Changes in lumbosacral spinal nerve roots on diff usion tensor imaging in spinal stenosis
2015-02-07ZhongjunHouYongHuangZiwenFanXinchunLiBingyiCao
Zhong-jun Hou, Yong Huang Zi-wen Fan, Xin-chun Li, Bing-yi Cao
1 Department of Radiology, the Second Affi liated Hospital of Guangzhou Medical University, Guangzhou, Guangdong Province, China
2 Department of Orthopedics, the Second Affi liated Hospital of Guangzhou Medical University, Guangzhou, Guangdong Province, China
3 Department of Radiology, the First Affi liated Hospital of Guangzhou Medical University, Guangzhou, Guangdong Province, China
Changes in lumbosacral spinal nerve roots on diff usion tensor imaging in spinal stenosis
Zhong-jun Hou1,*, Yong Huang1, Zi-wen Fan2, Xin-chun Li3, Bing-yi Cao1
1 Department of Radiology, the Second Affi liated Hospital of Guangzhou Medical University, Guangzhou, Guangdong Province, China
2 Department of Orthopedics, the Second Affi liated Hospital of Guangzhou Medical University, Guangzhou, Guangdong Province, China
3 Department of Radiology, the First Affi liated Hospital of Guangzhou Medical University, Guangzhou, Guangdong Province, China
Lumbosacral degenerative disc disease is a common cause of lower back and leg pain. Conventional T1-weighted imaging (T1WI) and T2-weighted imaging (T2WI) scans are commonly used to image spinal cord degeneration. However, these modalities are unable to image the entire lumbosacral spinal nerve roots. Thus, in the present study, we assessed the potential of diff usion tensor imaging (DTI) for quantitative assessment of compressed lumbosacral spinal nerve roots. Subjects were 20 young healthy volunteers and 31 patients with lumbosacral stenosis. T2WI showed that the residual dural sac area was less than two-thirds that of the corresponding normal area in patients from L3to S1stenosis. On T1WI and T2WI, 74 lumbosacral spinal nerve roots from 31 patients showed compression changes. DTI showed thinning and distortion in 36 lumbosacral spinal nerve roots (49%) and abruption in 17 lumbosacral spinal nerve roots (23%). Moreover, fractional anisotropy values were reduced in the lumbosacral spinal nerve roots of patients with lumbosacral stenosis. These fi ndings suggest that DTI can objectively and quantitatively evaluate the severity of lumbosacral spinal nerve root compression.
nerve regeneration; magnetic resonance imaging; diffusion tensor imaging; lumbosacral area; degeneration; nerve root; fractional anisotropy; neural regeneration
Funding: This study was supported by the Science and Technology Planning Project of Guangdong Province of China in 2012, No. 2012B031800232.
Hou ZJ, Huang Y, Fan ZW, Li XC, Cao BY (2015) Changes in lumbosacral spinal nerve roots on diffusion tensor imaging in spinal stenosis. Neural Regen Res 10(11):1860-1864.
Introduction
Lumbosacral degenerative disc disease is the most common cause of pain in the lower back and legs. The most common levels of disc degeneration are at L4–5and L5to S1(Quint and Wilke, 2008; Hicks et al., 2009; Saleem et al., 2013). X-ray imaging plays a limited role in evaluating functional impairment associated with spinal cord degeneration (Quint and Wilke, 2008). Furthermore, the severity of lower back pain does not match the degree of disc degeneration and facet joint pathology on radiographs (Hicks et al., 2009).
Conventional magnetic resonance imaging (MRI), including T1-weighted imaging (T1WI) and T2-weighted imaging (T2WI), can image lumbosacral disc degeneration, but does not image the entire lumbosacral spinal nerve roots (LSNR). Three-dimensional (3D) MR radiculography is able to display the morphology of LSNR, although it has poor image rending quality (Byun et al., 2012).
Diff usion weighted imaging (DWI) can provide valuable structural information and the apparent diff usion coeffi cient of the LSNR. DWI neuroimaging can visualize abnormalities such as nerve indentation, swelling, and transverse nerve direction through the foramen, and can quantitatively evaluate lumbar nerve entrapment in patients with foraminal stenosis. However, the resolution of the apparent diff usion coeffi -cient map is unsatisfactory and the limited directions of the gradient magnetic fi elds may aff ect the apparent diff usion coeffi cient value (Eguchi et al., 2010).
