广西地区人群CD36基因rs17154181和rs1761667位点多态性与2型糖尿病大血管病变的关系
2015-02-22庞翠军肖常青潘海林廖碧芝张峥嵘
袁 雁,庞翠军,肖常青,潘海林,宋 琳,廖碧芝,张峥嵘
·论著·
广西地区人群CD36基因rs17154181和rs1761667位点多态性与2型糖尿病大血管病变的关系
袁 雁,庞翠军,肖常青,潘海林,宋 琳,廖碧芝,张峥嵘
目的 探讨CD36基因rs17154181、rs1761667位点多态性与2型糖尿病患者发生大血管病变的关系。方法 选取2012年12月—2014年6月于广西医科大学第一附属医院内分泌代谢科住院治疗的2型糖尿病患者112例为病例组,并选取同期于本院体检健康者65例为对照组。记录两组一般资料,并检测相关生化指标。提取外周血DNA,CD36基因rs17154181和rs1761667经PCR扩增后分析基因型。结果 两组CD36基因rs17154181、rs1761667位点基因型和等位基因频率比较,差异无统计学意义(P>0.05)。病例组不同程度糖尿病大血管病变患者年龄、总胆固醇(TC)、三酰甘油(TG)水平比较,差异有统计学意义(P<0.05);其中,临床动脉粥样硬化和亚临床动脉粥样硬化患者年龄大于无大血管病变患者,TC水平低于无大血管病变患者;亚临床动脉粥样硬化患者TG水平低于无大血管病变患者(P<0.05)。病例组不同程度糖尿病大血管病变患者CD36基因rs17154181、rs1761667位点基因型及等位基因频率比较,差异均无统计学意义(P>0.05)。病例组rs17154181位点不同基因型患者收缩压比较,差异有统计学意义(P<0.05),其中,基因型AG患者收缩压高于基因型AA患者(P<0.05)。多因素Logistic回归分析显示,年龄、合并高血压、低密度脂蛋白胆固醇(LDL-C)进入回归方程,是2型糖尿病患者发生糖尿病大血管病变的影响因素(P<0.05),而rs17154181、rs1761667位点基因型未进入回归方程(P>0.05)。结论 本研究未发现CD36基因rs17154181、rs1761667位点多态性与广西地区2型糖尿病患者发生大血管病变有关,其多态性可能不是CD36与糖脂代谢有关的功能性多态位点。
糖尿病,2型;糖尿病血管病变;CD36;多态性,单核苷酸
袁雁,庞翠军,肖常青,等.广西地区人群CD36基因rs17154181和rs1761667位点多态性与2型糖尿病大血管病变的关系[J].中国全科医学,2015,18(20):2421-2425.[www.chinagp.net]
Yuan Y,Pang CJ,Xiao CQ,et al.Relationship between the polymorphism of rs17154181 and rs1761667 sites of CD36 gene and macroangiopathy in patients with type 2 diabetes mellitus in Guangxi province[J].Chinese General Practice,2015,18(20):2421-2425.
