Observation on clinical effect of electroacupuncture plus pricking-cupping bloodletting therapy for herpes zoster
2015-05-18HuaYu,LiYing,GuoQing等
Observation on clinical effect of electroacupuncture plus pricking-cupping bloodletting therapy for herpes zoster
Objective: To observe the clinical effect of electroacupuncture (EA) plus pricking-cupping bloodletting therapy for herpes zoster.
Herpes Zoster; Acupuncture Therapy; Electroacupuncture; Cupping Therapy; Blood-letting Puncturing and Cupping
Herpes zoster is an acute infectious skin disease caused by varicella zoster virus. Because the virus is neurotropic, virus would move to skin along the nerve fibers after the onset, causing fierce inflammation in the involved nerves and skin. Skin rash is usually characterized by unilateral presence or presence along the nerve segment, composed of clustered blisters and accompanied by pain. Herpes zoster often affects adults and is more commonly seen in spring and autumn. This disease is similar to snake sores in traditional Chinese medicine (TCM). We treated 23 cases with this disease by electroacupuncture (EA) plus pricking-cupping bloodletting therapy, together with 20 cases treated by oral administration of medications for control study. Now, the report is given as follows.
1 Clinical Data
1.1 Diagnostic criteria
The diagnosis was made in reference to the diagnostic criteria of snake sores in the Shanghai Diagnostic and Therapeutic Guidelines of Traditional Chinese Medicine[1]promulgated by Shanghai Municipal Health Bureau. Skin rash was characterized by blisters in size of mung bean, in cluster, tense in the blister wall, in red base, often distributed unilaterally and in belt. In severe cases, skin rash was manifested by bleeding or visible gangrenous damage. If skin rash occurs in the head and face, the pathological condition would be severe. Before appearance of skin rash, pricking pain or burning sensation would often appear first in the skin,accompanied by mild discomfort in the whole body, fever, obviously subjective pain, intolerable severe pain or neuralgia after fadeaway of skin rash.
1.2 Inclusion criteria
In conformity with the above diagnostic criteria; at the age of 28-70; with blisters for 1-7 d, without anti-viral and analgesic treatment; informed consent, able to go on with acupuncture treatment.
1.3 Exclusion criteria
Women in pregnancy or lactation; those in allergic constitution and allergic to various medications; in scar diathesis; those with severe primary diseases in the cardiovascular, hepatic, renal and hemopoietic system; patients with diabetes, malignant tumor, connective tissue disease, hemophilia; patients with bleeding tendency or in poor blood coagulation; those difficult to make a precise assessment on the efficacy and safety of the treatment; and those unable to accept or inappropriate for acupuncture treatment.
1.4 Statistical method
The obtained data were statistically analyzed by SPSS 13.0 version statistical software. The enumeration data were processed by Chi-square test. The measurement data were processed by t-test. A P value < 0.05 indicates a statistical significance.
1.5 General data
From May of 2010 to January of 2014, 43 patients with herpes zoster were selected from the Community Health Service Center, Huajing Township, Xuhui District, Shanghai, and randomly divided into two groups, 23 cases in the treatment group and 20 cases in the control group. In comparisons of gender, age and duration between the two groups, there were no statistical significances (P>0.05), indicating that the two groups were comparable (Table 1).
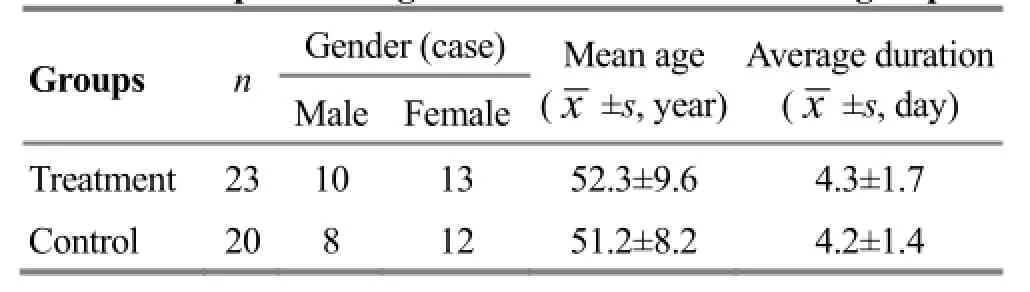
Table 1. Comparison of general data between the two groups
2 Therapeutic Methods
2.1 Treatment group
The patients in the treatment group were given EA plus pricking-cupping bloodletting therapy.