Diff usion tensor imaging (DTI) has been used to image nerve fi ber tracts in the white matter of the central nervous system, and can also display peripheral nerve fi bers (Li et al., 2013; Jang et al., 2014). Nevertheless, the application of DTI is less common for evaluation of LSNR morphology and pathology (Filippi et al., 2010; Eguchi et al., 2011). Clinical practice requires quantitative evaluation of the degree of trauma and recovery after treatment in LSNR (Arrigo et al., 2011). In the present study, we performed conventional MRI versus DTI in the lumbosacral spine to evaluate the LSNR in both healthy volunteers and patients with spinal stenosis. The aim of this study was to examine the potential of DTI for intuitive and quantitative assessment of the compressed LSNR.
Materials and Methods
Subjects
A total of 20 young healthy volunteers and 93 patients with lumbosacral stenosis were verifi ed by physical examination in the Department of Orthopedics of the Second Affi liated Hospital of Guangzhou Medical University, China. For healthy volunteers, there were 14 males (mean age 23.3 ± 1.7 years; range: 21–27 years) and six females (22.8 ± 1.9 years; range: 21–26 years) as a control group.
Conventional MRI
After signing informed consent, MRI scans were performed with a scanner (Signa 1.5T HDXT; General Electric, Milwaukee, WI, USA). For conventional examination, sagittal planes were oriented from the 10ththoracic vertebra to the coccyx on T1WI and T2WI, while axial T2WI scans were performed along the intervertebral spaces from L3to S1to assess intervertebral disc changes. Axial T2WI and DTI scans were then performed in horizontal orientation from the upper-middle part of the L2to the inferior margin of S1with 8-channel cardiac array coils.
The following scanning parameters were maintained for horizontal T2WI and DTI for orientation, slice thickness, number of slices, fi eld of view, and zero gap. For axial T2WI, the scanning parameters were repetition time of 3,720.0–3,880.0 ms, echo time of 80.1–89.6 ms, slice thickness of 3 mm, fi eld of view of 300 × 300 mm, matrix of 256 × 256, echo length of 16, number of slices of 50, signal excitations and acquisitions of 2, and scanning time from 2′44′′to 3′22′′. For DTI, the scanning parameters were repetition time of 10,000–10,400 ms, echo time of 71.8–72.1 ms, matrix of 128 × 128, signal excitations and acquisitions of 8, diff usion factors at b values of 0 s/mm2and 400 s/mm2, 12 directions of diff usion gradients, and scanning time from 17′30′′ to 18′12′′ in echo planar imaging.
For post processing, images were processed using Functool 5.2.09 on the MRI host computer. First, on axial scans of intervertebral discs, the areas of the dural sacs were measured from L3to S1in both healthy volunteers and patients. At each level, the areas of the dural sacs were then measured three times and averaged.
Patient selection
Patients who exhibited the following symptoms were selected: intermittent claudication, numbness, and weakness that could be relieved by bed rest and bending motion or aggravated by extension of the legs. In a clinical test, patients exhibited altered sensation disturbances in the back and legs, weakening or disappearance in ankle refl ection, and atrophy in the buttocks and legs. One patient exhibited cauda equina syndrome characterized by serious low back pain, radicular pain in both legs, numbness around the anus, urine retention, and fecal incontinence. With respect to accessing standards, only those patients without a metal frame of the vertebral body and dural sac area less than two-thirds of that at the corresponding normal intervertebral spaces were included in this study (Feng et al., 2000). Thirty-one patients out of 93 exhibited this requirement. The lesion group contained 18 males (mean 51.0 ± 9.1 years; range: 33–63 years) and 13 females (62.5 ± 13.9 years; range: 39–80).
DTI data analysis
In post processing of DTI data, after comparing the shape and contours of the dural sac on axial T2WI and DTI and ruling out image deformation, we selected one of 12 groups of DTI with 50 images, and then reconstructed the spinal nerves and ganglia on the maximum intensity projection. DWI neuroimaging in one direction was used as the reference for DTI tractography. To mark the nerve roots at the cauda equina and the dorsal root ganglia, the fractional anisotropy (FA) values of LSNR were measured in triplicate at each site; the positions were recorded for selecting the region of interest and tracking LSNR. The ‘seed’ and ‘target’ mode were used by referring the regions of interest of the proximal and distal ends of the LSNR on 3D axial DTI images. Images of the LSNR from L3to S1on both sides were reconstructed using an FA threshold of 0.18.