糖尿病大血管病变是2型糖尿病患者常见并发症,早期可仅表现为动脉内膜厚度增厚或斑块形成,随着病情的发展可由亚临床动脉粥样硬化进展为临床动脉粥样硬化,发生严重心脑血管事件的风险增加[1]。在动脉粥样硬化形成早期,巨噬细胞吞噬氧化型的低密度脂蛋白(oxLDL)转化为泡沫细胞是粥样斑块形成的关键步骤。而CD36是巨噬细胞膜上oxLDL的主要受体,参与炎性反应、止血、免疫清除、脂质代谢和动脉粥样硬化等多种生理和病理过程[2]。CD36可能存在多个功能性多态位点,与心脑血管、糖脂代谢等相关代谢性疾病的发生相关[3]。本研究通过探讨广西地区2型糖尿病患者CD36基因rs17154181、rs1761667位点多态性与2型糖尿病大血管病变的关系,分析2型糖尿病大血管病变的发生机制,为改善2型糖尿病患者预后提供依据。
1 资料与方法

1.2 方法
1.2.1 一般资料 测量身高、体质量、血压,若收血压≥140/90 mm Hg(1 mm Hg=0.133 kPa),或血压正常但正服用降压药物则诊断为合并高血压,记录糖尿病病程及吸烟史。
1.2.2 生化指标检测 空腹12 h后采集静脉血2 ml,EDTA抗凝管抗凝,送本院实验室检测空腹血糖(FBG)、餐后2 h血糖(2 h PBG)、糖化血红蛋白(HbA1c)、总胆固醇(TC)、三酰甘油(TG)、低密度脂蛋白胆固醇(LDL-C)、高密度脂蛋白胆固醇(HDL-C)。
1.2.3 大血管病变诊断标准 亚临床动脉粥样硬化诊断标准:颈总动脉、股动脉、髂总动脉经彩色多普勒超声检查任一部位内膜中层厚度>1.0 mm和/或出现粥样硬化斑块且无临床症状表现。临床动脉粥样硬化的诊断标准:(1)下肢大血管病变:有间歇性跛行、休息痛,足背动脉搏动消失,甚至有足缺血性溃疡或坏疽表现,均经外周血管超生检查证实外周血管动脉粥样硬化有缺血表现或闭塞;(2)冠心病:有典型心绞痛或心肌梗死病史,或心电图、冠状动脉造影明确诊断心肌缺血或冠状动脉狭窄;(3)出现偏瘫或其他脑局灶症状,或颅脑CT、MRI显示有缺血或出血改变。
1.2.4 DNA提取及基因型分析 采用苯酚三氯甲烷提取外周血细胞基因组DNA,溶于TE液中-20 ℃保存待用。rs17154181位点引物序列设计参考文献[2],rs1761667位点引物应用Primer 5.0软件设计,并经Oligo 7软件评价,均由生工生物(上海)工程有限公司合成。rs17154181位点引物序列上游引物:5′-CAAACATTACAGCAGAACT-3′,下游引物:5′-TATTTACCAAGACAACCC-3′;rs1761667位点引物序列上游引物:5′-TATCCACCTGTTTTCCTCACT-3′,下游引物:5′-GACTCTTCCATTTGTTTTGGT-3′。 PCR反应体系为25 μl,包括12 μl Premix Taq(大连宝生物工程有限公司),上下游引物各0.5 μl(20 pmol/μl),DNA模板1 μl(50~300 ng/μl),不足部分由双蒸水补充。rs17154181位点PCR扩增参数:预变性95 ℃,10 min,变性94 ℃,1 min,退火51 ℃,30 s,延伸72 ℃,1 min,变性、退火、延伸30个循环后,再次延伸72 ℃,7 min。rs1761667PCR位点PCR扩增参数:预变性95 ℃,10 min,变性94 ℃,1 min,退火56 ℃,30 s,延伸72 ℃,1 min,变性、退火、延伸30个循环后,再次延伸72 ℃,7 min。
限制性内切酶通过在线软件NEB CUTTER选定,消化反应进行基因型分析。酶切反应体系为20 μl,包括PCR产物10 μl,10倍稀释buffer缓冲液1 μl,限制性内切酶3~5 U(大连宝生物工程有限公司),不足部分由双蒸水补充。37 ℃恒温箱孵育4~6 h后,2%琼脂糖凝胶(核酸染料GREEN染色),100 V电泳30 min后紫外灯下确定基因型。

2 结果
2.1 两组CD36基因rs17154181、rs1761667位点多态性分析CD36基因rs17154181、rs1761667位点基因频率分布符合Hardy-Weinberg遗传平衡,具有群体代表性(χ2=0.742、0.921,P=0.631)。两组CD36基因rs17154181、rs1761667位点基因型和等位基因频率分布比较,差异无统计学意义(P>0.05,见表1)。
