncture and moxibustion for treatment of sciatica. Liaoning Zhongyi Zazhi, 2011, 38(3): 526-529.
[8]Peng DH. Traditional Chinese medicine syndrome and treatment for sciatica. Yunnan Zhongyi Xueyuan Xuebao, 1997, 20(1): 35-39
[9]Guan H.My opinion on differentiation of Huantiao (GB 30) along the meridian. Jiangsu Zhongyiyao, 2002, 23(5): 31-32.
[10]Gao XQ, Zhao KR. A brief analysis of Huantiao (GB 30). Tianjin Zhongyiyao, 2010, 27(2): 123-124.
[11]Yang FQ, Chen LJ. Talk about the location of Huantiao (GB 30). Shizhen Guoyi Guoyao, 2006, 17(6): 1068-1069.
[12]Sun ZR, Jin SY, Sun YZ, Sun ST. Mechanical study on acupuncture for regeneration and repair of peripheral nerve injury: influence of acupuncture on induced potential of sciatic injury. Zhongguo Zhongyiyao Keji, 1996, 3(2): 10-12.
[13]Tong S, Wang S, Sun ZR, Liu JQ. Influence of acupuncture therapy on motor end plate after sciatic nerve injury in rats. Zhongguo Kangfu Yixue Zazhi, 2007, 22(6): 533-534.
[14]Zhao HY. Clinical observation on electroacupuncture plus cupping method for trunk sciatica. Hebei Zhongyi, 2004, 26(4): 280.
[15]Wang ZL, Leng J, Cui HY. Review on the development of Cobamamide in clinical application. Zhongguo Yaoshi, 2006, 20(2): 122-125.
[16]Xu QL, Liu T. Therapeutic evaluation of the accumulative analgesic effect of electroacupuncture. Shanghai Zhenjiu Zazhi, 2013, 32(4): 289-290.
[17]Shang XJ, hu WG, Yao FX, Shi L, Jiang WJ. Pharmacodynamics and clinical application of Cobamamide. Chin J of Clinical Rational Drug Use, 2013, 6(8B): 80.
Translator: Huang Guo-qi (黄国琪)
电针加穴位注射治疗根性坐骨神经痛的疗效观察
Li Kai (李凯), Xu Xin-yin (许辛寅), Ding De-guang (丁德光)
Hubei Hospital of Traditional Chinese Medicine, Wuhan 430060, China
目的:观察电针加穴位注射治疗根性坐骨神经痛的临床疗效。方法:将 114 例患者随机分为观察组和对照组,每组57例。观察组采用电针加腺苷钴胺穴位注射治疗,对照组采用双氯芬酸钠缓释片口服加腺苷钴胺肌肉注射治疗,治疗 1 个疗程后比较两组之间的临床疗效。结果:观察组总有效率 96.5%,对照组总有效率 91.2%,两者差异无统计学意义(P>0.05);观察组痊愈率 57.9%,对照组为 21.1%,两组痊愈率差异有统计学意义(P<0.05);治疗结束后第 4 天随访,观察组的复发率为 23.1%,对照组为 47.9%,两者具有统计学差异(P<0.05)。结论:电针加穴位注射治疗根性坐骨神经痛的临床效果显著,值得临床推广。
针刺疗法;电针;水针;穴位注射;坐骨神经痛
R246.6
A
Author: Li Kai, master of medicine, attending physician. E-mail: likaipop1000@163.com
Li K, Xu XY, Ding DG. Observation on therapeutic effect of electroacupuncture plus acupoint-injection for nerve root sciatica. J Acupunct Tuina Sci, 2015, 13 (1): 32-35
10.1007/s11726-015-0819-9
Methods: A total of 114 cases were randomly divided into an observation group and a control group, 57 cases in each group. The observation group was given EA plus acupoint-injection therapy with Cobamamide. The control group was given oral administration of Diclofenac Sodium Sustained-release Tablets plus muscular injection of Cobamamide. After one-course treatment, the clinical effects were compared between the two groups.
Results: The total effective rate was 96.5% in the observation group and 91.2% in the control group, without a statistical significance in the difference between the two groups (P>0.05). The curative rate was 57.9% in the observation group and 21.1% in the control group, with a statistical significance in the difference between the two groups (P<0.05). In the follow-up on the fourth day after the treatment, the recurrence rate was 23.1% in the observation group and 47.9% in the control group, with statistical difference between the two groups (P<0.05).
Conclusion: EA plus acupoint-injection therapy for sciatica of nerve roots is remarkable in the clinical effect and needs promotion in clinic.
猜你喜欢
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- 复式针刺补泻对臀大肌挛缩术后髋关节和膝关节屈伸角度的影响
- 电针对脑缺血再灌注模型大鼠血清白介素的影响
- 隔药灸天枢和气海对慢性炎性内脏痛大鼠痛行为和痛情绪的影响
- Clinical observation on warm needling in canicular days for knee osteoarthritis
- Observation on clinical effect of electroacupuncture plus pricking-cupping bloodletting therapy for herpes zoster
- Observation on clinical effect of acupuncture plus Zi Shen Tiao Gan Decoction for perimenopausal insomnia