退行性腰椎侧凸后路长节段固定不同上端固定椎选择比较的 Meta 分析
2015-05-10章柯杰陈其昕李方才陈刚
章柯杰 陈其昕 李方才 陈刚
后路长节段融合内固定术是目前治疗退行性腰椎侧凸的主要方法,有利于改善退行性腰椎侧凸的矢状位失衡,减轻与改善患者背部疼痛,实现脊柱平衡的重新建立[1-3]。目前,对于长节段后路融合内固定术上端椎的选择仍然存在争议[4]。为此,笔者搜集国内外已发表的关于后路长节段融合不同上端固定椎治疗退行性腰椎侧凸术后疗效的比较文献,对后路长节段融合治疗退行性腰椎侧凸的术后疗效、并发症等进行分析,以期对上端固定椎的选择策略起指导作用。
资料与方法
一、文献检索
计算机检索下列数据库:Cochrane 图书馆( 2014 年第8期 )、PubMed ( 1966 年至 2014 年8月 )、EMbase ( 1966 年至 2014 年8月 )、中国生物医学文献数据库 ( 1978 年至 2014 年8月 )、万方数据库 ( 1998 年至 2014 年8月 )、中国期刊全文数据库( 1999 年至 2014 年8月 )、维普期刊 ( 1998 年至2014 年8月 )。人工检索期刊《The Journal of Bone and Joint Surgery》、《中华骨科杂志》、《中国脊柱脊髓杂志》。英文检索词:degenerative lumbar scoliosis,adult scoliosis,decompression with long fusion,upper instrumented vertebra,DLS,AS,UIV;中文检索词:退行性腰椎侧凸,成人侧凸,长节段融合,上端固定椎。
二、文献纳入与排除标准
1. 纳入标准:(1) 国内外公开发表的比较后路长节段融合不同上端固定椎选择治疗退行性腰椎侧凸的随机对照试验或非随机对照试验;(2) 术前辅助检查提示腰椎侧凸,且侧凸角度>20°;(3) 平均随访时间>12 个月;(4) 患者的性别、年龄、种族、国籍不限。
2. 排除标准:(1) 动物实验;(2) 伴有脊柱骨折、滑脱、结核等;(3) 平均随访时间<12 个月;(4) 特发性侧凸。
三、文献质量评价与资料提取
2 名评价员根据纳入和排除标准,独立筛选文献,如有分歧,通过咨询第三方解决。Deeks 等[5]研究并解释 194 个已发表的非随机对照试验可用于控制偏倚与其它混杂因素,他们认为有6种适合研究的系统评价[6-11]。采用 Jadad 等[12]量表对符合纳入标准的回顾性研究进行方法学质量评价。(1) 患者的随机方法是否正确;(2) 治疗方案执行者、研究对象、研究结果统计和测量者是否采用盲法;(3) 分配方案隐藏是否完善;(4) 有无失访或退出,有失访或退出时是否采用意向治疗分析;(5) 基线是否一致。同时根据 Jadad 评分量表进行评分,满分为5分,≥3 分为高质量研究纳入本次研究,如果出现意见分歧,则通过第三人裁定来解决。
四、结局指标
(1) 术后 Oswestry 功能障碍指数 ( oswestry disability index,ODI );(2) 术后矢状位垂直轴( sagittal vertical axis,SVA );(3) 术后胸椎后凸角 ( thoracic kyphosis,TK );(4) 术后腰椎前凸角 ( lumbar lordosis,LL );(5) 术后交界性后凸角( proximal junctional kyphosis,PJK )。
五、统计学分析
采用 Cochrane 协作网提供的 RevMan5.2 进行Meta 分析。采用χ2检验分析各研究间的异质性,如果各研究间异质性检验差异无统计学意义 (P>0.1,I2<50% ),采用固定效应模型进行 Meta 分析;如果各研究间异质性检验差异有统计学意义 (P<0.1,I2>50% ),则采用随机效应模型进行 Meta 分析。二分类变量采用OR值,以 95%CI表示。
结 果
一、文献检索结果及质量评价
根据检索策略,共检索到相关文献 54 篇。阅读题目和摘要,排除非临床研究、重复发表等不合格文献,进一步阅读全文后排除低质量文献,最终纳入6个对照试验[13-18],共计 453 例。其中融合至上胸椎 ( upper thoracic,UT ) 208 例 ( T10及以上 ),融合至下胸椎 ( lower thoracic,LT ) 245 例 ( T10以下 ),全部为英文文献 ( 表1)。
