DHS与Intertan治疗老年患者股骨粗隆间Evans Ⅰ型骨折的疗效比较
2015-03-10丁裕润王伟力马涛胡光宇李展春王博
丁裕润 王伟力 马涛 胡光宇 李展春 王博
(上海交通大学医学院附属仁济医院骨科, 上海 200127)
·论著·
DHS与Intertan治疗老年患者股骨粗隆间Evans Ⅰ型骨折的疗效比较
丁裕润王伟力马涛胡光宇李展春王博
(上海交通大学医学院附属仁济医院骨科, 上海200127)
摘要目的:比较闭合复位动力髋螺钉(dynamic hip screw,DHS)与闭合复位股骨近端髓内钉Intertan治疗老年患者股骨粗隆间Evans Ⅰ型骨折的疗效。方法: 手术治疗股骨粗隆间骨折(Evans Ⅰ型)老年患者70例,其中行闭合复位DHS内固定术30例(DHS组),行闭合复位Intertan内固定术40例(Intertan组)。结果:患者均获随访,时间6~24 (12.0±3.0)个月。骨折均愈合,未出现内固定失败、股骨头坏死等并发症。手术时间:DHS组40~90 (63.6±8.4) min,Intertan组40~90 (55.6±9.8) min;术中出血量:DHS组100~200 (145.4±22.5)mL,Intertan组100~200 (92.4±25.5)mL;住院时间:DHS组6~16 (11.2±2.8)d,Intertan组6~9 (7.9±1.1) d;两组手术时间、术中出血量、住院时间比较,差异有统计学意义(P<0.05)。DHS组4例患者术后手术切口液化,换药后愈合。骨折愈合时间:DHS组2.5~4.0 (3.4±0.8)个月,Intertan组2.5~4.0 (3.2±0.7)个月,两组差异无统计学意义(P>0.05)。术后髋关节Harris总评分:DHS组67~84 (73.5±5.1)分,Intertan组70~86 (77.9±3.7)分;功能评分:DHS组23~40 (30.8±3.2)分,Intertan组25~44 (34.4±2.9)分;两组术后髋关节Harris总评分和功能评分比较,差异有统计学意义(P<0.05)。疼痛评分:DHS组为20~44 (34.9±4.8)分,Intertan组为20~44 (35.8±5.0)分;活动范围评分:DHS组2~4 (3.0±0.8)分,Intertan组2~4 (3.0±1.0)分;两组疼痛评分和活动范围评分比较,差异均无统计学意义(P>0.05)。结论:Intertan和DHS内固定都是治疗老年患者股骨粗隆间骨折的有效手段,但前者创伤较小,住院时间较短,髋关节功能恢复更好。
关键词股骨粗隆间骨折;Evans分型;Intertan髓内钉;动力髋螺钉;Harris髋关节功能评分
Efficacy Comparison between DHS and Intertan in the Treatment of Elderly Patients with Evans Type Ⅰ Intertrochanteric FractureDINGYurunWANGWeiliMATaoHUGuangyuLIZhanchunWANGBoDepartmentofOrthopedics,RenjiHospital,ShanghaiJiaoTongUniversitySchoolofMedicine,Shanghai200127,China
AbstractObjective:To compare the clinical efficay between dynamic hip screw (DHS)and proximal femoral nail(Intertan) fixation after closed reduction for the treatment of elderly patients with Evans type Ⅰ intertrochanteric fracture. Methods:Among 70 elderly patients with intertrochanteric fracture (Evans Ⅰ) undergoing surgical treatment, 30 cases (DHS Group) were treated by closed reduction and DHS internal fixation and the other 40 cases (Intertan Group) were treated by closed reduction and Intertan fixation. Results: All the patients were followed up for 6-24 (12.0±3.0) months. All the fractures were healed and no complication such as failure of internal fixation or femoral head necrosis occurred. There was statistically significant difference between operation time the DHS group and the Intertan group with 40-90 (63.6±8.4) min and 40-90 (55.6±9.8) min in DHS Group and Intertan Group, respectively. And the intraoperative blood loss were 100-200 (145.4±22.5) mL and 100-200 (92.4±25.5) mL in DHS Group and Intertan Group, respectively. Furthermore, the duration of stay were 6-16 (11.2±2.8) days and 6-9 (7.9±1.1) days in DHS Group and Intertan Group, respectively. There were significant difference regarding operation time, intraoperative blood loss, and duration of stay between the two groups(P<0.05). Wound healing were achieved by postoperative liquefaction wound care in 4 cases of DHS group. There was no significant difference regarding fracture healing time between the 2.5-4.0 (3.4±0.8) months in DHS Group and the 2.5-4.0 (3.2±0.7) months in Intertan Group(P>0.05). There were statistically significant differences between the two groups regarding Harris function scores after operation, which were 67-84 (73.5±5.1) points in DHS Group and 70-86 (77.9±3.7) points in Intertan Group, and function scores which were 23-40 (30.8±3.2) points in DHS Group and 25-44 (34.4±2.9) points in Intertan Group (P<0.05). There was no significant difference between two groups regarding pain scores, which were 20-44 (34.9±4.8) points in DHS Group and 20-44 (35.8±5.0) points in Intertan Group, and activity range scores, which were 