Acupoints: Based upon the positions of the patient’s blisters, Jiaji (EX-B 2) points on the sick side were selected in accordance with the corresponding nerve segments of skin rash, and one segment above and one segment below respectively, and Ashi points.
Operation: The patient took a lateral position, with the sick side above. After routine disinfection, the filiform needles of 0.35 mm in diameter and 40 mm in length were selected. In puncturing Jiaji (EX-B 2), the needles were inserted with an angle of 60-80° between the needle tip and the spine. Ashi points on the skin area surrounding the blisters were punctured circularly around the sick area, in an angle of 15-45° between the needle tip and center of skin rash, about 1-1.5 cun. After the arrival of the needling sensation, Jiaji (EX-B 2) points and Ashi points were manipulated by Tou Tian Liang (Heaven-penetrating Cooling) manipulation (i.e. after the needle was inserted into the deep layer and the arrival of the needling sensation, the needle was thrust lightly and lifted heavily, for six times; then the needle was lifted to the middle layer and thrust lightly and lifted heavily for six times; finally, the needle was lifted to the superficial layer and thrust lightly and lifted heavily for six times, as one process, totally for two processes). Jiaji (EX-B 2) points as one group, and the points in diagonal lines of blister area as one group respectively, totally three groups of the points, were connected to SDZ-II acupuncture apparatus (Huatuo Brand) with a dense-sparse wave, at frequency of 2 Hz/100 Hz, and current intensity of 2-5 mA, within the patient’s tolerance. The treatment was given once per day, for 20 min each session. Ten sessions made one course and totally two courses were given.
After EA treatment, the blister area and surrounding skin were disinfected routinely, and then were tapped with a seven-star needle till slight oozing of blood. Afterward, a cup was quickly attached on the tapped area by a fire-flashing method, to suck out fluid and stagnant blood from local tissue. The cup was retained for 8 min. After the cup was removed, fluid and stagnant blood of the local tissue were wiped off, and then Chlortetracycline eye ointment was applied, in order to prevent infection. The treatment was given once every other day. Five sessions made one course. Totally, two courses were given.
2.2 Control group
The patients in the control group were treated by oral administration of medications, Aciclovir Tablets 800 mg, three times per day; Diclofenac Sodium Dual Release Enteric-coated Capsules 10 mg, once per day; Methylcobalamin Dispersible Tablets 0.5 mg, three times per day; and Vitamin B120.25 mg, three times per day. The local skin of the blisters was kept clean. Ten days made one course. The therapeutic effect was assessed after two courses of treatment.
3 Observation of Therapeutic Effects
3.1 Measurements
Scores of clinical symptoms[2]: Pain, itching and serious burning sensation, accompanied by discomfortin the whole body, restlessness, poor sleep as 4 points; intolerable pain, intermittent sleep affecting work as 3 points; tolerable pain and possible sleep and normal job as 2 points; slight pain or slight itching, not affecting work or rest as 1 point, and no subjective symptoms of pain and itching as 0 point.
Blistering-ending time[3]: Recorded the starting time of the blisters and ending time of the blisters. Blistering-ending time = Ending time of the blistersincreasing - Starting time of the blisters.
Scarring time: Recorded the scarring time of the patient’s skin.
3.2 Criteria of therapeutic effects
The integral-reducing rates of the clinical symptoms were calculated based upon Nimodipine score method.
The integral-reducing rate = (Integral before treatment - Integral after treatment) ÷ Integral before treatment × 100%.
Cure: The integral-reducing rate was 100%.
Remarkable effect: The integral-reducing rate ≥60%,≤99%.
Effect: The integral-reducing rate ≥30%, ≤59%.
Failure: The integral-reducing rate was less than 30%.
3.3 Therapeutic results
3.3.1 Comparisons of the blistering-ending time and scarring time between the two groups
In comparison of the blistering-ending time between the two groups, the difference was statistically significant (P<0.05). In comparison of the scarring time between the two groups, the difference was statistically significant (P<0.01). The blistering-ending time and scarring time were shorter in the treatment group than those in the control group (Table 2).

Table 2. Comparisons of blistering-ending time and scarring time between the two groups (x ±s, day)
3.3.2 Comparison of therapeutic effects between the two groups
The total effective rate was 87.0% in the treatment group and 70.0% in the control group. The difference in the total effective rate was statistically significant between the two groups (P<0.01). The therapeutic effect was better in the treatment group than that in the control group (Table 3).