Statistical analysis
Data were analyzed using SPSS 11.5 software (SPSS, Chicago, IL, USA). The dural sac area, between two-thirds of the normal and the narrowed lumbosacral canal, and FA values between healthy volunteers and patients in the lesion group were compared using the Student’s t-test. A P value less than 0.05 was considered statistically signifi cant.
Results
Dural sac area in healthy volunteers and patients with lumbosacral stenosis
In 20 healthy volunteers, the dural sac areas of the axial lumbosacral canals were 188.7 ± 45.0 mm2, 174.6 ± 44.0 mm2, and 156.6 ± 44.5 mm2at L3–4, L4–5, and L5to S1, respectively, and 173.0 ± 46.1 mm2on average. The residual dural sac area of the lumbosacral canal was reduced in patients with lumbosacral stenosis (98.9 ± 25.6 mm2) to two-thirds of the dural sac area of normal persons (115.3 ± 30.7 mm2) (t = 4.719, P = 0.000).
FA values of LSNR from L2to S1between healthy
volunteers and patients with lumbosacral canal stenosis
The mean FA value was higher in healthy volunteers (0.332 ± 0.074) than that in patients with lumbosacral canal stenosis (0.304 ± 0.085) (P = 0.000).
Neuroimaging and tractography of LSNR
In healthy volunteers, DWI showed symmetrical or almost symmetrical LSNR from L3to S1, which was very clear from the bifurcation of the LSNR in the cauda equina to the dorsal ganglia. The LSNR from L2to S1was observed completely on DTI tractography, which corresponded to DWI neuroimaging and normal anatomy (Figure 1) (Arslan et al., 2011). Lumbosacral degeneration was seen in 74 LSNR of patients with spinal stenosis on T1WI and T2WI. On DTI tractography, 36 LSNR (49%) were thin and distorted, while 17 LSNR (23%) were ruptured (Figures 2 and 3). Morphologically, the most evident signs were asymmetry and distortion of the LSNR. Overall, these data suggest that the compression state of the ruptured LSNR on DTI was more serious than that of thinning and distortion observed with T1WI and T2WI.
Discussion
Spinal degeneration and spinal stenosis
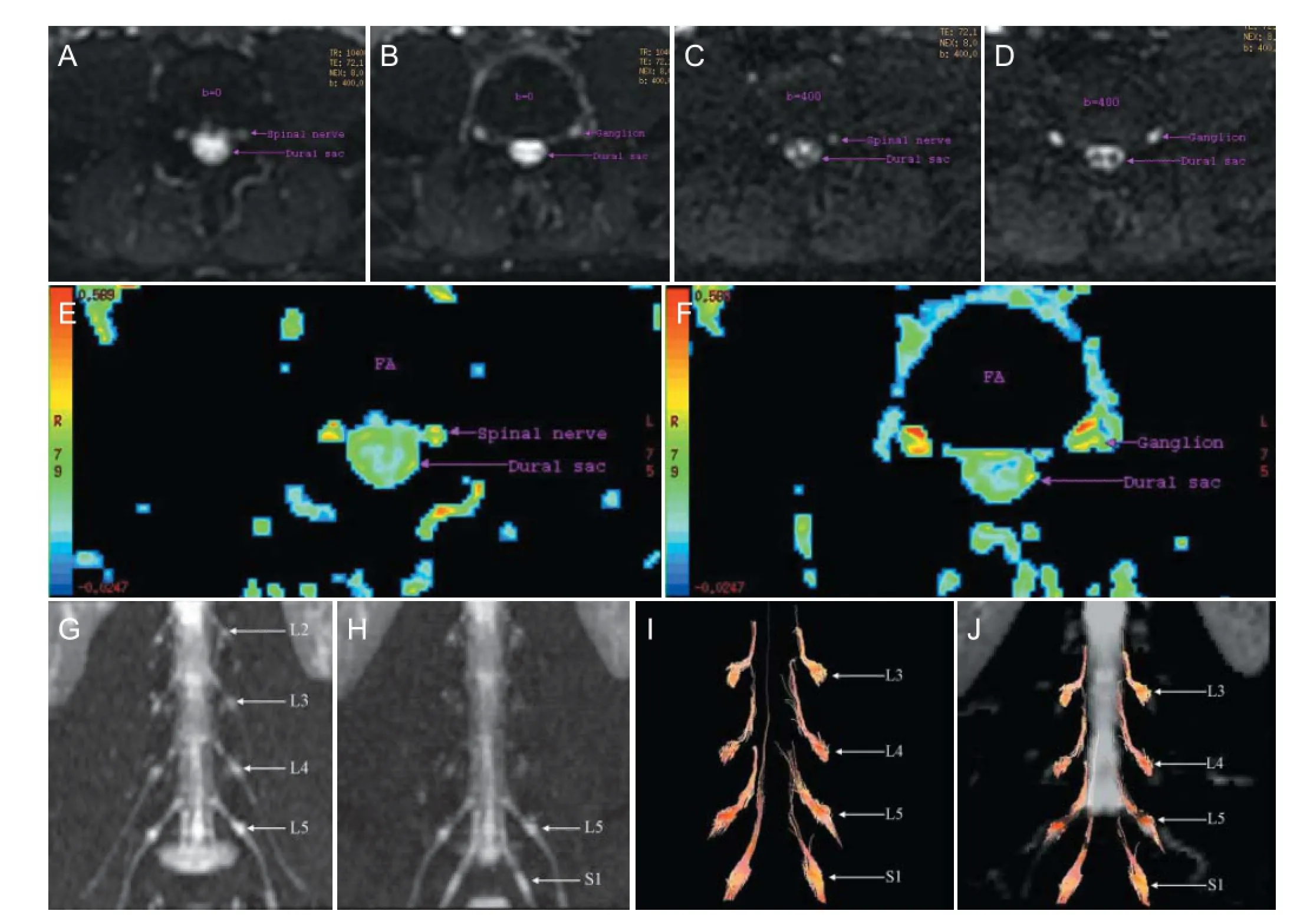
Figure 1 Images of LSNR of a 22-year-old male healthy volunteer.
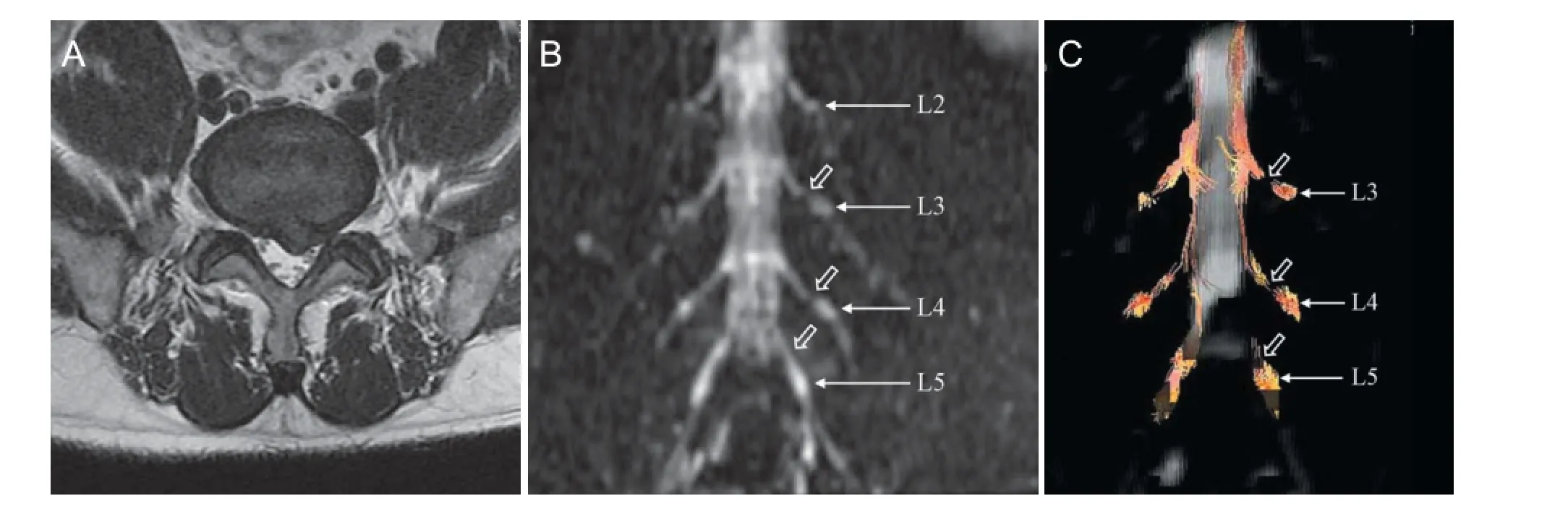
Figure 2 Changes in the LSNR of a 56-year-old male patient with spinal stenosis.