2-4 (3.0±0.8) points in DHS Group and 2-4 (3.0±1.0) points in Intertan Group (P>0.05). Conclusions: The Intertan and DHS internal fixation are effective methods for the treatment of elderly patients with intertrochanteric fractures. Intertan showed less trauma, shorter duration of stay, and better recovery of hip function.
Key WordsIntertrochanteric fracture;Evans type;Intramedullary intertan nail;Dynamic hip screw;Harris function score
股骨粗隆间骨折在四肢骨折中较为常见,是老年人的常见病和多发病。保守治疗股骨粗隆间骨折虽可使骨折愈合,但因老年患者常合并多种内科疾患,加上长期卧床会发生褥疮、肺部感染等并发症,故病死率较高。对于没有手术禁忌的股骨粗隆间骨折患者,一般主张早期手术治疗,以减少并发症[1-2]。但对于Evans Ⅰ型股骨粗隆间骨折,目前临床上尚无统一的手术标准[3-5]。2010年1月—2014年3月我院分别采用动力髋螺钉(dynamic hip screw,DHS)和股骨近端髓内钉Intertan治疗70例老年股骨粗隆间Evans Ⅰ型骨折患者,现比较两种治疗方法的临床效果,并报告如下。
1资料与方法
1.1一般资料选择2010年1月—2014年3月在我院手术治疗的股骨粗隆间Evans Ⅰ型骨折的老年患者70例,其中男性20例,女性50例;年龄70~83(74.2±3.3)岁;均经X线片及CT检查确诊为单侧闭合骨折;Evans Ⅰ型稳定型骨折37例,Ⅰ型不稳定型骨折33例;排除其他疾病引起的髋关节功能障碍。70例中,30例行闭合复位DHS内固定术(DHS组),40例行闭合复位Intertan内固定术(Intertan组)。DHS组中,男性6例,女性24例;年龄70~81 (74.1±3.3)岁;稳定型骨折25例,不稳定型骨折5例;受伤至手术时间1~3(1.6±0.6) d。Intertan组中,男性14例,女性26例;年龄70~83(74.3±3.4)岁;稳定型骨折17例,不稳定型骨折23例;受伤至手术时间1~3 (1.5±0.6) d。两组术前资料比较,差异无统计学意义(P>0.05)。
1.2手术方法采用全身麻醉,患者置于牵引床,在C臂机透视下行闭合复位,复位满意后消毒铺巾。(1)DHS组的手术方法参照文献[6]:取外侧切口,自股骨大粗隆顶点向远端延伸,长10~12 cm;逐层切开皮肤及皮下组织、阔筋膜、肌肉,在C臂机透视下,将加压螺钉的导针打入股骨颈内,测量长度,置入加压螺钉;置入侧方钢板,用皮质骨螺钉固定钢板与股骨干;在C臂X线机透视下确认无误后,关闭切口。 (2)Intertan组的手术方法参照文献[7-8]:在股骨大粗隆顶点处作3~5 cm的直切口。用手指触摸到大转子顶点,进钉点为大转子顶点偏内处;用开孔器在进钉点开孔,穿透皮质,放入球形导针;扩髓后放入相应大小的Intertan主钉,用手连接器将主钉插入髓腔;在C臂机透视下确认主钉位置后,通过侧方组件套筒打入导针,透视下确认导针位置在颈部中央偏下;钻孔后选择合适长度组合钉,先旋入主钉,再旋入加压钉,加压效果满意后,在股骨远端打入锁钉;在C臂机透视下确认无误后,关闭切口。
1.3术后处理术后第2天起开始被动活动髋、膝、踝关节,采用膝关节功能训练机(CPM)辅助锻炼。术后2周左右伤口拆线,加强主动不负重床上及床边活动,加强股四头肌肌力训练。稳定型骨折患者术后4周可以用助步器下床进行不负重活动。不稳定型骨折患者则需要适当延后下床时间,术后8周若X线片示骨折线开始模糊、骨痂生长,可以在助步器辅助下逐渐负重;术后12周骨折愈合后,可以自由负重活动。