二、Meta 分析结果
1. 手术时间:4 项研究进行了上胸椎固定与下胸椎固定手术的手术时间比较[13-14,16-17],共纳入335 例,上胸椎固定手术组 149 例,下胸椎固定手术组 186 例。各研究间无统计学异质性 (P=0.36,I2=8% ),采用固定效应模型进行 Meta 分析。上胸椎固定组的手术时间长于下胸椎固定组,差异有统计学意义 [WMD=0.94,95%CI( 0.50,1.38 ),P<0.0001 ] ( 图1)。
2. 术中出血量:4 项研究进行了了上胸椎固定与下胸椎固定手术的术中出血量比较[13-14,16-17],共纳入 335 例,上胸椎固定手术组 149 例,下胸椎固定手术组 186 例。各研究间无统计学异质性 (P=0.48,I2=0% ),采用固定效应模型进行 Meta 分析。上胸椎固定组的术中出血量大于下胸椎固定组,差异有统计学意义 [WMD=0.60,95%CI( 0.34,0.86 ),P<0.00001 ] ( 图2)。
3. 术后 ODI 评分:3 项研究进行了上胸椎固定与下胸椎固定手术的术后 ODI 评分比较[13,16-17],共纳入 170 例,上胸椎固定手术组 68 例,下胸椎固定手术组 102 例。各研究间无统计学异质性 (P=0.49,I2=0% ),采用固定效应模型进行 Meta 分析。上胸椎固定组的术后 ODI 评分与下胸椎固定组比较,差异无统计学意义 [WMD=0.83,95%CI(-3.45,5.10 ),P=0.70 ] ( 图3)。
表1 纳入后路长节段融合内固定不同上端固定椎选择治疗退行性腰椎侧凸相关6篇文献的基本特征 (±s)Tab.1 General characteristics of7 related literatures about posterior long-segment fixation with different upper instrumented vertebrae for degenerative lumbar scoliosis (±s)
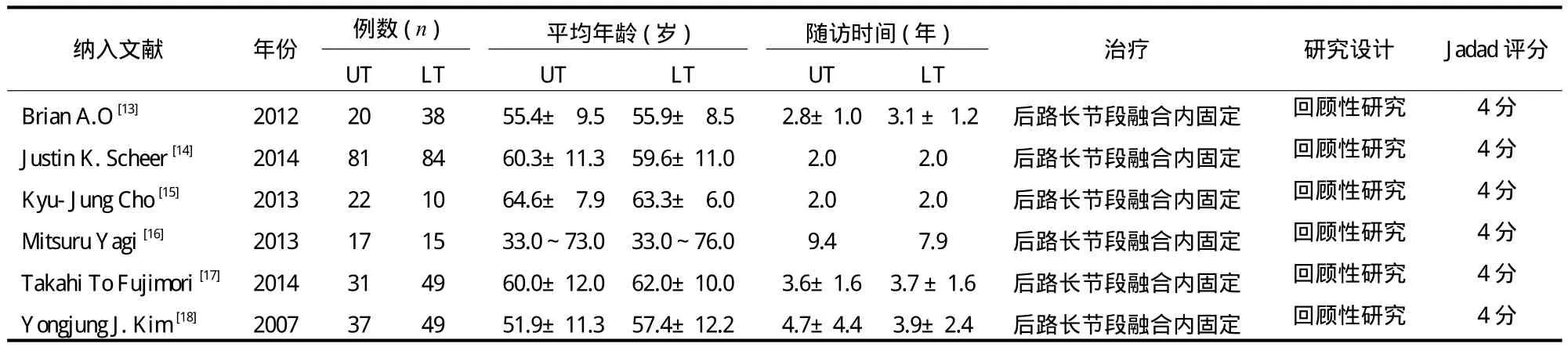
表1 纳入后路长节段融合内固定不同上端固定椎选择治疗退行性腰椎侧凸相关6篇文献的基本特征 (±s)Tab.1 General characteristics of7 related literatures about posterior long-segment fixation with different upper instrumented vertebrae for degenerative lumbar scoliosis (±s)
注:UT:上胸椎;LT:下胸椎Notice: UT: upper thoracic; LT: lower thoracic
纳入文献 年份 例数 ( n ) 平均年龄 ( 岁 ) 随访时间 ( 年 ) 治疗 研究设计 Jadad 评分UT LT UT LT UT LT Brian A.O [13] 2012 20 38 55.4± 9.5 55.9± 8.52.8±1.03.1 ± 1.2 后路长节段融合内固定 回顾性研究4 分Justin K. Scheer [14] 2014 81 84 60.3±11.3 59.6±11.02.02.0 后路长节段融合内固定 回顾性研究4 分Kyu-Jung Cho [15] 2013 22 10 64.6±7.9 63.3±6.02.02.0 后路长节段融合内固定 回顾性研究4 分Mitsuru Yagi [16] 2013 17 15 33.0~73.0 33.0~76.0 9.47.9 后路长节段融合内固定 回顾性研究4 分Takahi To Fujimori [17] 2014 31 49 60.0±12.0 62.0±10.03.6±1.63.7 ±1.6 后路长节段融合内固定 回顾性研究4 分Yongjung J. Kim [18] 2007 37 49 51.9±11.3 57.4±12.24.7±4.43.9±2.4 后路长节段融合内固定 回顾性研究4 分