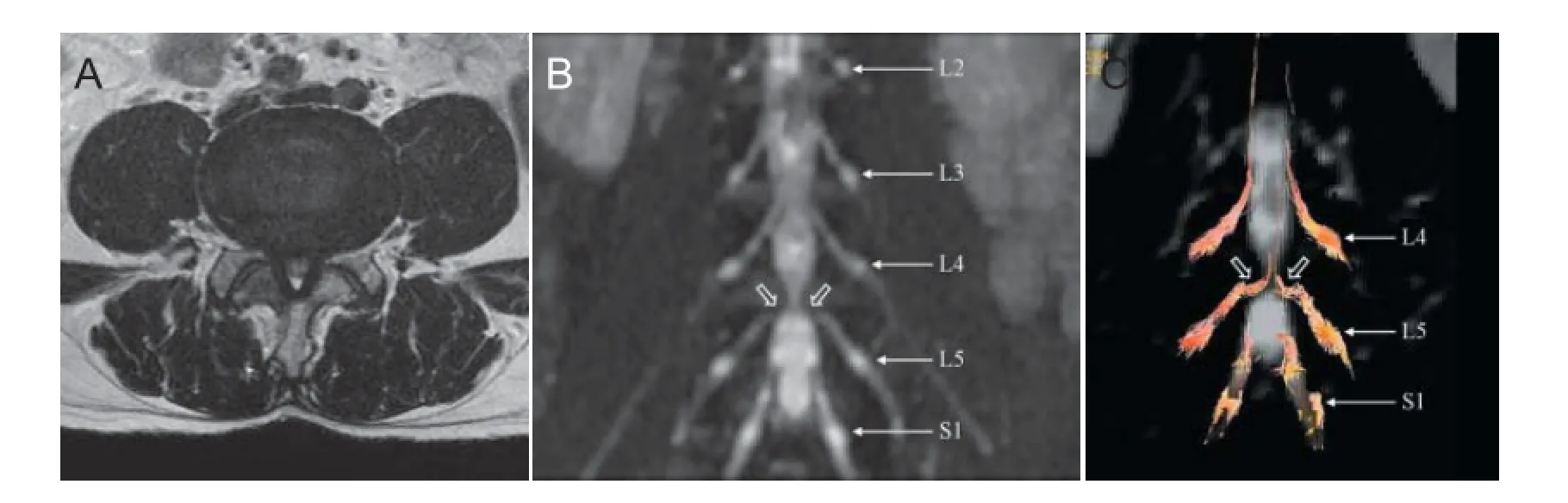
Figure 3 Changes in the LSNR of a 59-year-old male patient with spinal stenosis.
Senocak et al. (2009) reported that the cauda equina conduction time was signifi cantly prolonged in lumbar spinal stenosis. When the central canal area was less than 1.5 cm2, a delay of cauda equina conduction may occur. Demyelination was previously reported in the compressed cauda equina (Senocak et al., 2009). Feng et al. (2000) also reported that the cauda equina showed high signal on MRI, with normal axons by light microscope, but worm-eaten changes in the myelin sheath without evidence of changes in polyribosomes and rough endoplasmic reticulum by electron microscope in dogs with 25% canal stenosis at 12 weeks of recovery. In dogs with 50% canal stenosis, there was evidence of high signal on MRI, with varied axonal diameters, partial separation, and vacuolation by light microscope, and myelin degeneration, axonal atrophy, and metachromatic granules in Schwann cell membrane by electron microscope at 12 weeks of recovery. In dogs with 75% canal stenosis, there was evidence of high signal on MRI and disappearance of normal structures by light microscopy, and lamellar myelin disorders and axon loss by electron at 12 weeks of recovery. Taken together, compression leads to deterioration in the function and histology of the cauda equina.