1.4观察指标及功能评价观察患者的手术时间、术中出血量、骨折愈合时间、住院时间及并发症情况[9-10]。骨折愈合后半年采用Harris评分评价髋关节功能[11]:疼痛44分,功能51分,髋关节前屈、外展、外旋等活动范围5分,总分100分。

2结果
70例患者均获得随访,随访时间为6~24 (12.0±3.0)个月。
2.1两组手术时间、术中出血量、骨折愈合时间、住院时间的比较见表1。
2.2并发症70例患者的骨折均愈合。DHS组4例患者术后出现伤口液化,经过换药处理后痊愈。两组均无神经、血管损伤,未出现股骨头缺血性坏死和骨折畸形愈合,未见明显的螺钉松动。
2.3两组患者的Harris髋关节功能评分见表2。 典型病例的影像学表现见图1~2。

表1 两组患者手术时间、术中出血量、骨折愈合时间及住院时间的比较 (±s)
表2 两组患者术后Harris髋关节功能评分比较 (分,±s)
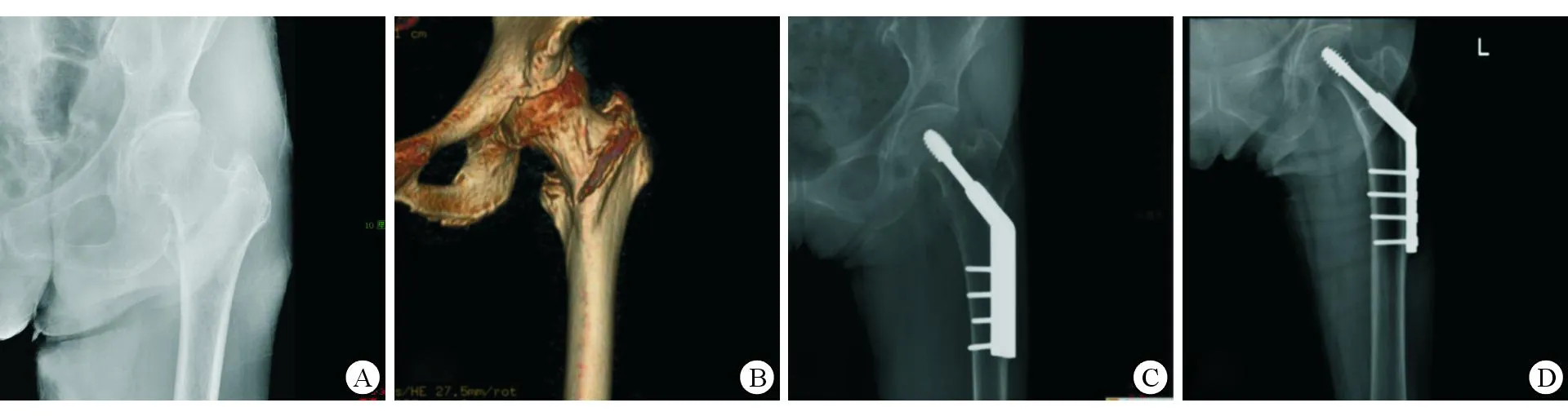
A: 术前X线片示左股骨粗隆间骨折;B: 术前CT三维重建;C: 术后X线片示DHS内固定术后,骨折对位对线好; D: 末次随访X线片,示骨折愈合
图1患者女,81岁,左股骨粗隆间骨折,Evans Ⅰb型,行闭合复位DHS内固定术

A: 术前X线片示右股骨粗隆间骨折;B: 术前CT三维重建; C: 术后X线片示髓内钉术后,骨折对位对线好; D: 末次随访X线片,示骨折愈合
图2患者女,79岁,右股骨粗隆间骨折,Evans Ⅰc型,行闭合复位Intertan内固定术
3讨论
3.1DHS和股骨近端髓内钉Intertan治疗股骨粗隆间骨折的特点[12]DHS的特点:套筒钢板有不同规格的颈干角,由于内固定器结构上滑动螺钉和钢板将骨折远近端牢固固定,抗弯强度强,并能恢复内侧稳定性,较适用于稳定型的股骨粗隆间骨折。但是,由于无有效的抗旋转作用,DHS不能有效防止骨折端旋转移位。此外,DHS内固定术切口大,出血常较多。Intertan的特点:Intertan系统的生物力学特性符合生物负重力线,股骨距区压应力减小,应力遮挡小,有助于骨折愈合。髓内针上、下端均有锁定交锁,可以防止骨折段的各种移位及髓内针旋转、下沉,起静力交锁作用。近端梯形的横断面采用关节假体柄设计原理,增强了稳定性,较小的近端最大程度地保留了正常骨质及周围软组织。因此,Intertan系统适用于几乎所有类型的股骨粗隆间骨折。不过,主钉进针点的选择偏差及暴力操作容易使骨折移位加重,甚至造成新的骨折。
本研究中,DHS组4例患者出现术后切口液化,虽然经过换药处理后愈合,但延长了住院时间及功能恢复。Intertan作为髓内固定,适应证范围广,几乎可用于所有的股骨骨折,如股骨颈骨折,顺、逆转子间骨折,转子下骨折等,其中尤其适用于股骨多段骨折。对于不稳定型的股骨粗隆间骨折,重建钉较接骨板具有固定牢固、防旋转等优点。
3.2手术技巧DHS:加压髋螺钉由套筒式钢板、近端拉力螺钉及远端多枚螺钉组成。近端套筒与钢板成130°或135°;套筒长度为25~38 mm,当中可通过拉力螺钉插入股骨头中,通过滑动给予折线加压;钢板有2~14个孔、60~300 mm长,拧入螺钉后可自动加压。导针位置在正位股骨头中央或偏头内下,侧位在略偏头的后部或中部。为防止钻孔及攻丝过程中骨折旋转,可在导针上方1.5 cm处插入1枚导针以临时固定,选择合适拉力的螺钉及钢板。 Intertan:暴露大粗隆的梨状窝进针点,插入导针,切忌暴力,避免引起大粗隆顶点的骨折;将导针插入远端,如果复位困难,可用股骨外侧小切口,使导针进入远端达骺线处;扩髓后将选定的髓内针固定于近端瞄准器上,插入髓内针。调整近端瞄准器,使2枚锁钉位于股骨颈及头的中央,以防止术后因锁钉偏向外上方而发生“割头”并发症。远端锁定以加强固定。
综上所述,DHS和Intertan治疗股骨粗隆间Evans Ⅰ型骨折都可以达到解剖复位与坚强内固定的效果。本研究中Intertan组的住院时间短于DHS组,髋关节功能优于DHS组,这主要得益于股骨近端髓内钉内固定的手术创伤小,从而降低了早期并发症,提高了早期功能锻炼的效率,促进髋关节功能恢复。
参考文献
[ 1 ]李意, 李新志.股骨粗隆间骨折内固定手术治疗的研究进展[J].重庆医学,2013,42(10):1172-1175.
