Single injection of platelet-rich plasma as a novel treatment of carpal tunnel syndrome
2015-02-07MichaelAlexanderMalahiasElizabethJohnsonGeorgeBabisVasileiosNikolaou
Michael Alexander Malahias¹, Elizabeth O. Johnson², George C. Babis¹, Vasileios S. Nikolaou
1 Second Department of Orthopedics, Athens University, Athens, Greece
2 Department of Anatomy, School of Medicine, Athens University, Athens, Greece
Single injection of platelet-rich plasma as a novel treatment of carpal tunnel syndrome
Michael Alexander Malahias¹, Elizabeth O. Johnson², George C. Babis¹, Vasileios S. Nikolaou¹,*
1 Second Department of Orthopedics, Athens University, Athens, Greece
2 Department of Anatomy, School of Medicine, Athens University, Athens, Greece
Both in vitro and in vivo experiments have conf rmed that platelet-rich plasma has therapeutic ef ects on many neuropathies, but its ef ects on carpal tunnel syndrome remain poorly understood. We aimed to investigate whether single injection of platelet-rich plasma can improve the clinical symptoms of carpal tunnel syndrome. Fourteen patients presenting with median nerve injury who had suf ered from mild carpal tunnel syndrome for over 3 months were included in this study. Under ultrasound guidance, 1–2 mL of platelet-rich plasma was injected into the region around the median nerve at the proximal edge of the carpal tunnel. At 1 month after single injection of platelet-rich plasma, Visual Analogue Scale results showed that pain almost disappeared in eight patients and it was obviously alleviated in three patients. Simultaneously, the disabilities of the arm, shoulder and hand questionnaire showed that upper limb function was obviously improved. In addition, no ultrasonographic manifestation of the carpal tunnel syndrome was found in f ve patients during ultrasonographic measurement of the width of the median nerve. During 3-month follow-up, the pain was not greatly alleviated in three patients. These f ndings show very encouraging mid-term outcomes regarding use of platelet-rich plasma for the treatment of carpal tunnel syndrome.
nerve regeneration; carpal tunnel syndrome; platelet-rich plasma; ultrasound guidance; pilot study; neural regeneration
Malahias MA, Johnson EO, Babis GC, Nikolaou VS (2015) Single injection of platelet-rich plasma as a novel treatment of carpal tunnel syndrome. Neural Regen Res 10(11):1856-1859.
Introduction
Carpal tunnel syndrome (CTS) can be treated by both conservative (Klauser et al., 2009) and surgical interventions. Surgical decompression of the median nerve through the incision of the transverse carpal ligament (either open or mini-open or under ultrasound guidance) is the most cost-ef ective therapeutic option (Hui et al., 2005). However, mild to moderate CTS can be treated by conservative interventions, like functional braces and local inf ltrations (Prime et al., 2010) in the carpal tunnel, mainly with corticosteroids. Local inf ltration of corticosteroids easily leads to atrophy of the median nerve, subcutaneous fat, and systematic complications, such as hair loss and Cushing syndrome (Lambru et al., 2012). This treatment option is clearly inferior to surgical intervention despite the fact that it can improve clinical condition. There is evidence that local inf ltration of corticosteroids is not superior to local injection of anesthetic (Karadas et al., 2012). To the best of our knowledgement, use of corticosteroids in the clinical practice has not been studied. However, a surgical treatment decision is always taken by the patient who sometimes wants to delay or avoid the surgery because of psychological or medical concerns including allergy to local anesthetic and immune def ciency and prefers a conservative treatment in the initial stage. A conservative treatment has been considered insuf cient for CTS. In vitro and in vivo clinical and laboratory studies (Allampallam et al., 2000; Farrag et al., 2007; Cho et al., 2010; Anjayani et al., 2014; Park and Kwon, 2014) have demonstrated that platelet-rich plasma (PRP) has therapeutic action in several neuropathies. It would be interesting if a PPP injection is used as an alternative conservative treatment of CTS. The purpose of this study was to investigate if, and to what extent, a PPP injection, under ultrasound guidance, can improve the clinical condition of patients with CTS.
