Injury of corticoreticular pathway and corticospinal tract caused by ventriculoperitoneal shunting
2015-02-07SungHoJang,JeongPyoSeo
IMAGING IN NEURAL REGENERATION
Injury of corticoreticular pathway and corticospinal tract caused by ventriculoperitoneal shunting
Ventriculoperitoneal shunting is a commonly used neurosurgical procedure for management of hydrocephalus (Jang et al., 2015). Various complications of ventriculoperitoneal shunting have been reported, including infection, hemorrhage, shunt malfunction, shunt displacement and brain swelling (Kwon and Jang, 2012, 2015). Although ventriculoperitoneal shunting can cause injury of adjacent neural tracts, little is known about injury of the neural tract by ventriculoperitoneal shunting (Kwon and Jang, 2013).
Diff usion tensor tractography (DTT), derived from diff usion tensor imaging (DTI), enables visualization and estimation of neural tracts in three dimensions (Gold et al., 2008). A previous study using DTT has reported on injury of neural tracts by invasive neurosurgical procedures such as extraventricular drainage or shunt operation (Kwon and Jang, 2013). However, it has not been clearly elucidated so far.
In the current study, using DTT, we attempted to demonstrate injury of the corticoreticular pathway (CRP) and corticospinal tact (CST) caused by ventriculoperitoneal shunting in a patient with normal pressure hydrocephalus.
A 70-year-old female patient who showed gait disturbance for 1 year and enlarged ventricles on the brain CT was diagnosed with normal pressure hydrocephalus at the department of neurosurgery of a university hospital. She underwent ventriculoperitoneal shunting approached through the right posterior parietal area in the brain. Brain CT and T2 weighted MRI after shunt operation revealed hemorrhage at the corona radiata around the passage of the ventriculoperitoneal shunt (Figure 1A, B). After the shunt operation, the patient developed the left hemiparesis and gait diffi culty as follows (based on Medical Research Council [MRC] and Functional Ambulation Category [FAC]) (Cunha et al., 2002; Paternostro-Sluga et al., 2008): The MRC score was used for evaluation of motor function: 0, no contraction; 1, palpable contraction but no visible movement; 2, movement without gravity; 3, movement against gravity; 4, movement against a resistance lower than the resistance overcome by the healthy side; and 5, movement against a resistance equal to the maximum resistance overcome by the healthy side (Paternostro-Sluga et al., 2008). The FAC was designed for examination of the levels of assistance required during a 15-m walk. Six categories are included in the FAC: 0 (non-ambulatory), 1 (needs continuous support from one person), 2 (needs intermittent support from one person), 3 (needs only supervision and verbal cues), 4 (help is required on stairs and uneven surfaces), and 5 (can walk independently anywhere) (Cunha et al., 2002). The patient provided signed, informed consent and our institutional review board approved the study protocol.
DTI was acquired at 1 month after the shunt operation using a six-channel head coil on a 1.5-T Philips Gyroscan Intera (Philips, Ltd, Best, The Netherlands) with single-shot echo-planar imaging. Imaging parameters were as follows: acquisition matrix = 96 × 96, repetition time = 10,398 ms, echo time = 72 ms, echo planar factor = 59 and b = 1,000 s/mm2, number of excitations = 1, slice gap = 0 mm and a slice thickness of 2.5 mm. Fiber tracking for the CRP and CST was performed using the fi ber assignment continuous tracking (FACT) algorithm implemented within the DTI task card software. The left CRP and CST showed intact integrities from the cerebral cortex to the medulla. By contrast, the right CRP showed discontinuation at the passage of the shunt of the right corona radiata and degeneration to the right midbrain. In addition, the anterior portion of the right CST also showed discontinuation at the passage of the shunt of the right corona radiata compared with the left CST (Figure 1C).
In the current study, using DTT, we demonstrated injury of the CRP and CST following ventriculoperitoneal shunting in a patient with normal pressure hydrocephalus. Injury of the right CRP and CST in this patient appeared to have resulted from ventriculoperitoneal shunting or ventriculoperitoneal shunting combined with hematoma caused by ventriculoperitoneal shunt operation. We think that the motor weakness of the left upper and lower extremities in this patient was ascribed to injury of the CRP and CST. Furthermore, the characteristics of the motor weakness were compatible with the injury of these motor tracts: more severe weakness of the left proximal joint muscle than the left distal joint muscles, indicating the injury of the right CRP, and milder weakness of the left distal joint muscles than the left proximal joint muscles, indicating the partial injury of the right CST (Jang et al., 2015).
Although many studies have reported on the complications of invasive procedures such as extraventricular drainage or shunt operation, injuries of neural tracts in the brain caused by these procedures have rarely been reported (Gold et al., 2008; Kwon and Jang, 2012, 2013, 2015). The injured neural tracts were as follows: CST, cingulum, fornix, and CRP. Regarding the CRP and CST, Gold et al. (2008) reported on a patient who presented with direct injury of the CST during revision of a ventriculoperitoneal shunt. Kwon and Jang (2015) reported on patients with intracerebral hemorrhage who showed injury of the CRP following external ventricular drainage (Gold et al., 2008; Kwon and Jang, 2015). As a result, to the best of our knowledge, this is the fi rst study to demonstrate combined injury of the CRP and CST following ventriculoperitoneal shunting.