图1 上胸椎固定组与下胸椎固定组手术治疗退行性腰椎侧凸手术时间比较( 注:采用固定效应模型进行 Meta 分析。上胸椎固定组与下胸椎固定组比较,差异有统计学意义 P <0.0001 )Fig.1 Comparison of the

图2 上胸椎固定组与下胸椎固定组手术治疗退行性腰椎侧凸出血量比较( 注:采用固定效应模型进行 Meta 分析。上胸椎固定组与下胸椎固定组比较,差异有统计学意义 P <0.00001 )Fig.2 Comparison of the operation time after upper thoracic instrumented fusion versus lower thoracic instrumented fusion for degenerative lumbar scoliosis ( Notice:The fixed effect mode1 was employed for this meta-analysis. The comparison between upper thoracic instrumented fusion and lower thoracic instrumented fusion showed statistically significant differences P<0.0001 )intraoperative bleeding amount after upper thoracic instrumented fusion versus lower thoracic instrumented fusion for degenerative lumbar scoliosis( Notice: The fixed effect mode1 was employed for this meta-analysis. The comparison between upper thoracic instrumented fusion and lower thoracic instrumented fusion showed statistically significant differences P<0.00001 )
4. 术后 SVA:4 项研究进行了上胸椎固定与下胸椎固定手术的术后 SVA 比较[14-15,17-18],共纳入363 例,上胸椎固定手术组 171 例,下胸椎固定手术组 192 例。各研究间有统计学异质性 (P<0.0001,I2=87% ),采用随机效应模型进行 Meta分析。上胸椎固定组的术后 SVA 与下胸椎固定组比较,差异无统计学意义 [WMD=-1.13,95%CI(-4.19,1.92 ),P=0.47 ] ( 图4)。
5. 术后 LL:3 项研究进行了上胸椎固定与下胸椎固定手术的术后 LL 比较[15,17-18],共纳入 198例,上胸椎固定手术组 90 例,下胸椎固定手术组108 例。各研究间无统计学异质性 (P=0.15,I2=48% ),采用固定效应模型进行 Meta 分析。上胸椎固定组的术后 LL 与下胸椎固定组比较,差异无统计学意义 [WMD=-0.94,95%CI(-3.39,5.27 ),P=0.67 ] ( 图5)。
6. 术后 TK:4 项研究进行了上胸椎固定与下胸椎固定手术的术后 TK 比较[15,17-18],共纳入 198例,上胸椎固定手术组 90 例,下胸椎固定手术组108 例。各研究间无统计学异质性 (P=0.73,I2=0% ),采用固定效应模型进行 Meta 分析。上胸椎固定组的术后 TK 与下胸椎固定组比较,差异无统计学意义 [WMD=1.51,95%CI(-2.76,55.78 ),P=0.49 ] ( 图6)。
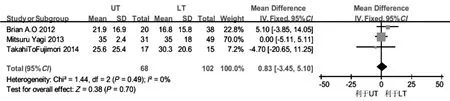
图3 上胸椎固定组与下胸椎固定组手术治疗退行性腰椎侧凸 ODI 评分比较 ( 注:采用固定效应模型进行 Meta 分析。上胸椎固定组与下胸椎固定组比较,差异无统计学意义 P =0.70 )Fig.3 Comparison of the