Materials and Methods
Fourteen patients were selected from initial 32 patients who received treatment in the Department of Orthopedics of“Konstantopouleio” General Hospital, Greece because of mild to moderate CTS, with a minimum of 3-month duration of symptoms, regardless of age and gender. Patients were rejected if they had one of the following items: thrombopenia, platelet dysfunction, local infection, NSAID use (less than 48 hours prior to injury), recent illness, malignancy, hemoglobin (Hb) level < 100 g/L, pregnancy, rheumatologic disease, uncontrolled hormonal disorder, vibrating caused neuropathy, systematic inf ammatory disease, polyneuropathy, inability to complete questionnaires (due to language unawareness or mental disability), addicted to alcohol or drugs, total loss of sensation in the f ngers, prior corticosteroid injection in the same wrist, had undergone a surgical intervention for CTS in the same hand, neurological def cit,cervical radiculopathy and/or cervical spinal stenosis and/or intervertebral disc herniation, nerve entrapment syndrome in the same hand.
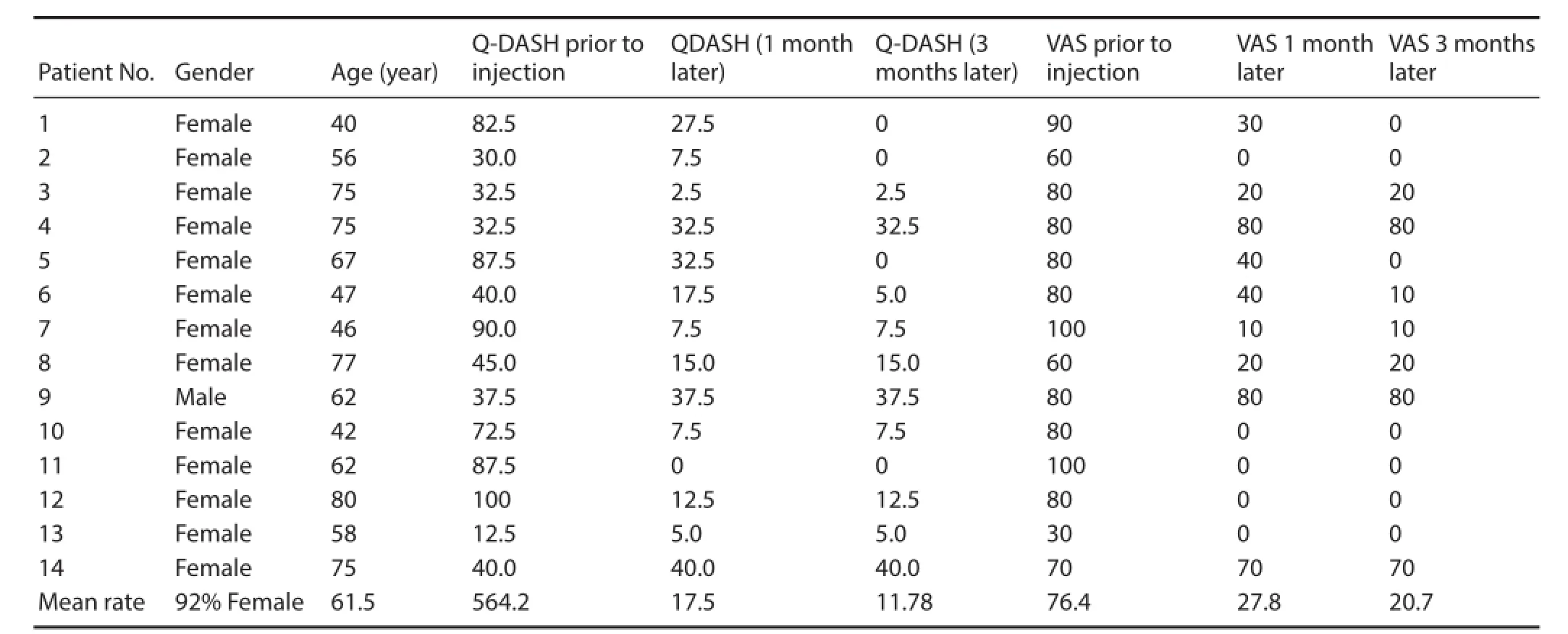
