Expression of prothymosin α predicts early recurrence and poor prognosis of hepatocellular carcinoma
2015-02-06
Seoul, Korea
Expression of prothymosin α predicts early recurrence and poor prognosis of hepatocellular carcinoma
Sang Yun Ha, Dae Hyun Song, Soo Hyun Hwang, Soo Youn Cho and Cheol-Keun Park
Seoul, Korea
BACKGROUND: Prothymosin α (PTMA) is a nuclear oncoprotein-transcription factor essential for cell cycle progression and proliferation. PTMA was overexpressed in several human malignancies including hepatocellular carcinoma (HCC). However, the prognostic signifcance of PTMA protein expression in HCC remains unclear. In the present study, we evaluated PTMA protein expression by immunohistochemistry in order to elucidate the prognostic roles of PTMA in HCC patients.
METHODS: By immunohistochemistry, we investigated the expression of PTMA protein in tumor tissue from 226 HCC patients who underwent curative hepatectomy. Univariate and multivariate analyses were performed to evaluate its predictive value for tumor recurrence and survival of patients. The median follow-up period was 120 months.
RESULTS: PTMA expression was observed in 162 (71.7%) of the 226 HCC patients and was signifcantly associated with higher Edmondson grade, microvascular invasion, intrahepatic metastasis, higher American Joint Committee on Cancer (AJCC) T-stage, and lower albumin level. PTMA expression was an independent predictor of early recurrence (P=0.001). PTMA expression showed an unfavorable infuence on recurrencefree survival (RFS) (P<0.001). Subgroup analysis showed that among patients with tumor size ≤5.0 cm (140 patients), patients at AJCC T-stage 1 (95 patients) and patients with α-fetoprotein≤ 20 ng/ mL (83 patients), the differences in RFS between PTMA-positive and PTMA-negative groups were also statistically signifcant (P=0.017,P=0.002 andP=0.002, respectively). In addition, PTMA expression was an independent predictor of shorter RFS (P=0.011). PTMA expression showed an unfavorable infuence on overall survival (P=0.014), but was not an independentpredictor of shorter overall survival (P=0.161).
CONCLUSIONS: PTMA protein expression might be a novel predictor of early recurrence and RFS in HCC patients, even those at early stage or with α-fetoprotein-negative after curative hepatectomy. PTMA could be used as an immunohistochemical biomarker to detect patients with a high risk of recurrence.
(Hepatobiliary Pancreat Dis Int 2015;14:171-177)
prothymosin α; hepatocellular carcinoma; recurrence
Introduction
Hepatocellular carcinoma (HCC) has a poor prognosis and surgical resection improves the survival rates for patients. However, the prognosis after surgical resection of HCC remains grave because of a high rate of recurrence.[1,2]It is critical to determine which individual patients need more effective and targeted therapy in order to prevent tumor recurrence after surgical resection. Although there are many reports on histologic parameters for predicting HCC prognosis, molecular markers for HCC recurrence and prognosis could provide additional information.[3]
Prothymosin α (PTMA) is an extremely abundant nuclear oncoprotein-transcription factor essential for cell cycle progression and proliferation.[4]A recent study[5]has identifed PTMA as an inhibitor of apoptosome formation, the essential step for the apoptotic pathway. PTMA was overexpressed in several human malignancies such as breast cancer, lung cancer, neuroblastoma, gastric cancer, bladder cancer, and upper urinary tract transitional cell carcinoma.[6-11]And PTMA also served as a prognostic marker for cancers of the breast, lung, prostate, bladder and stomach.[6,7,9,12,13]Wu et al[14]reported that PTMA mRNA levels were two- to 9.2-fold higher in HCC tissues than those in adjacent non-tumoral tissues in 14 of 17 patients with HCC, andin situhybridizationrevealed increased PTMA mRNA localized in the HCC tissues. No difference in PTMA mRNA levels was present in 4 patients with hepatic adenoma.[14]However, the prognostic signifcance of PTMA protein expression in HCC remains unclear. In the present study, we evaluated PTMA protein expression by immunohistochemistry in order to elucidate the prognostic roles of PTMA in 226 HCC patients with a long-term follow-up and extensive information on clinicopathologic characteristics.