Sensitivity of FA in detecting spinal degeneration
FA is an important indicator for describing the degree of anisotropy on DTI (Filler, 2009; Jambawalikar et al., 2010). An FA of zero represents isotropic diff usion, while an FA of 1 represents only linear diff usion. FA values in nerve fi bers of the human body range from 0.2–0.8 (Jambawalikar et al., 2010). In the present study, the mean normal FA value of the LSNR was 0.332 ± 0.074. Anatomically, from the L1to L5level, the average angle was 40° (range 37–41°) between the LSNR and the dural sac. At the S2level, the angle sharply reduces to 22 ± 4° on average, and tends to be smaller in the following spinal nerves in the sacral canal (Cohen et al., 1990).
Previous studies have used DTI for anatomical assessment of spinal nerves. For example, spinal nerve imaging by DWI could visualize anatomical structures from the separation of the LSNR to the dorsal ganglia. FA values of the spinal nerves were also signifi cantly lower after sciatic neuropathy compared with controls. Furthermore, FA values in the sciatic nerve were correlated with disability scores and electrophysiological parameters of axonal damage at baseline and at 6 months after the initial DTI scan (Mathys et al., 2013). The changes in FA values were strongly correlated with histological changes, including axon and myelin regeneration (Takagi et al., 2009; Morisaki et al., 2011), and indicated that axon membranes played a major role in anisotropic water diff usion and that myelination could modulate the degree of anisotropy (Takagi et al., 2009). In the present study, the FA value of the LSNR was lower in areas of lumbar stenosis, in which the LSNR is compressed over a long period with demyelination and axonal degeneration (Feng et al., 2000). These fi ndings are consistent with previous studies (Takagi et al., 2009; Morisaki et al., 2011; Mathys et al., 2013).
Signifi cance of tractography in assessing the changes in LSNR
Lumbosacral spine MRI clearly shows the structures of the spinal canal and characteristics of the spinal nerves on T1WI and T2WI. DWI can clearly visualize the shape of the spinal nerves and the nerve ganglia in maximum intensity projection mode (Zhang et al., 2009). In the present study, we used a group of DTI images in one direction for DWI to reduce the misregistration between DTI and DWI.
The axial scanning of the two-dimensional T2WI in our study matched that of DTI with respect to range, thickness, and orientation for comparison of the spinal structures. The separation points of the LSNR and the dorsal ganglia were visible on DWI. This allowed us to mark the slice position of the LSNR and apply it to the axial images of DTI for selecting the ‘seed’ and ‘target’ to reconstruct the LSNR. Our results confi rmed that the LSNR could be displayed clearly and symmetrically in normal volunteers from L3to S1on DTI. However, in patients with lumbosacral stenosis, LSNR had a varied appearance including thinning, distortion, and abruption. Asymmetry and distortion were the main morphological changes in LSNR.
Study limitations
This study compared LSNR between normal volunteers and lumbar stenosis patients using DTI. DTI has high potential for displaying the morphology and histology of the LSNR. However, image distortion can occur with DTI as a result of eddy currents, cerebrospinal fl uid motion, and physiological movement (Wang et al., 2011; Middleton et al., 2014). Simultaneously, the impact of the intervertebral discs shouldbe considered during reconstruction of the LSNR (Yang et al., 2007), while the presence of the cauda equina will aff ect observation of the LSNR (Hou et al., 2013). Indeed, the fi nding of abruption of the LSNR on tractography does not indicate disconnection of the spinal nerves, but rather loss on tractography tracing due to the lower FA (Eguchi et al., 2010). An indicator of the dural sac area may not fully refl ect the real severity of LSNR compression, as the degree of stenosis of the lateral recess plays a more important direct role, while the lateral recess on one side or both sides is diffi cult to evaluate quantitatively and repeatedly. Nevertheless, the dural sac area represents an aspect of the severity of compression in the cauda equina.