[ 2 ]赵洪普, 徐秋玉, 吕玉明, 等. 三种内固定方法(PFNA、LPFP、DHS)治疗老年股骨粗隆间骨折的比较[J]. 中国骨与关节损伤杂志, 2012, 27(6):500-502.
[ 3 ]Imren Y, Gurkan V, Bilsel K, et al. Biomechanical comparison of dynamic hip screw, proximal femoral nail, cannulated screw, and monoaxial external fixation in the treatment of basicervical femoral neck fractures[J]. Acta Chir Orthop Traumatol Cech, 2015, 82(2): 140-144.
[ 4 ]Li YJ, Li ZB, Yu WH, et al. Case-control study on dynamic hip screw and proximal femoral nail anti-rotation for the treatment of unstable intertrochanteric fractures in elderly patients[J]. Zhongguo Gu Shang, 2013, 26(12): 977-980.
[ 5 ]Ma KL, Wang X, Luan FJ, et al. Proximal femoral nails antirotation, Gamma nails, and dynamic hip screws for fixation of intertrochanteric fractures of femur: A meta-analysis[J]. Orthop Traumatol Surg Res, 2014, 100(8): 859-866.
[ 6 ]Shah AA, Kumar S, Rashid RH, et al. Dynamic hip screw fixation for inter-trochanteric fractures: determinants of outcomes[J]. J Pak Med Assoc, 2014;64(12 Suppl 2): S95-S99.
[ 7 ]Kim JW, Kim TY, Ha YC, et al. Outcome of intertrochanteric fractures treated by intramedullary nail with two integrated lag screws: A study in Asian population[J]. Indian J Orthop, 2015, 49(4): 436-441.
[ 8 ]徐明伟, 周荣魁. 股骨近端抗旋髓内钉治疗老年股骨粗隆间骨折患者的效果及安全性[J]. 中国老年学杂志, 2015, 35(16):4616-4617.
[ 9 ]Zhang PX, Xue F, An S, et al. Clinical analysis of obvious and hidden blood loss in inter-trochanter fracture patients treated with proximal femoral nail anti-rotation and dynamic hip screw[J]. Beijing Da Xue Xue Bao, 2012, 44(6): 891-894.
[10]Nizamoglu M. Pyoderma gangrenosum mimicking an infected wound following dynamic hip screw fixation[J]. Case Rep Orthop, 2015, 2015: 571472.
[11]徐诗雄,洪顺红,孙文栋.老年股骨粗隆间骨折术后髋关节功能恢复的影响因素[J]. 中国老年学杂志, 2014, 7(12):3353-3355.
[12]Zehir S, Zehir R, Zehir S, et al. Proximal femoral nail antirotation against dynamic hip screw for unstable trochanteric fractures; a prospective randomized comparison[J]. Eur J Trauma Emerg Surg, 2015, 41(4): 393-400.
通讯作者李展春, E-mail: kcb069@163.com
基金项目:国家自然科学基金资助项目(编号:81370976、81400904);上海市自然科学基金资助项目(编号:13ZR1424900);上海交通大学医工交叉基金项目(编号:YG2014MS41)
中图分类号R 683.42
文献标识码A