Methods
Patients and tissue samples
HCC tissues from the 226 patients who had been treated with curative hepatectomy from July 2000 to May 2006 at Samsung Medical Center, Seoul, Korea were analyzed in this study. We defned curative resection as complete resection of all tumor nodules with clear microscopic resection margins and no residual tumors as indicated by a computed tomography scan one month after surgery. The diagnosis was confrmed histologically in all patients. The Institutional Review Board of Samsung Medical Center approved the study. In this series, there were 184 men and 42 women, aged on average 52.2 years (range 17-76). Chronic hepatitis B virus infection was detected in 174 (77.0%) patients and chronic hepatitis C virus infection in 22 (9.7%). No viral marker was recognized in 30 (13.3%) patients. None of the patients had received preoperative chemotherapy. Tumor differentiation was graded histologically according to the criteria of Edmondson and Steiner.[15]Microvascular invasion was defned when at least one or more endothelial cells or the tunica media of the vessel surrounded a neoplastic cell group. Intrahepatic metastasis and multicentric occurrence were defned according to the previously reported criteria.[16]Tumor stage was determined according to both the American Joint Committee on Cancer (AJCC) staging system[17]and Barcelona Clinic Liver Cancer (BCLC) staging classifcation.[18]HCC recurrence within the frst two years after surgery is mainly due to intrahepatic metastasis, but late recurrence usually results from multicentric occurrence.[19]Using 2 years as the cutoff, tumor recurrence was classifed as either early recurrence or late recurrence.[20]
Patients after curative hepatectomy were followed by monitoring serum α-fetoprotein levels and three phase dynamic computed tomography scans every 3 months after surgery. Magnetic resonance imaging was used to confrm tumor recurrence in suspected cases. The follow-up period for recurrence was at least 24 months and the median follow-up period for overall survival (OS) was 120 months (range 14.0-151.4). Recurrence-free survival (RFS) was defned from the date of resection until the detection of tumor recurrence. Tumor relapse was detected in 165 patients (73.0%), and 91 patients (40.3%) died of HCC. Seventeen of the 108 deaths in this study were due to non-HCC causes. Ten of the 17 deaths were due to hepatic failure, fve due to non-hepatic causes, and two due to unknown causes.
Histologic sections were examined by two pathologists and representative tumor regions free from necrosis or hemorrhage were marked in formalin-fxed paraffn-embedded blocks. Two tissue cores with a diameter of 2.0 mm were punched from the marked areas of each block and arranged in recipient paraffn blocks. As controls, two cores of normal liver tissue from 12 patients with metastatic colonic carcinoma of the liver were included in each array block.
Immunohistochemical analysis
Immunohistochemical staining was performed as previously described.[21]Antigen retrieval was performed with 0.01 mol/L citrate buffer (pH 6.0) for 30 minutes in a pressure cooker. The sections were incubated for 30 minutes at room temperature with mouse monoclonal antibody to PTMA (LS-B2322, 1:200; LifeSpan Biosciences Inc., Seattle, WA, USA). No immunoreactivity was observed in tissue sections used as negative control where the primary antibody was replaced by isotype-matched irrelevant antibody. To validate the concordance between tissue microarrays and whole tumor sections, we further detected PTMA expression for 40 corresponding whole tumor sections randomly chosen from the 226 patients.
All sections were scored by two independent pathologists (Ha SY and Park CK) who did not know patient characteristics, and any discrepancies were resolved by consensus. A nearly homogeneous immunostaining with moderate staining intensity was observed. The proportion of stained tumor cells was determined semi-quantitatively and each sample was scored on a scale of 0-4 (0,<1%; 1, 1%-25%; 2, 26%-50%; 3, 51%-75%; 4, >75%). Duplicate tissue cores for each tumor showed high levels of homogeneity for proportion of stained cells. In cases of differences between duplicate tissue cores, the higher score was taken.
Statistical analysis
Statistical analyses were performed using IBM SPSS version 18 software (IBM, Armonk, NY, USA). The correlation between PTMA expression and clinicopathologic features was examined by the Chi-square test and Fisher's exact test. Univariate and multivariate analyses for factors of tumor recurrence were performed using the logistic regression model. Cumulative survivalrates were calculated by the Kaplan-Meier method and compared by means of the log-rank test. Univariate and multivariate analyses of survival were performed using the Cox proportional hazards regression model. The signifcant variables in univariate analysis were introduced into multivariate analysis.Pvalues <0.05 were considered statistically signifcant.
Results
PTMA protein expression in HCC
In HCC, immunoreactivity for PTMA was observed only in the nuclei of tumor cells with moderate staining intensity. No immunoreactivity was found in normal hepatocytes. We regarded the PTMA as positive when≥1% of tumor cells showed nuclear immunoreactivity. PTMA protein expression was observed in 162 (71.7%) of the 226 HCC patients (Fig. 1). PTMA expression was signifcantly associated with higher Edmondson grade (P=0.017), microvascular invasion (P=0.014), intrahepat-ic metastasis (P=0.015), higher AJCC T-stage (P=0.006), and lower albumin level (P=0.034). PTMA expression was correlated with the early recurrence (P<0.001), but not with the late relapse (P=0.952) (Table 1).