Table 1 General data and outcome measures of patients
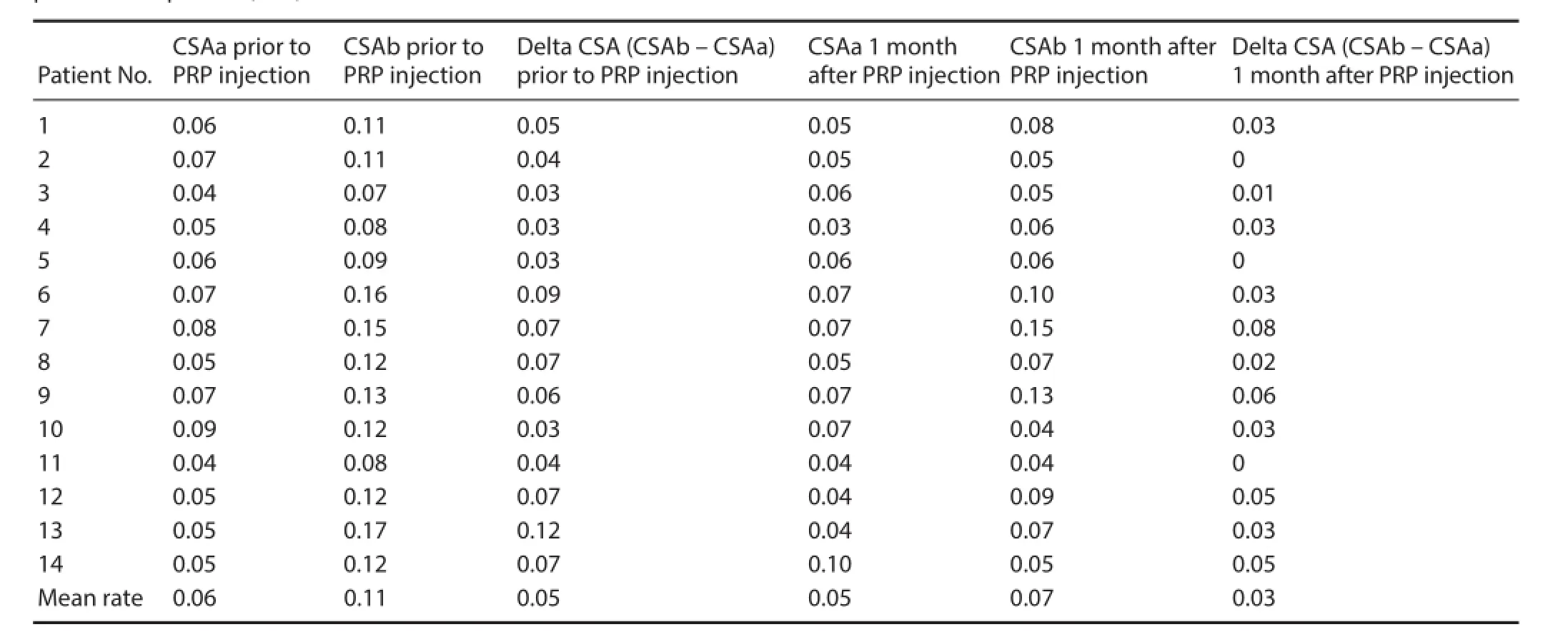
Table 2 Sonographic measurement of the cross sectional areas (CSA, cm²) of the median nerve and the delta CSA prior to and 1 month after platelet-rich plasma (PRP) inf ltration
From the initial 32 patients, three patients who had concomitant pain that derived from cervical spine disorder, one patient who showed other nerve compression unilaterally, one patient with thrombopenia, two patients with rheumatic diseases, two patients with uncontrolled hormonal disorder, and one pregnant patient were excluded. In addition, two patients who had received local inf ltration of corticosteroids and one patient who failed in surgical intervention for CTS were also excluded (Figure 1).
The remaining 19 patients were examined clinically using Phalen and Tinnel tests (Bozek and Gazdzik, 2001) and underwent diagnostic ultrasonography for measurement of the width of the median nerve (delta CSA, as the dif erence –delta-between the cross sectional areas – CSA-proximal to the carpal tunnel and at the tunnel inlet) and electromyogram.