This work was supported by the National Research Foundation (NRF) of Korea funded by the Korean Government (MSIP), No. 2015R1A2A2A01004073. SHJ conceived and designed this study, was responsible for fundraising, data acquisition, and paper development and writing. JPS was responsible for data acquisition, paper development, writing, and authorization. Both of these two authors approved the fi nal version of this paper.
Sung Ho Jang, Jeong Pyo Seo*
Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, Daegu, Republic of Korea
*Correspondence to: Jeong Pyo Seo, M.S., raphael0905@hanmail.net.
Accepted: 2015-09-02
orcid: 0000-0002-2695-7957 (Jeong Pyo Seo)
Cunha IT, Lim PA, Henson H, Monga T, Qureshy H, Protas EJ (2002) Performance-based gait tests for acute stroke patients. Am J Phys Med Rehabil 81:848-856.
Gold MM, Shifteh K, Valdberg S, Lombard J, Lipton ML (2008) Brain injury due to ventricular shunt placement delineated by diff usion tensor imaging (DTI) tractography. Neurologist 14:252-254.
Jang SH, Choi BY, Kim SH, Chang CH, Jung YJ, Yeo SS (2015) Injury of the corticoreticular pathway in subarachnoid haemorrhage after rupture of a cerebral artery aneurysm. J Rehabil Med 47:133-137.
Kwon HG, Jang SH (2012) Cingulum injury by ventriculoperitoneal shunt. Eur Neurol 67:63-64.
Kwon HG, Jang SH (2013) Cingulum injury by external ventricular drainage procedure: diff usion tensor tractography study. Clin Neuroradiol 25:65-67.
Kwon YM, Jang SH (2015) Neural injury by frontal approach of external ventricular drainage in stroke patients. Int J Neurosci doi:10.3109/00207454.2 015.1012665.
Paternostro-Sluga T, Grim-Stieger M, Posch M, et al (2008) Reliability and validity of the Medical Research Council (MRC) scale and a modifi ed scale for testing muscle strength in patients with radial palsy. J Rehabil Med 40:665-671.
Copyedited by Feling RJ, de Oliveira FF, Li CH, Song LP, Zhao M
10.4103/1673-5374.170320 http://www.nrronline.org/
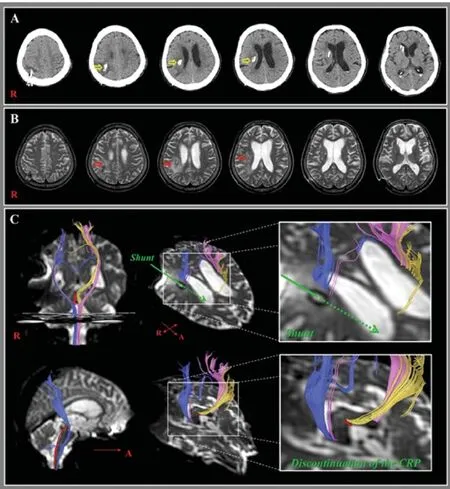
Figure 1 CT, T2 weighted MRI and diff usion tensor tractography (DTT) images of a 70-year-old female patient undergoing ventriculoperitoneal (VP) shunting approached through the right posterior parietal area in the brain.
(A) Brain CT images taken after shunt operation reveal hemorrhage at the corona radiata (yellow arrows) around the passage of the ventriculoperitoneal shunt. (B) T2-weighted MR images taken at 1 month after the shunt operation show a leukomalactic lesion in the right corona radiata (red arrows). (C) DTT images for the corticoreticular pathway (CRP) and corticospinal tact (CST) were acquired at 1 month after the shunt operation. The right CRP showed discontinuation at the passage of the shunt of the right corona radiata and degeneration to the right midbrain, and the anterior portion of the right CST also showed discontinuation at the right corona radiata (red color: right CRP; yellow color: left CRP; blue color: right CST; pink color: left CST). R: Right; A: anterior.
Jang SH, Seo JP (2015) Injury of corticoreticular pathway and corticospinal tract caused by ventriculoperitoneal shunting. Neural Regen Res 10(11):1874-1875.
杂志排行

中国神经再生研究(英文版)的其它文章
- The role of the Rho/ROCK signaling pathway in inhibiting axonal regeneration in the central nervous system
- Targeting brain microvascular endothelial cells: a therapeutic approach to neuroprotection against stroke
- Severe bilateral anterior cingulum injury in patients with mild traumatic brain injury
- Susceptibility weighted imaging in the evaluation of hemorrhagic dif use axonal injury
- Mechanical properties of nerve roots and rami radiculares isolated from fresh pig spinal cords
- Endogenous neurotrophin-3 promotes neuronal sprouting from dorsal root ganglia