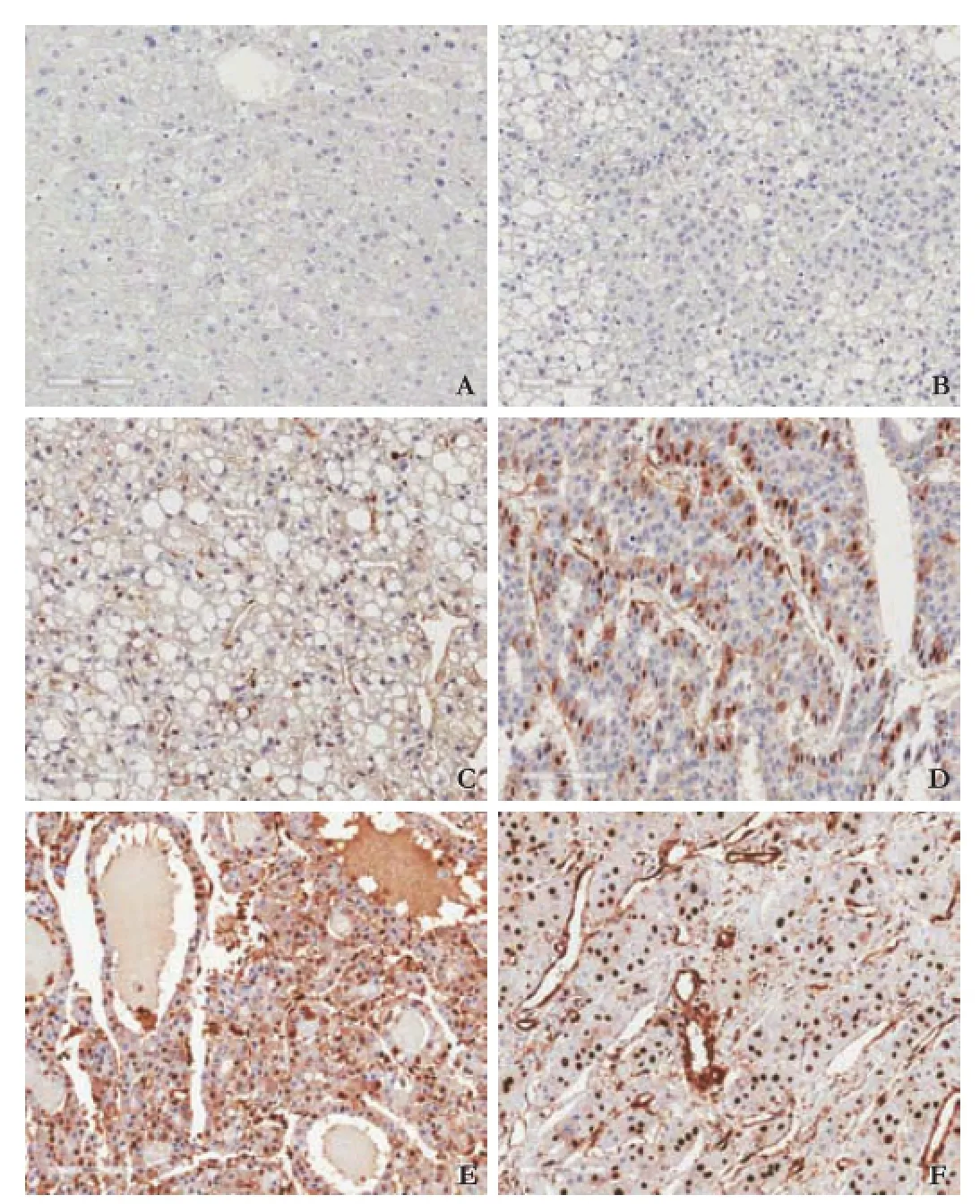
Fig. 1.Immunostaining of PTMA in normal liver and HCC. No immunoreactivity in normal liver (A) and representative images of areas showing nuclear immunoreactivity according to the proportion of positive tumor cells (B-F). (B) <1%, (C) 1%-25%, (D) 26%-50%, (E) 51%-75%, (F) >75% (horseradish peroxidase stain, original magnifcation ×200).