The ultrasonography was performed with a portable gray scale ultrasound machine (frequency of 10–12 MHz, A6 Portable Ultrasonic Diagnostic System, Sonoscape Company Limited, Shenzhen, China). The patients were informed with an oral and written manner for their options of treatment and they received clear explanations about the treatment with PRP that was recommended as an alternative to surgery.
For conf rmation, they signed full written consent. Thus, 14 out of 19 patients who chose treatment with PRP instead of surgical intervention were included in this study. Our study protocol with written informed consent was approved by the Scientif c Committee, Health Institution, School of) Medicine, Athens University, Greece. Venous blood samples were obtained from subjects according to the World Medical Association outlined in the Declaration of Helsinki.
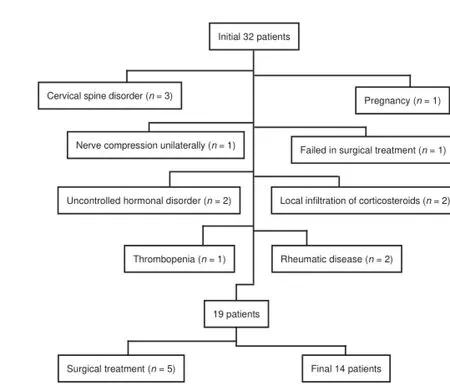
Figure 1 Flow chart of patient selection.
The severity of patient’s clinical symptoms was estimated using the disabilities of the arm, shoulder and hand (DASH) questionnaire (Q-DASH; Greenslade et al., 2004) and visual analogue scale (VAS) score (0–100 mm; Karadag et al., 2010) before inf ltration. Under sterile condition, 20 mL of autologous venous blood sample was taken from each patient’s contralateral (non-af ected) hand and then centrifuged at two consecutive density gradient centrifugations (total 3,100 runs for 10 minutes) at the laboratory of our hospital. At the f rst centrifugation, red blood cells were separated, and at the second centrifugation, PRP was separated from the platelet poor plasma (PPP) and then transferred to sterile tubes. The inf ltration was done under sterile conditions (skin sterilization, ultrasound probe covered with sterile pad, use of appropriate gel) by a physician who simultaneously managed the ultrasound device (free hand one-man technique: a single doctor holds the syringe with one hand while he scans by moving the probe with the other hand). Under continuous imaging of the tip of the needle, the syringe was put around the median nerve at the proximal edge of the carpal tunnel (ulnar insertion of the needle (Smith et al., 2008)) where the inf ltration of PRP (1–2 mL) was performed (Figure 2A).
The patients were encouraged to return to their daily activities immediately. Short-term outcomes were estimated and the width of the median nerve at its entry at the carpal tunnel measured by the ultrasound was compared between before and after inf ltration of PRP. Short- (4 weeks) and mid-term (12 weeks) outcomes were estimated using Q-DASH and the pain scale VAS. One physician (resident) did the procedure in all patients and evaluated them prior to the PRP injection using VAS and Q-DASH. Another physician (consultant) performed the ultrasonographic evaluation by measuring the dif erence –delta CSA in cross sectional areas of the median nerve (Klauser et al., 2009) before and after PRP injection in all patients. A third physician (another resident) evaluated the patients during the follow-up period (VAS, Q-DASH). This physician was blinded to the procedure (PRP injection) and to the pre-injection scores of these patients. Instructions for return to work (or usual activities in elderly people) were identical in all patients.
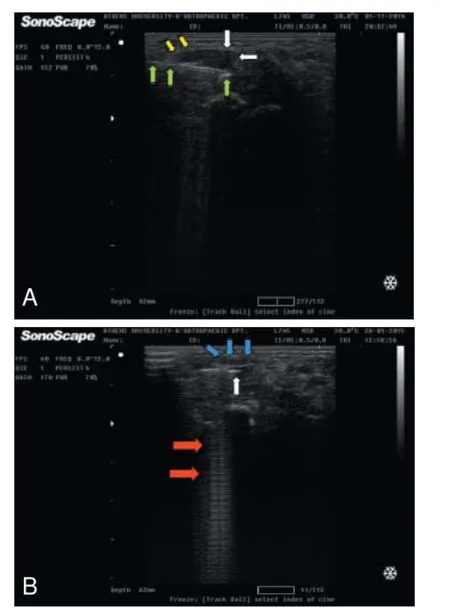
Figure 2 Ultrasound-guided injection of PRP.