7. 术后 PJK:3 项研究进行了上胸椎固定与下胸椎固定手术的术后 PJK 比较[15,17-18],共纳入198 例,上胸椎固定手术组 90 例,下胸椎固定手术组 108 例。各研究间无统计学异质性 (P=0.49,I2=0% ),采用固定效应模型进行 Meta 分析。上胸椎固定组的术后 PJK 与下胸椎固定组比较,差异无统计学意义 [WMD=-1.93,95%CI(-4.65,0.79 ),P=0.16 ] ( 图7 )。postoperative ODI scores after upper thoracic instrumented fusion versus lower thoracic instrumented fusion for degenerative lumbar scoliosis( Notice: The fixed effect mode1 was employed for this meta-analysis. The comparison between upper thoracic instrumented fusion and lower thoracic instrumented fusion showed no statistically significant differencesP=0.70 )upper thoracic instrumented fusion versus lower thoracic instrumented fusion for degenerative lumbar scoliosis ( Notice: The random effect model was employed for this meta-analysis. The comparison between upper thoracic instrumented fusion and lower thoracic instrumented fusion showed no statistically significant differencesP=0.47 )

图4 上胸椎固定组与下胸椎固定组手术治疗退行性腰椎侧凸术后 SVA 比较( 注:采用随机效应模型进行 Meta 分析。上胸椎固定组与下胸椎固定组比较,差异无统计学意义 P = 0.47 )Fig.4 Comparison of the postoperative SVA after
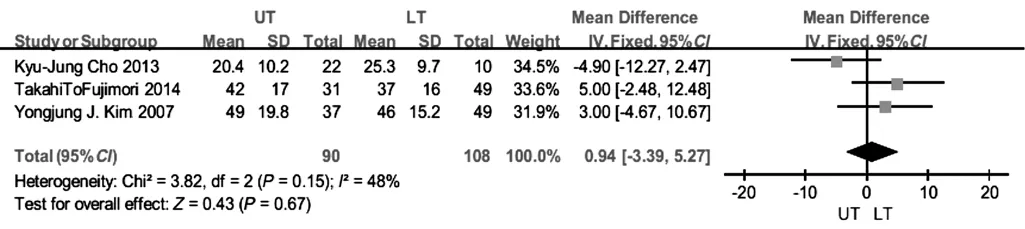
图5 上胸椎固定组与下胸椎固定组手术治疗退行性腰椎侧凸术后 LL 比较( 注:采用固定效应模型进行 Meta 分析。上胸椎固定组与下胸椎固定组比较,差异无统计学意义 P = 0.67 )Fig.5 Comparison of the postoperative LL after upper thoracic instrumented fusion versus lower thoracic instrumented fusion for degenerative lumbar scoliosis ( Notice: The fixed effect mode1 was employed for this meta-analysis. The comparison between upper thoracic instrumented fusion and lower thoracic instrumented fusion showed no statistically significant differences P=0.67 )