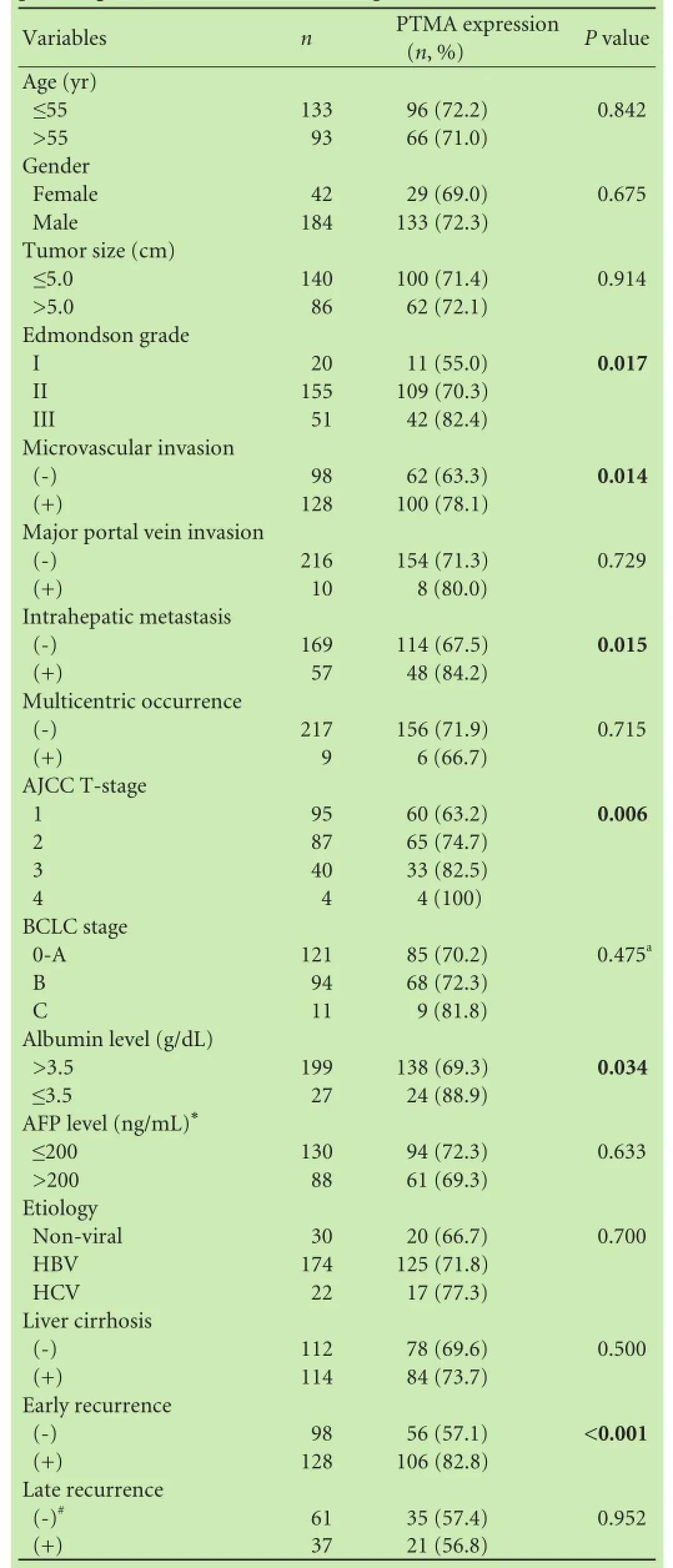
Table 1.Correlation between PTMA expression and the clinicopathologic features in the 226 HCC patients
Prediction of early recurrence in HCC
In univariate analyses, early recurrence was signifcantly associated with larger tumor size (P=0.002), microvascular invasion (P<0.001), intrahepatic metastasis (P<0.001), higher AJCC T-stage (P<0.001), higher BCLC stage (P<0.001), viral etiology (P=0.003), and PTMA expression (P<0.001). As AJCC T-stage and BCLC stage were associated with vascular invasion, we did not make multiple analyses with these indices to avoid potentialbias. The signifcance of serum α-fetoprotein level was not evaluated because of missing data (n=218). In multivariate analyses, intrahepatic metastasis (P<0.001), viral etiology (P=0.017), and PTMA expression (P= 0.001) were independent predictors of early recurrence (Table 2).