Table 3. Comparison of clinical effect between the two groups (case)
4 Discussion
It is believed in TCM that this disease is induced by the accumulation of fire in the Liver Meridian or the accumulation of dampness and heat in the Spleen Meridian, plus contraction of pathogenic fire, heat and dampness, so as to induce the liver fire, dampness and heat to attack the muscle and skin and collaterals, leading to blisters. Toxic damp-heat blocking the meridians can cause intense pain. By linking with the meridian qi of Governor Vessel and the Bladder Meridian of Foot Taiyang, like the Back-Shu points, and as the entrance and exit of Zang-fu organs qi, Jiaji (EX-B 2) points respond to Zang-fu organs internally and refill qi to the back externally. As a result, they can reflect the state of Zang-fu organs and are used to treat diseases of Zang-fu organs. It has been proven by the physiological anatomy in the modern medicine that Jiaji (EX-B 2) points are closely related to the nerve segments[4]. Jiaji (EX-B 2) points are located between the Bladder Meridian of Foot Taiyang and Governor Vessel. Acupuncture at Jiaji (EX-B 2) points can regulate qi of the two meridians and regulate yang qi of the whole body, so as to remove the blockage of blood stasis[5]. On one hand, acupuncture at Jiaji (EX-B 2) points in the area of the corresponding nerve segments can stimulate the above structure and surrounding tissues, and can possibly block the pain fiber conduction in the nerves. At the same time, acupuncture can also enhance the pain threshold, and intensify the tolerance of the organism to pain. On the other hand, the propagation of the needling sensation induced by stimulating Jiaji (EX-B 2) points can influence the release of chemical mediators from the sympathetic nerve endings by the neural and humoral regulation[6], so as to produce the analgesic effect.
It has been reported in the literature that EA can regulate and boost the immune functions of the human body, inhibit the inflammatory exudation, and enhance the pain threshold with a better analgesic effect[7]. Surrounding puncture by the filiform needles and tapping by seven-star needle in the painful area aresupposed to clear away heat and dredge the collaterals, and in combination of the Tou Tian Liang (Heaven-penetrating Cooling) needling manipulation, to help to clear away heat, disperse accumulation and expel blood stasis[8-9]. The cupping method after pricking the collaterals can expel the pathogens, dredge the collaterals, stop pain and also can expel blood stasis and promote granulation, beneficial to the healing of skin lesions. This is the important reason to shorten the blistering-ending time time and scarring time. Judging from the modern medical theory, the pricking-cupping bloodletting therapy can quickly reduce the stimulation from pressure of blisters on the surrounding nerves, so as to realize an analgesic effect[10-12].
Generally, it has been proven by this study that the comprehensive application of TCM traditional therapeutic methods of EA stimulation, plus surrounding puncture around the skin rash area and pricking-cupping bloodletting therapy, is mutually complementary, and plays a positive role in improving the clinical symptoms and alleviating pain for greatly shortening the blistering-ending time time and scarring time of herpes zoster and is an effective, convenient and economic therapeutic method.
Conflict of Interest
The authors declared that there was no potential conflict of interest.
Acknowledgments
This work was supported by Community Health Service Center, Huajing Township, Xuhui District, Shanghai.
Statement of Informed Consent
All of the patients in the study signed the informed consent.
Received: 6 August 2014/Accepted: 15 September 2014
[1]Shanghai Municipal Health Bureau. Shanghai Diagnostic and Therapeutic Guidelines of Traditional Chinese Medicine. 2nd Edition. Shanghai: Publishing House of Shanghai University of Traditional Chinese Medicine, 2003: 352-353.
[2]Liu YN, Zhang HX, Huang GF, Zhou Y, Wei W. Observation on therapeutic effect of electroacupuncture at Jiaji (EX-B 2) points plus collateral-pricking and cupping method for herpes zoster. Shanghai Zhenjiu Zazhi, 2009, 28(9): 523-525.
[3]Lu Z, Zheng JY. Treatment of 53 cases of herpes zoster by electroacupuncture plus magic lamp. Henan Zhongyi, 2013, 33(12): 2191-2192.
[4]Cao JR, Li JN, Jia Q, Gao YQ, Shi JH, Song P. Analysis of advantage of electroacupuncture plus acupoint-injection method for postherpetic neuralgia. Huanqiu Zhongyiyao, 2011, 4(4): 289-291.
[5]Zhang SJ, Zhou YH. Acupuncture at Jiaji (EX-B 2) points plus surrounding puncture for postherpetic neuralgia. Zhenjiu Linchuang Zazhi, 2009, 25 (2): 4-6.
[6]Wei L, Yuan GH. Observation on therapeutic effect of acupoint-injection method on Jiaji (EX-B 2) points plus acupuncture treatment for senile postherpetic neuralgia. Zhongguo Zhen Jiu, 2001, 21(6): 333-334.