2.2 病例组不同程度糖尿病大血管病变患者临床特征比较 病例组不同程度糖尿病大血管病变患者糖尿病病程、体质指数(BMI)、收缩压、舒张压、FPG、2hPBG、HbA1c、LDL-C和HDL-C水平比较,差异无统计学意义(P>0.05)。病例组不同程度糖尿病大血管病变患者年龄、TC、TG水平比较,差异有统计学意义(P<0.05);其中,临床动脉粥样硬化和亚临床动脉粥样硬化患者年龄大于无大血管病变患者,TC水平低于无大血管病变患者;亚临床动脉粥样硬化患者TG水平低于无大血管病变患者(P<0.05,见表2)。
2.3 病例组不同程度糖尿病大血管病变患者基因型及等位基因频率比较 病例组不同程度糖尿病大血管病变患者CD36基因rs17154181、rs1761667位点基因型及等位基因频率比较,差异均无统计学意义(P>0.05,见表3)。
表1 两组CD36基因rs17154181、rs1761667位点基因型及等位基因频率比较(n)
Table 1 Comparison of genotype and alleles frequency of rs17154181 and rs1761667 sites of CD36 gene between the two groups
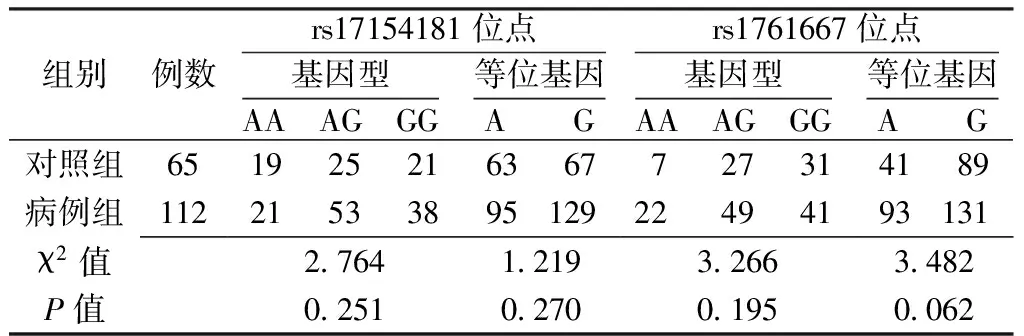
组别例数rs17154181位点基因型AA AG GG 等位基因A Grs1761667位点基因型AA AG GG 等位基因A G对照组651925216367727314189病例组1122153389512922494193131χ2值2764121932663482P值0251027001950062
表3 病例组不同程度糖尿病大血管病变患者CD36基因rs17154181、rs1761667位点基因型及等位基因频率比较(n)
Table 3 Comparison of genotype and alleles frequency of rs17154181 and rs1761667 sites of CD36 gene among diabetic patients with different levels of macroangiopathy in the case group

病变程度例数rs17154181位点基因型AA AG GG 等位基因A Grs1761667位点基因型AA AG GG 等位基因A G无糖尿病大血管病变39618153048617162949临床动脉粥样硬化2761110233161292430亚临床动脉粥样硬化469241342501021154151χ2值1661089510521125P值0798063909020570

表2 病例组不同程度糖尿病大血管病变患者临床特征比较
注:FBG=空腹血糖,2 h PBG=餐后2 h血糖,HbA1c=糖化血红蛋白,TC=总胆固醇,TG=三酰甘油,LDL-C=低密度脂蛋白胆固醇,HDL-C=高密度脂蛋白胆固醇;与无大血管病变比较,aP<0.05;b为u值
2.4 病例组CD36基因rs17154181、rs1761667位点不同基因型患者临床特征比较 病例组rs17154181位点不同基因型患者收缩压比较,差异有统计学意义(P<0.05),其中,基因型AG患者收缩压高于基因型AA患者(P<0.05)。病例组rs17154181位点不同基因型患者BMI、舒张压、FPG、2 h PBG、HbA1c、TC、TG、LHL-C 和HDL-C水平比较,差异无统计学意义(P>0.05,见表4)。病例组rs1761667位点不同基因型患者BMI、收缩压、舒张压、FPG、2 h PBG、HbA1c、TC、TG、 LHL-C 和HDL-C水平比较,差异均无统计学意义(P>0.05,见表5)。
2.5 2型糖尿病患者发生糖尿病大血管病变影响因素的多因素Logistic分析 以病例组患者临床特征为自变量,是否发生糖尿病大血管病变为因变量行多因素Logistic回归分析。结果显示,年龄、合并高血压、LDL-C进入回归方程,是2型糖尿病患者发生糖尿病大血管病变的影响因素(P<0.05),而rs17154181、rs1761667位点基因型未进入回归方程(P>0.05,见表6)。
3 讨论
CD36是一类B族清道夫受体,广泛分布于单核细胞、巨噬细胞、血小板、红细胞、某些肿瘤细胞、内皮细胞、视网膜色素上皮细胞和脂肪细胞等细胞膜[2],参与体内多种病理生理活动,其介导的巨噬细胞对oxLDL的吞噬从而转化为泡沫细胞的过程在动脉粥样硬化发生发展中发挥重要作用[3]。Luo等[5]对新疆地区汉族、维吾尔族人群CD36基因多态性与急性冠脉综合征关系的研究发现,急性冠脉综合征患者rs17154181位点等位基因A频率低于健康人群。另外,rs1761667位点单核苷酸多态性与白人游离脂肪酸水平升高有关[6],而高水平的游离脂肪酸可降低外周组织对胰岛素的敏感性。CD36是游离脂肪酸的受体,其在肌肉和脂肪组织表达的差异性影响2型糖尿病患者对胰岛素的敏感性[7-8]。最近一项研究发现在非洲裔美国人群中rs1761667位点等位基因A与单核细胞CD36的表达减少有关,是动脉粥样硬化的保护因素[9]。