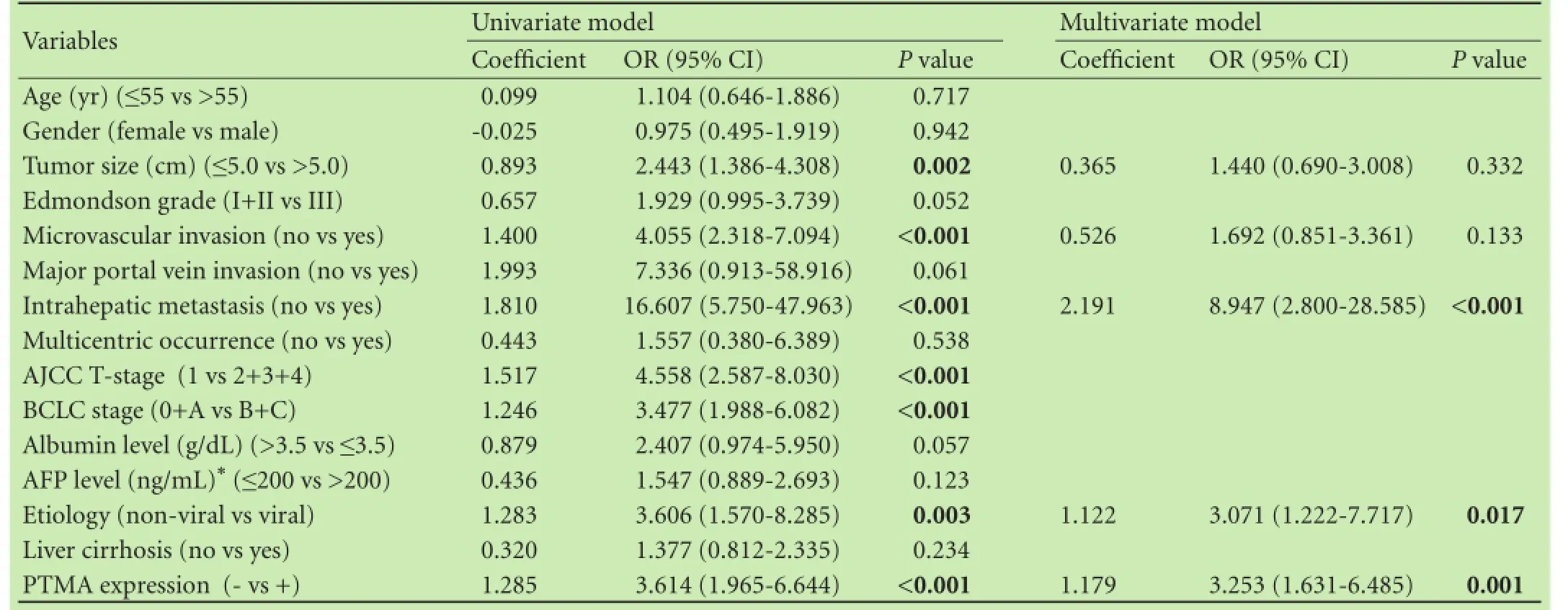
Table 2.Univariate and multivariate logistic regression models for the prediction of early recurrence in the 226 HCC patients
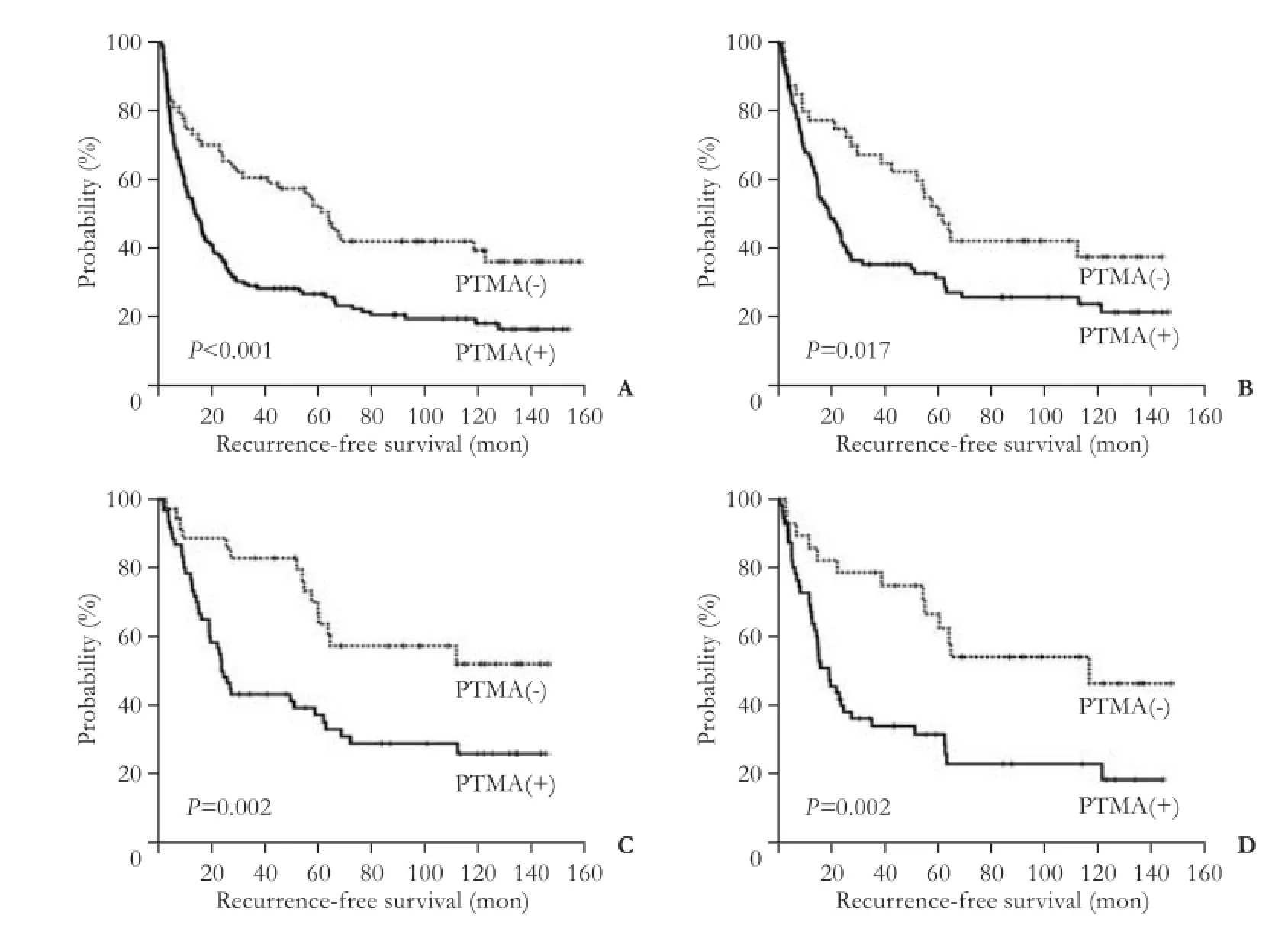
Fig. 2.Kaplan-Meier survival curves showing recurrence-free survival among all patients (A), patients with tumor size ≤5.0 cm (B), patients at AJCC T-stage 1 (C), and patients with α-fetoprotein ≤20 ng/mL (D) for PTMA expression.
Association between PTMA expression and prognosis of HCC
The RFS and OS rates in the 226 HCC patients were 38.4% and 75.1% at 3 years, 33.3% and 65.5% at 5 years, 27.2% and 57.1% at 7 years and 26.5% and 50.6% at 9 years, respectively. Univariate analyses revealed that larger tumor size, Edmondson grade III, microvascular invasion, major portal vein invasion, intrahepatic metastasis, higher AJCC T-stage, higher BCLC stage, and lower albumin level had unfavorable infuences on both RFS and OS. Higher α-fetoprotein level and viral etiology had negative infuences on RFS. PTMA expression was negatively associated with RFS (P<0.001) (Table 3). The 5-year RFS rate of the PTMA-positive group was signifcantly lower than that of the PTMA-negative group (26.4% vs 50.9%) (Fig. 2A). The mean RFS of PTMA-positive group and PTMA-negative group was 41.3 and 75.7 months, respectively. Subgroup analysis showed that among patients with tumor size ≤5.0 cm (140 patients), the difference in RFS between the PTMA-positive and PTMA-negative groups was also statistically signifcant (P=0.017, Fig. 2B). Further analysis revealed that between patients at AJCC T-stage 1 (95 patients) and those with α-fetoprotein ≤20 ng/mL (83 patients), there were signifcant differences (P=0.002 andP=0.002, respectively, Fig. 2C and D).