图6 上胸椎固定组与下胸椎固定组手术治疗退行性腰椎侧凸术后 TK 比较( 注:采用固定效应模型进行 Meta 分析。上胸椎固定组与下胸椎固定组比较,差异无统计学意义 P = 0.49 )Fig.6 Comparison of the postoperative TK after upper thoracic instrumented fusion versus lower thoracic instrumented fusion for degenerative lumbar scoliosis ( Notice: The fixed effect mode1 was employed for this meta-analysis. The comparison between upper thoracic instrumented fusion and lower thoracic instrumented fusion showed no statistically significant differences P=0.49 )thoracic instrumented fusion versus lower thoracic instrumented fusion for degenerative lumbar scoliosis ( Notice: The fixed effect mode1 was employed for this meta-analysis. The comparison between upper thoracic instrumented fusion and lower thoracic instrumented fusion showed no statistically significant differences P=0.16 )
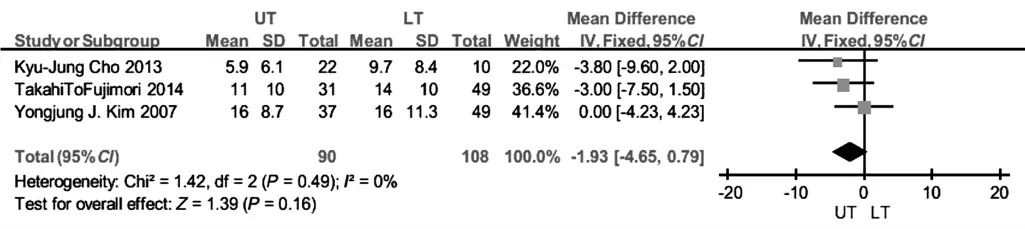
图7 上胸椎固定组与下胸椎固定组手术治疗退行性腰椎侧凸术后 PJK 比较( 注:采用固定效应模型进行 Meta 分析。上胸椎固定组与下胸椎固定组比较,差异无统计学意义 P = 0.16 )Fig.7 Comparison of the postoperative PJK after upper
讨 论
目前,后路长节段融合内固定仍是退行性腰椎侧凸的主要手术治疗方法。手术的目标不仅是缓解患者的疼痛症状,也要减少手术所出现的并发症[19]。本次系统评价共纳入6项临床研究,共计453 例,其中融合至上胸椎 208 例,融合至下胸椎 245 例。本研究结果提示,与融合至上胸椎组相比,融合至下胸椎组的手术融合节段少、手术时间短且手术出血量少。另一方面,两组术后 ODI 评分差异无统计学意义,提示下胸椎固定融合较上胸椎融合更具有优势。
恢复脊柱的矢状面平衡是手术治疗退行性腰椎侧凸的主要目标之一。既往的研究结果显示,退行性腰椎侧凸患者根据其 LL 和 PJK 不同,可分为三种不同类型,手术矫正以恢复这些参数对恢复脊柱的矢状面平衡至关重要[20]。有学者认为可以通过向近端延长固定节段以达到更好的矫形[4,21]。本组 Meta分析发现向近端延长固定椎并未能改善术后 LL 和PJK,对代表脊柱矢状面重要指标的 SVA 也无显著性影响。
近端固定椎相邻节段后凸是退行性腰椎侧凸长节段固定术后常见的并发症,被认为是影响术后疗效的主要原因之一。TK 是判断 PJK 发生的主要指标。一般认为术后近端固定椎相邻节段发生>10° 的渐进性后凸即可界定为 PJK 的发生。由于 PJK 均发生在胸椎,笔者对两种不同近端固定椎的 TK 进行了比较,结果显示两组间差异无统计学意义。此结果也表明了单纯向近端延长固定节段对防止 PJK 的发生并无显著的效果。
本次系统评价目前仍存在以下局限性:(1) 本次纳入均为回顾性研究,无随机对照实验 ( randomized controlled trial,RCT ) 纳入本组分析,因此结果的可靠性需要进一步考量;(2) 纳入文章数量较少,可能影响可靠性;(3) 文章未纳入全部术后疗效指标 ( 如 SRS,术后假关节发生率,术后再次手术等 ),矢状位骨盆测量指标 ( 如骨盆倾斜角、骨盆入射角,腰椎前凸-骨盆入射角等 ) 也未纳入其中,导致数据分析不全面;(4) 各研究随访时间的差异可能在一定程度上影响结果的可靠性。
[1] Chow DH, Luk KD, Evans JH, et al. Effects of short anterior lumbar interbody fusion on biomechanics of neighboring unfused segments. Spine, 1996, 21(5):549-555.