In clinical practice, after surgery the quality of DTI in reexamination is often diminished by the metal instrument fi xed on the vertebral pedicles. In addition, scanning with DTI is time-consuming when the scanning direction is perpendicular to the spinal canal. Furthermore, the tractography fi ndings did not totally match the changes in LSNR on T1WI and T2WI, with nearly 30% false negative results. The quality of tractography and spatial resolution of the images were based mainly on the skill and experience of the operator. Thus, to assure the quality of DTI, future studies are required to reduce the scan time and improve the reconstruction mode of tractography for assessment of LSNR.
Acknowledgments: We thank technician Shu-xin Li for his instruction and help in MRI scans in both volunteers and patients in the Department of Radiology of the Second Affiliated Hospital of Guangzhou Medical University in China.
Author contributions: ZJH, YH, ZWF and XCL participated in study design. ZJH, XCL and BYC did literature search. ZJH, YH and BYC performed experiments. ZJH, YH and ZWF collected data. ZJH and ZWF analyzed the data. ZJH wrote the paper. ZJH and XCL reviewed the paper. All authors approved the fi nal version of the paper.
Confl icts of interest: None declared.
Plagiarism check: This paper was screened twice using Cross-Check to verify originality before publication.
Peer review: This paper was double-blinded, stringently reviewed by international expert reviewers.
Arrigo RT, Kalanithi P, Boakye M (2011) Is cauda equina syndrome being treated within the recommended time frame? Neurosurgery 68:1520-1526.
Arslan M, Cömert A, Açar H, Özdemir M, Elhan A, Tekdemir İ, Tubbs S, Attar A, Uğur H (2011) Lumbosacral intrathecal nerve roots: an anatomical study. Acta Neurochir (Wien) 153:1435-1442.
Byun WM, Ahn SH, Ahn MW (2012) Value of 3D MR lumbosacral radiculography in the diagnosis of symptomatic chemical radiculitis. Am J Neuroradiol 33:529-534.
Cohen MS, Wall EJ, Brown RA, Rydevik B, Garfi n SR (1990) 1990 AcroMed Award in basic science. Cauda equina anatomy. II: Extrathecal nerve roots and dorsal root ganglia. Spine (Phila Pa 1976) 15:1248-1251.
Eguchi Y, Ohtori S, Orita S, Kamoda H, Arai G, Ishikawa T, Miyagi M, Inoue G, Suzuki M, Masuda Y, Andou H, Takaso M, Aoki Y, Toyone T, Watanabe A, Takahashi K (2011) Quantitative evaluation and visualization of lumbar foraminal nerve root entrapment by using diff usion tensor imaging: preliminary results. Am J Neuroradiol 32:1824-1829.
Eguchi Y, Ohtori S, Yamashita M, Yamauchi K, Suzuki M, Orita S, Kamoda H, Arai G, Ishikawa T, Miyagi M, Ochiai N, Kishida S, Masuda Y, Ochi S, Kikawa T, Takaso M, Aoki Y, Toyone T, Suzuki T, Takahashi K (2010) Clinical applications of diff usion magnetic resonance imaging of the lumbar foraminal nerve root entrapment. Eur Spine J 19:1874-1882.
Feng JG, Han YT, Wang F (2000) Comparative observation of MRI and histology of delayed graded compression of the dog cauda equina. Zhonghua Fangshe Xue Zazhi 34:208-211.
Filippi C, Andrews T, Gonyea J, Linnell G, Cauley K (2010) Magnetic resonance diff usion tensor imaging and tractography of the lower spinal cord: application to diastematomyelia and tethered cord. Eur Radiol 20:2194-2199.
Filler A (2009) Magnetic resonance neurography and diff usion tensor imaging: origins, history, and clinical impact of the fi rst 50,000 cases with an assessment of effi cacy and utility in a prospective 5000-patient study group. Neurosurgery 65:A29-43.
Hicks GE, Morone N, Weiner DK (2009) Degenerative lumbar disc and facet disease in older adults: prevalence and clinical correlates. Spine 34:1301-1306.
Hou ZJ, Huang Y, Fan ZW, Cao BY (2013) The research of diffusion tensor imaging of magnetic resonance imaging in normal cauda equina. Yixue Yingxiang Xue Zazhi 23:371-375.
Jambawalikar S, Baum J, Button T, Li H, Geronimo V, Gould E (2010) Diffusion tensor imaging of peripheral nerves. Skeletal Radiol 39:1073-1079.