表6 2型糖尿病患者发生糖尿病大血管病变影响因素的多因素Logistic分析
Table 6 Multivariable Logistic regression analysis on influencing factors for macroangiopathy in patients with type 2 diabetes mellitus

变量bSEWaldχ2值OR(95%CI)P值年龄02220053175371249(1125,1386)<0001BMI-0140011514810870(0694,1089)0224合并高血压2143074414818527(1985,36625)0004吸烟史-0050072500050951(0230,3941)0928糖尿病病程-0151007639530860(0740,1108)0077FBG-0083014503280920(0693,1223)05672hPBG0057010303061059(0865,1297)0580HbA1c0053014801271054(0789,1408)0721TC-2524083591400080(0016,1012)0080TG0074024500921077(0666,1743)0762LDL-C3070105185288551(2745,69223)0003HDL-C0273104100691314(0171,10144)0793rs17154181位点基因型 GG---1- AA1794117023536016(0608,59574)0125 AG0281075501381324(0301,5820)0710rs1761667位点基因型 GG---1- AA0879108906522409(0285,20349)0721 AG0390091106541477(0247,8801)0419
注:-表示无此数据

表4 病例组rs17154181位点不同基因型患者临床特征比较±s)
注:与基因型AA比较,aP<0.05
表5 病例组rs1761667位点不同基因型患者临床特征比较±s)
一项在印度人群中开展的研究表明,2型糖尿病患者CD36基因rs3211938位点等位基因G频率高于健康人群[10]。而本研究结果显示,病例组和对照组rs17154181、rs176166位点基因型和等位基因频率并无差异,提示该基因位点多态性可能不是2型糖尿病的易患多态位点。本研究对照组和病例组rs17154181位点等位基因A的频率分别为48.5%(63/130)和42.4%(95/224),均高于新疆人群的33.8%[5];对照组和病例组rs1761667位点等位基因A的频率分别是31.5%(41/130)和41.5(93/224),低于墨西哥人群的58%[11],rs17154181、rs176166位点等位基因分布是否有地域差异,尚需更大样本量的研究进一步证实。
Rac等[12]对CD36基因多态性与动脉粥样硬化斑块厚度关系的研究发现,外显子6等位基因为573A、591T的患者动脉粥样硬化斑块厚度较薄。本研究病例组不同程度糖尿病大血管病变患者CD36基因rs17154181、rs176166位点基因型和等位基因频率无差异,提示该位点可能不是功能性位点,对动脉粥样硬化的发生发展无影响。多因素Logistic回归分析显示,年龄是2型糖尿病患者发生糖尿病大血管病变及亚临床动脉粥样硬化的危险因素,与Trinity等[13]研究结果一致。
2型糖尿病是环境因素和多基因共同作用的结果,单基因对糖脂代谢及动脉粥样硬化的贡献大小尚不得而知,需要更大样本量、更深入的基础实验加以阐明。今后的研究需探讨CD36表达水平与2型糖尿病大血管病变的关系,更加客观地反映两者的关联性。此外,由于CD36基因多态性有明显的民族、地域差异,对CD36基因多态性的研究尚需在更大地区、更广人群中进行。
[1]Matsushita K,Sang Y,Ballew SH,et al.Subclinical atherosclerosis measures for cardiovascular prediction in CKD[J].J Am Soc Nephrol,2015,26(2):439-447.