[2] Dekutoski MB, Schendel MJ, Ogilvie JW, et al. Comparison of in vivo and in vitro adjacent segment motion after lumbar fusion. Spine, 1994, 19(15):1745-1751.
[3] Herkowitz HN, Abraham DJ, Albert TJ. Management of degenerative disc disease above an L5-S1 segment requiring arthrodesis. Spine, 1999, 24(12):1268-1270.
[4] Shufflebarger H, Suk SI, Mardjetko S. Debate: determiningthe upper instrumented vertebra in the management of adult degenerative scoliosis: stopping at T10 versus L1. Spine, 2006,31(Suppl 19):S185-194.
[5] Deeks JJ, Dinnes J, D’Amico R, et al. Evaluating nonrandomised intervention studies. Health Technol Assess, 2003,7(27):iii-x,1-173.
[6] Reisch JS, Tyson JE, Mize SG. Aid to the evaluation of therapeutic studies. Pediatrics, 1989, 84(5):815-827.
[7] Thomas H. Quality assessment tool for quantitative studies.Toronto: Effective Public Health Practice Project, 2009:164-168.
[8] Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. [2014-08-31]. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
[9] Zaza S, Wright-De Agüero LK, Briss PA, et al. Data collection instrument and procedure for systematic reviews in the Guide to Community Preventive Services. Task Force on Community Preventive Services. Am J Prev Med, 2000, 18(Suppl 1):44-74.
[10] Cowley DE. Prostheses for primary total hip replacement. A critical appraisal of the literature. Int J Technol Assess Health Care, 1995, 11(4):770-778.
[11] Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health, 1998, 52(6):377-384.
[12] Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary?Control Clin Trials, 1996, 17(1):1-12.
[13] O’Shaughnessy BA, Bridwell KH, Lenke LG, et al. Does a long-fusion “T3-sacrum” portend a worse outcome than a shortfusion “T10-sacrum” in primary surgery for adult scoliosis?Spine, 2012, 37(10):884-890.
[14] Scheer JK, Lafage V, Smith JS, et al. Maintenance of radiographic correction at2years following lumbar pedicle subtraction osteotomy is superior with upper thoracic compared with thoracolumbar junction upper instrumented vertebra. Eur Spine J, 2015, 24(Suppl 1):121-130.
[15] Cho KJ, Suk SI, Park SR, et al. Selection of proximal fusion level for adult degenerative lumbar scoliosis. Eur Spine J, 2013,22(2):394-401.
[16] Yagi M, King AB, Cunningham ME, et al. Long-term clinical and radiographic outcomes of pedicle subtraction osteotomy for fixed sagittal imbalance: does level of proximal fusion affect the outcome? Minimum5-year follow-up. Spine Deformity,2013, 1(2):123-131.
[17] Fujimori T, Inoue S, Le H, et al. Long fusion from sacrum to thoracic spine for adult spinal deformity with sagittal imbalance: upper versus lower thoracic spine as site of upper instrumented vertebra. Neurosurg Focus, 2014, 36(5):E9.
[18] Kim YJ, Bridwell KH, Lenke LG, et al. Is the T9, T11, or L1 the more reliable proximal level after adult lumbar or lumbosacral instrumented fusion to L5 or S1? Spine, 2007, 32(24):2653-2661.
[19] Cho KJ, Kim YT, Shin SH, et al. Surgical treatment of adult degenerative scoliosis. Asian Spine J, 2014, 8(3):371-381.
[20] 李方财, 陈其昕, 陈维善, 等. 腰椎退行性侧凸患者脊柱矢状位参数与骨盆参数的相关性. 中华骨科杂志, 2013, 33(9):928-934.
[21] Kim YJ, Bridwell KH, Lenke LG, et a1. An analysis of sagitgal spinal alignment following long adult lumbar instrumentation and fusion to L5 or Sl: can we predict ideal lumbar lordosis.Spine, 2006, 31(20):2343-2352.