Jang SH, Chang PH, Kim YK, Seo JP (2014) Anatomical location of the frontopontine fi bers in the internal capsule in the human brain: a diff usion tensor tractography study. Neuroreport 25:117-121.
Li X, Chen J, Hong G, Sun C, Wu X, Peng MJ, Zeng G (2013) In vivo DTI longitudinal measurements of acute sciatic nerve traction injury and the association with pathological and functional changes. Eur J Radiol 82:e707-e714.
Mathys C, Aissa J, Zu Hörste GM, Reichelt DC, Antoch G, Turowski B, Hartung HP, Sheikh KA, Lehmann HC (2013) Peripheral neuropathy: assessment of proximal nerve integrity by diff usion tensor imaging. Muscle Nerve 48:889-896.
Middleton DM, Mohamed FB, Barakat N, Hunter LN, Shellikeri S, Finsterbusch J, Faro SH, Shah P, Samdani AF, Mulcahey MJ (2014) An investigation of motion correction algorithms for pediatric spinal cord DTI in healthy subjects and patients with spinal cord injury. Magn Reson Imaging 32:433-439.
Morisaki S, Kawai Y, Umeda M, Nishi M, Oda R, Fujiwara H, Yamada K, Higuchi T, Tanaka C, Kawata M, Kubo T (2011) In vivo assessment of peripheral nerve regeneration by diff usion tensor imaging. J Magn Reson Imaging 33:535-542.
Quint U, Wilke HJ (2008) Grading of degenerative disk disease and functional impairment: imaging versus patho-anatomical fi ndings. Eur Spine J 17:1705-1713.
Saleem S, Aslam HM, Rehmani MAK, Raees A, Alvi AA, Ashraf J (2013) Lumbar disc degenerative disease: disc degeneration symptoms and magnetic resonance image fi ndings. Asian Spine J 7:322-334.
Senocak Ö, Hürel DM, Sener U, Ugurel B, Öztura I, Ertekin C (2009) Motor conduction time along the cauda equina in patients with lumbar spinal stenosis. Spine 34:1410-1414.
Takagi T, Nakamura M, Yamada M, Hikishima K, Momoshima S, Fujiyoshi K, Shibata S, Okano HJ, Toyama Y, Okano H (2009) Visualization of peripheral nerve degeneration and regeneration: monitoring with diff usion tensor tractography. Neuroimage 44:884-892.
Wang ZJ, Seo Y, Chia JM, Rollins NK (2011) A quality assurance protocol for diff usion tensor imaging using the head phantom from American College of Radiology. Med Phys 38:4415-4421.
Yang HT, Wang RF, Wang J, Gao XL, Li FT, Zhang HD, Xia LM, Wang CY (2007) Clinical application of MR diff usion tensor imaging in lumbar disc annulus fi brosis. Zhonghua Fangshe Xue Zazhi 41:1100-1103.
Zhang Z, Song L, Meng Q, Li Z, Pan B, Yang Z, Pei Z (2009) Morphological analysis in patients with sciatica: a magnetic resonance imaging study using three-dimensional high-resolution diff usion-weighted magnetic resonance neurography techniques. Spine (Phila Pa 1976) 34:E245-250.
Copyedited by Dean J, Raye W, Yu J, Qiu Y, Li CH, Song LP, Zhao M
*Correspondence to: Zhong-jun Hou, 13694208683@163.com.
orcid: 0000-0002-5916-7206 (Zhong-jun Hou)
10.4103/1673-5374.170317 http://www.nrronline.org/
Accepted: 2015-09-10
杂志排行

中国神经再生研究(英文版)的其它文章
- The role of the Rho/ROCK signaling pathway in inhibiting axonal regeneration in the central nervous system
- Targeting brain microvascular endothelial cells: a therapeutic approach to neuroprotection against stroke
- Severe bilateral anterior cingulum injury in patients with mild traumatic brain injury
- Injury of corticoreticular pathway and corticospinal tract caused by ventriculoperitoneal shunting
- Susceptibility weighted imaging in the evaluation of hemorrhagic dif use axonal injury
- Mechanical properties of nerve roots and rami radiculares isolated from fresh pig spinal cords