Results
PRP injection proved to be well tolerated, with no side effects, infections or complaints for persistent pain. We achieved well def ned ultrasonographic mobilization, hydrodissection and hydrodisolution (Figure 2B) of the compressed median nerve through PRP simple injection.
At the end of the f rst month after PRP injection, the mean reduction in VAS (%) was 48.6 mm out of 100 mm in comparison to rates prior to injection. At that time, we found eight patients with full or almost full recovery (VAS: 0 – 20 mm) and three patients with great improvement (VAS decline: more than 30 mm). The mean decline of the Q-DASH score was calculated just a little less than 70% compared to the pre-injection rates (from mean Q-DASH 56.42 prior to injection to mean Q-DASH17.5 one month after). These rates slightly more improved 3 months later (Table 1).
At 1 month after PRP injection, we performed a new ultrasound measurement of delta CSA of the median nerve and found no ultrasonographic f ndings of the CTS in f ve patients (delta CSA: 0–0.02 cm²). We also found that delta CSA or CSAb was reduced in f ve patients; delta CSA was not changed after injection in three patients compared to prior to injection; delta CSA was increased after injection in one patient (Table 2). At 3 months of follow-up period, poor or fair improvement was found in three patients (VAS decline less than 30 mm) and an open operation for CTS was performed.
Discussion
One double-blind randomized controlled clinical trial was reported on perineural administration of PRP in 60 patients with Hansen’s disease (Anjayani et al., 2014), and positive outcomes of sensory symptoms were obtained. In another in vitro study, the ef ects of four growth factors on the transformation of cells from the impaired transverse ligament were investigated in patients with CTS using microscopy (Allampallam et al., 2000).
Three animal experimental studies also conf rmed that neural tissue regeneration is attributable to PRP inf ltration (Allampallam et al., 2000; Farrag et al., 2007; Cho et al., 2010; Anjayani et al., 2014; Park and Kwon, 2014). Of note, the f rst two studies were about regeneration of the facial nerve (the former in rats, and the latter in new guinea pigs), the last and more recent study referred to an artificially made model of CTS (Yoshii et al., 2011) at the median nerve of rabbits by inf ltration of 10% dextrose (Park and Kwon, 2014). Our results showed that PRP protected patients with CTS. To the best of our knowledge, this is the f rst published clinical study regarding PRP injection in patients with CTS.
A limitation of our study is the small number of patients, because this is a pilot study. This choice is deliberate and was done for ethical reasons, despite the fact that there are in vitro and in vivo data from animal or laboratory studies that are in favor of our hypothesis. We deal with a rather not extensively investigated f eld of clinical application (Malahias et al., 2014) that would not ethically justify the direct planning and performance of a study with many patients.
To conclude, our study showed very encouraging midterm results (12 weeks) regarding use of PRP for treatment of CTS. Based on our results, we recommend the planning and performance of a randomized double-blind controlled clinical trial to conf rm the possible favorable use of PRP in patients with mild to moderate CTS.
Acknowledgments: We wish to thank the personnel of the Hematology Department of “Konstantopouleio” General Hospital, Greece for their contributions to the laboratory part of our study.
Author contributions: MAM conducted this survey and wrote the paper. He also performed the single ultrasound-guided injection in all patients and evaluated them prior to injection using VAS and Q-DASH. VSN was in charge of ultrasonographic evaluation before and after the injection in all patients and revised the paper. EOJ retrieved the literature and evaluated the
patients using VAS and Q-DASH. GCB supervised the whole study. All authors approved the f nal version of this paper. Conf icts of interest: None declared.
Plagiarism check: This paper was screened twice using Cross-Check to verify originality before publication.
Peer review: This paper was double-blinded, stringently reviewed by international expert reviewers.
Allampallam K, Chakraborty J, Robinson J (2000) Effect of ascorbic acid and growth factors on collagen metabolism of f exor retinaculum cells from individuals with and without carpal tunnel syndrome. J Occup Environ Med 42:251-259.
Anjayani S, Wirohadidjojo YW, Adam AM, Suwandi D, Seweng A, Amiruddin MD (2014) Sensory improvement of leprosy peripheral neuropathy in patients treated with perineural injection of platelet-rich plasma. Int J Dermatol 53:109-113.