[2]Nergiz-Unal R,Rademakers T,Cosemans JM,et al.CD36 as a multiple-ligand signaling receptor in atherothrombosis[J].Cardiovasc Hematol Agents Med Chem,2011,9(1):42-55.
[3]Kennedy DJ,Kuchibhotla S,Westfall KM,et al.A CD36-dependent pathway enhances macrophage and adipose tissue inflammation and impairs insulin signalling[J].Cardiovasc Res,2011,89(3):604-613.
[4] Xu XJ,Pan CY,Tian H,et al.Analysis and evaluation of the diagnosis criteria of World Health Organization and American Diabetes Association for diabetes mellitus in senile population[J].Chinese Journal of Endocrinology and Metabolism,2002,18(5):27-31.(in Chinese) 徐向进,潘长玉,田慧,等.WHO及美国糖尿病学会糖尿病诊断标准在老年人群中应用的分析和评估[J].中华内分泌代谢杂志,2002,18(5):27-31.
[5]Luo J,Ma Y,Xie X,et al.Association between the single nucleotide polymorphisms of human CD36 gene and acute coronary syndrome[J].Zhonghua Liu Xing Bing Xue Za Zhi,2014,35(2):200-204.
[6]Ma X,Bacci S,Mlynarski W,et al.A common haplotype at the CD36 locus is associated with high free fatty acid levels and increased cardiovascular risk in Caucasians[J].Hum Mol Genet,2004,13(19):2197-2205.
[7]Pietka TA,Schappe T,Conte C,et al.Adipose and muscle tissue profile of CD36 transcripts in obese subjects highlights the role of CD36 in fatty acid homeostasis and insulin resistance[J].Diabetes Care,2014,37(7):1990-1997.
[8]Corpeleijn E,van der Kallen CJ,Kruijshoop M,et al.Direct association of a promoter polymorphism in the CD36/FAT fatty acid transporter gene with type 2 diabetes mellitus and insulin resistance[J].Diabet Med,2006,23(8):907-911.
[9]Love-Gregory L,Sherva R,Schappe T,et al.Common CD36 SNPs reduce protein expression and may contribute to a protective atherogenic profile[J].Hum Mol Genet,2011,20(1):193-201.
[10]Gautam S,Pirabu L,Agrawal CG,et al.CD36 gene variants and their association with type 2 diabetes in an Indian population[J].Diabetes Technol Ther,2013,15(8):680-687.