[7]Fu JL, Dong WY. Treatment of 36 cases of herpes zoster by electroacupuncture plus moxibustion. Zhongguo Zhen Jiu, 2002, 22(5): 314.
[8]Zhu MF, Kuang L, Ouyang H, Yang ZB, Wang C. Clinical observation on 126 cases of postherpetic neuralgia treated by surrounding puncture. Hunan Zhongyiyao Daxue Xuebao, 2006, 26(5): 52-53.
[9]Liu YX, Zhang HX, Huang GF, Zou R, Wei W. Treatment of herpes zoster with electroacupuncture plus collateralpricking and cupping therapy. J Acupunct Tuina Sci, 2013, 11(5): 282-285.
[10]Er ZJ. Observation on clinical effects of collateralpricking and cupping method plus laser radiation for herpes zoster. Jiangxi Zhongyiyao, 2004, (5): 58.
[11]Liu YN, Zhang HX, Huang GF, Zou R, Wei W. Treatment of herpes zoster with electroacupuncture plus collateralpricking and cupping therapy. J Acupunct Tuina Sci, 2013, 11(5): 282-285.
[12]Lu LM. Sequlae neuralgia of herpes zoster treated with bloodletting puncture and cupping and moxibustion. Zhejiang Zhongyiyao Daxue Xuebao, 2010, 34(4): 582-583.
Translator: Huang Guo-qi (黄国琪)
电针联合刺络拔罐治疗带状疱疹疗效观察
Hua Yu (华宇)1, Li Ying (李瑛)1, Guo Qing (郭清)1, Ji Ling-lin (季玲琳)1, Wang Jian-bo (王剑波)2
1 Community Health Service Center, Huajing Township, Xuhui District, Shanghai, Shanghai 200231, China
2 Community Health Service Center of Xietu Neighborhood, Xuhui District, Shanghai, Shanghai 200231, China
目的:观察电针配合刺络拔罐治疗带状疱疹的临床疗效。方法:将43例带状疱疹患者随机分为治疗组23 例和对照组 20 例。治疗组采用电针联合刺络拔罐治疗;对照组采用口服阿昔洛韦片(Aciclovir Tablets)、双氯芬酸钠双释放肠溶胶囊(Diclofenac Sodium Dual Release Enteric-coated Capsules)、甲钴胺分散片(Methylcobalamin Dispersible Tablets)、维生素 B12治疗。结果:治疗组总有效率为 87.0%,对照组为 70.0%,两组总有效率差异有统计学意义(P<0.01)。结论:电针联合刺络拔罐治疗带状疱疹的临床疗效优于药物治疗。
带状疱疹; 针刺疗法; 电针; 拔罐; 刺络拔罐疗法
R246.6
A
Author: Hua Yu, bachelor, attending physician of traditional Chinese medicine
Wang Jian-bo, bachelor, chief physician of traditional Chinese medicine.
E-mail: wangjianbo4013@163.com
Hua Y, Li Y, Guo Q, et al. Observation on clinical effect of electroacupuncture plus pricking-cupping bloodletting therapy for herpes zoster. J Acupunct Tuina Sci, 2015, 13 (1): 54-57
10.1007/s11726-015-0823-0
Methods: A total of 43 patients with herpes zoster were randomly divided into two groups, 23 cases in the treatment group and 20 cases in the control group. The treatment group was given EA plus pricking-cupping bloodletting therapy. The control group was given oral administration of Aciclovir Tablets, Diclofenac Sodium Dual Release Enteric-coated Capsules, Methylcobalamin Dispersible Tablets, and Vitamin B12.
Results: The total effective rate was 87.0% in the treatment group and 70.0% in the control group, with a statistical significance in difference of the total effective rate between the two groups (P<0.01).
Conclusion: The clinical effect is better in the treatment of herpes zoster by EA plus pricking-cupping bloodletting therapy than by medications.
猜你喜欢
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- 复式针刺补泻对臀大肌挛缩术后髋关节和膝关节屈伸角度的影响
- 电针对脑缺血再灌注模型大鼠血清白介素的影响
- 隔药灸天枢和气海对慢性炎性内脏痛大鼠痛行为和痛情绪的影响
- Clinical observation on warm needling in canicular days for knee osteoarthritis
- Observation on clinical effect of acupuncture plus Zi Shen Tiao Gan Decoction for perimenopausal insomnia
- Observation on the efficacy of acupoint massage plus moxibustion for refractory insomnia