Bozek M, Gazdzik TS (2001) The value of clinical examination in the diagnosis of carpal tunnel syndrome. Ortop Traumatol Rehabil 3:357-360.
Cho HH, Jang S, Lee SC, Jeong HS, Park JS, Han JY, Lee KH, Cho YB (2010) Ef ect of neural-induced mesenchymal stem cells and platelet-rich plasma on facial nerve regeneration in an acute nerve injury model. Laryngoscope 120:907-913.
Farrag TY, Lehar M, Verhaegen P, Carson KA, Byrne PJ (2007) Ef ect of platelet rich plasma and f brin sealant on facial nerve regeneration in a rat model. Laryngoscope 117:157-165.
Greenslade JR, Mehta RL, Belward P, Warwick DJ (2004) Dash and Boston questionnaire assessment of carpal tunnel syndrome outcome: what is the responsiveness of an outcome questionnaire? J Hand Surg Br 29:159-164.
Hui AC, Wong S, Leung CH, Tong P, Mok V, Poon D, Li-Tsang CW, Wong LK, Boet R (2005) A randomized controlled trial of surgery vs steroid injection for carpal tunnel syndrome. Neurology 64:2074-2078.
Karadag YS, Karadag O, Cicekli E, Ozturk S, Kiraz S, Ozbakir S, Filippucci E, Grassi W (2010) Severity of carpal tunnel syndrome assessed with high frequency ultrasonography. Rheumatol Int 30:761-765.
Karadas O, Tok F, Akarsu S, Tekin L, Balaban B (2012) Triamcinolone acetonide vs procaine hydrochloride injection in the management of carpal tunnel syndrome: randomized placebo-controlled study. J Rehabil Med 44:601-604.
Klauser AS, Halpern EJ, De Zordo T, Feuchtner GM, Arora R, Gruber J, Martinoli C, Loscher WN (2009) Carpal tunnel syndrome assessment with US: value of additional cross-sectional area measurements of the median nerve in patients versus healthy volunteers. Radiology 250:171-177.
Lambru G, Lagrata S, Matharu MS (2012) Cutaneous atrophy and alopecia after greater occipital nerve injection using triamcinolone. Headache 52:1596-1599.
Malahias MA, Chytas D, Babis GC, Nikolaou VS (2014) Platelet-rich plasma guided injections: clinical application in peripheral neuropathies. Front Surg 1:41.
Park GY, Kwon DR (2014) Platelet-rich plasma limits the nerve injury caused by 10% dextrose in the rabbit median nerve. Muscle Nerve 49:56-60.
Prime MS, Palmer J, Khan WS, Goddard NJ (2010) Is there light at the end of the tunnel? controversies in the diagnosis and management of carpal tunnel syndrome. Hand 5:354-360.
Smith J, Wisniewski SJ, Finnof JT, Payne JM (2008) Sonographically guided carpal tunnel injections: the ulnar approach. J Ultrasound Med 27:1485-1490.
Yoshii Y, Zhao C, Schmelzer JD, Low PA, An KN, Amadio PC (2011) Ef ects of hypertonic dextrose injections in the rabbit carpal tunnel. J Orthop Res 29:1022-1027.
Copyedited by Vanni D, Li CH, Song LP, Zhao M
*Correspondence to: Vasileios S. Nikolaou, M.D., Ph.D., vassilios.nikolaou@gmail.com.
orcid: 0000-0001-7422-4195 (Vasileios S. Nikolaou)
10.4103/1673-5374.165322 http://www.nrronline.org/
Accepted: 2015-07-27
杂志排行

中国神经再生研究(英文版)的其它文章
- Intracellular sorting pathways of the amyloid precursor protein provide novel neuroprotective strategies
- The role of the Rho/ROCK signaling pathway in inhibiting axonal regeneration in the central nervous system
- VEGF in the nervous system: an important target for research in neurodevelopmental and regenerative medicine
- Studying neurological disorders using induced pluripotent stem cells and optogenetics
- Ef cacy of glucagon-like peptide-1 mimetics for neural regeneration
- Compliant semiconductor scaf olds: building blocks for advanced neural interfaces