[11]Ramos-Arellano LE,Salgado-Bernabé AB,Guzmán-Guzmán IP,et al.CD36 haplotypes are associated with lipid profile in normal-weight subjects[J].Lipids Health Dis,2013(12):167.
[12]Rac ME,Safranow K,Rac M,et al.CD36 gene is associated with thickness of atheromatous plaque and ankle-brachial index in patients with early coronary artery disease[J].Kardiol Pol,2012,70(9):918-923.
[13]Trinity JD,Groot HJ,Layec G,et al.Impact of age and body position on the contribution of nitric oxide to femoral artery shear rate:implications for atherosclerosis[J].Hypertension,2014,63(5):1019-1025.
(本文编辑:吴立波)
Relationship Between the Polymorphism of rs17154181 and rs1761667 Sites of CD36 Gene and Macroangiopathy in Patients With Type 2 Diabetes Mellitus in Guangxi Province
YUANYan,PANGCui-jun,XIAOChang-qing,etal.
DepartmentofEndocrinologyandMetabolism,theFirstAffiliatedHospitalofGuangxiMedicalUniversity,Nanning530021,China
Objective To investigate the relationship between the polymorphism of rs17154181 and rs1761667 sites of CD36 gene and macroangiopathy in patients with type 2 diabetes mellitus in Guangxi Province.Methods We enrolled 112 patients with type 2 diabetes mellitus who received hospitalized treatment in the Department of Endocrinology and Metabolism of the First Affiliated Hospital of Guangxi Medical University from December 2012 to June 2014 as the case group.Another 65 healthy people who underwent physical examination in the same period were enrolled as control group.General data were recorded,and relevant biochemical indicators were tested.DNA in peripheral blood was extracted ,and through PCR amplification of rs17154181 and rs1761667 sites of CD36 gene,genotypes were determined.Results The two groups were not significantly different(P>0.05) in the distribution of genotypes and allele frequency at rs17154181 and rs1761667 sites of CD36 gene.In the case group,the diabetic patients with different levels of macroangiopathy were significantly different(P<0.05) in age,TC and TG;patients with clinical arteriosclerosis and subclinical arteriosclerosis were higher(P<0.05) in age and were lower(P<0.05) in TC level than the diabetic patients without macroangiopathy;diabetic patients with subclinical arteriosclerosis were lower(P<0.05) than the diabetic patients without macroangiopathy in TG level.In the case group,the diabetic patients with different levels of macroangiopathy were not significantly different(P>0.05) in the rs 17154181 and rs 1761667 genotypes of CD36 genes and allele frequency.In the case group,patients with different genotypes of rs17154181 site were significantly different(P<0.05) in systolic pressure;patients with AG genotype were higher(P<0.05) than patients with AA genotype in systolic pressure.The multivariate logistic regression analysis showed that age,complicated hypertension and LDL-C entered the regression equation,which indicated that these factors were the influencing factors for macroangiopathy in patients with type 2 diabetes mellitus.The genotypes at rs17154181 and rs1761667 sites didn′t enter the regression equation(P>0.05).Conclusion No correlation was found between the polymorphisms of rs17154181 and rs1761667 sites of CD36 gene and macroangiopathy in patients with type 2 diabetes mellitus.The two sites may be not the CD36 functional polymorphism sites relevant with glucolipid metabolism.
Diabetes mellitus,type 2;Diabetic angiopathies;CD36;Polymorphism,single nucleotide
广西自然科学基金资助项目(2011GXNSFA018257);广西中医药管理局基金项目(GZKZ10-113)
530021广西南宁市,广西医科大学第一附属医院内分泌代谢科
庞翠军,530021广西南宁市,广西医科大学第一附属医院内分泌代谢科;E-mail:pangcuijun@qq.com
R 587.23
A
10.3969/j.issn.1007-9572.2015.20.015
2015-03-08;
2015-06-03)