PTMA expression was negatively associated with OS (P=0.014) (Table 3). The 5-year OS rate of the PTMA-positive group was signifcantly lower than that of the PTMA-negative group (63.1% vs 73.3%) (Fig. 3A). The mean OS of the PTMA-positive and PTMA-negative groups was 90.9 and 111.3 months, respectively. Subgroup analysis showed that among patients with tumor size ≤ 5.0 cm (140 patients), there was signifcant difference in OS between the PTMA-positive and PTMA-negative groups (P=0.047, Fig. 3B). Further analysis revealed that among patients at AJCC T-stage 1 (95 patients) and those with α-fetoprotein ≤20 ng/mL (83 patients), there was a weak association with OS (P=0.086 andP=0.060, respectively, Fig. 3C and D).
Multivariate analyses indicated that intrahepatic metastasis and lower albumin level were independent predictors of both shorter RFS and OS. Microvascular invasion and viral etiology were independent predictors of shorter RFS. PTMA expression was an independent predictor of shorter RFS (P=0.011), but not of OS (P=0.161). PTMA-positive patients were more likely to suffer from recurrence than PTMA-negative patients (hazard ratio=1.624) (Table 4).
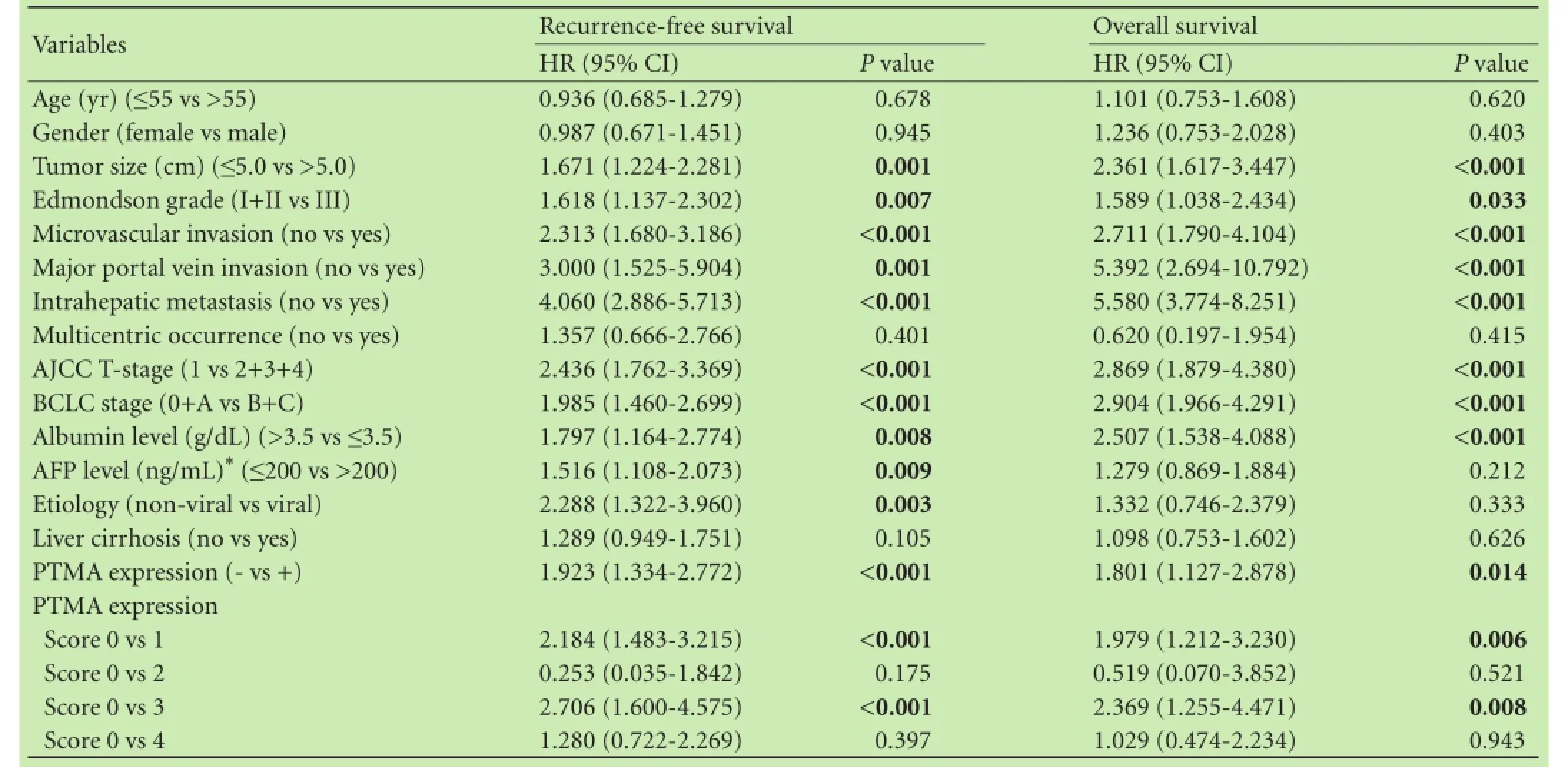
Table 3.Univariate analyses of recurrence-free survival and overall survival in the 226 HCC patients
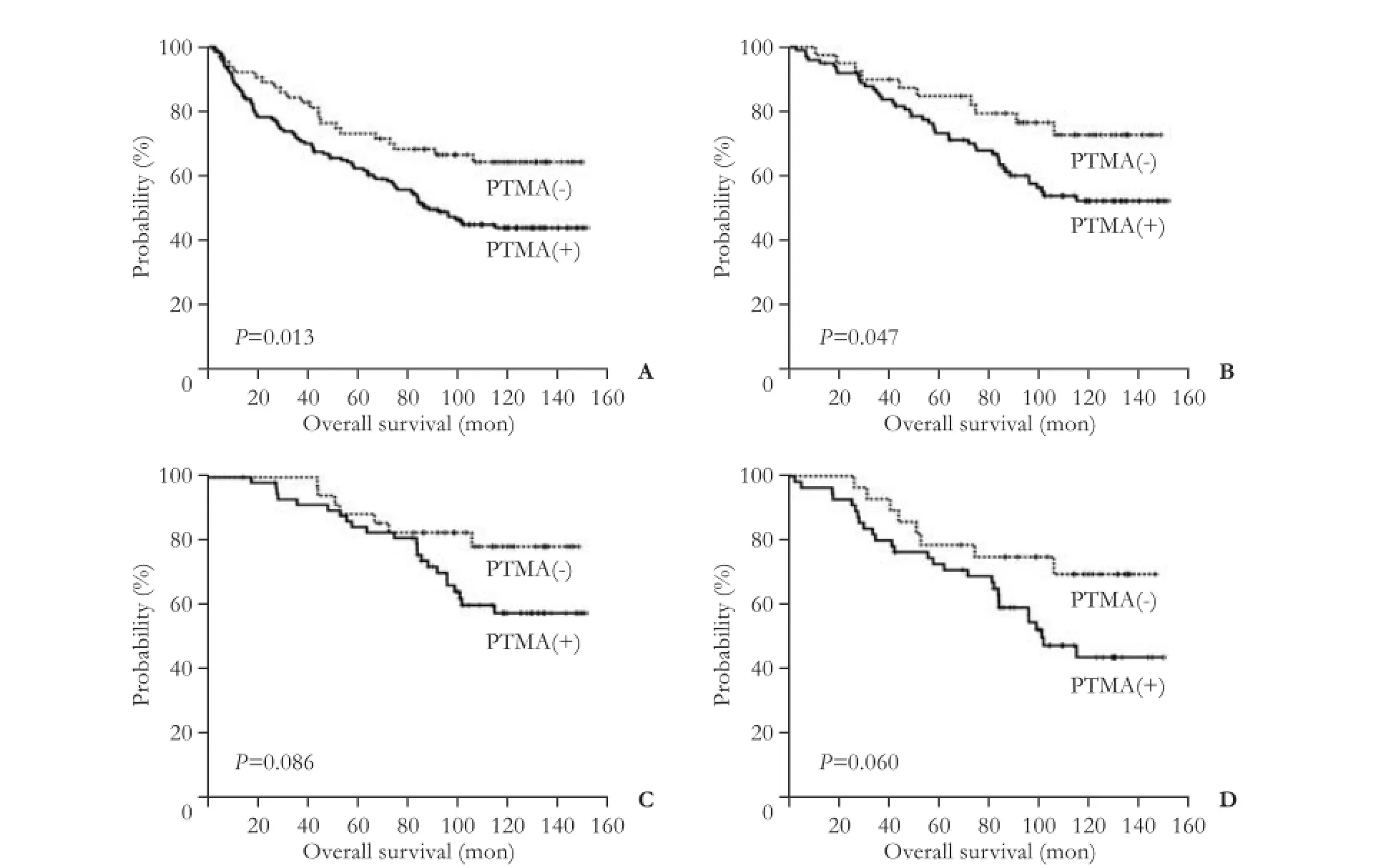
Fig. 3.Kaplan-Meier survival curves showing overall survival among all patients (A), patients with tumor size ≤5.0 cm (B), patients at AJCC T-stage 1 (C), and patients with α-fetoprotein ≤20 ng/mL (D) for PTMA expression.
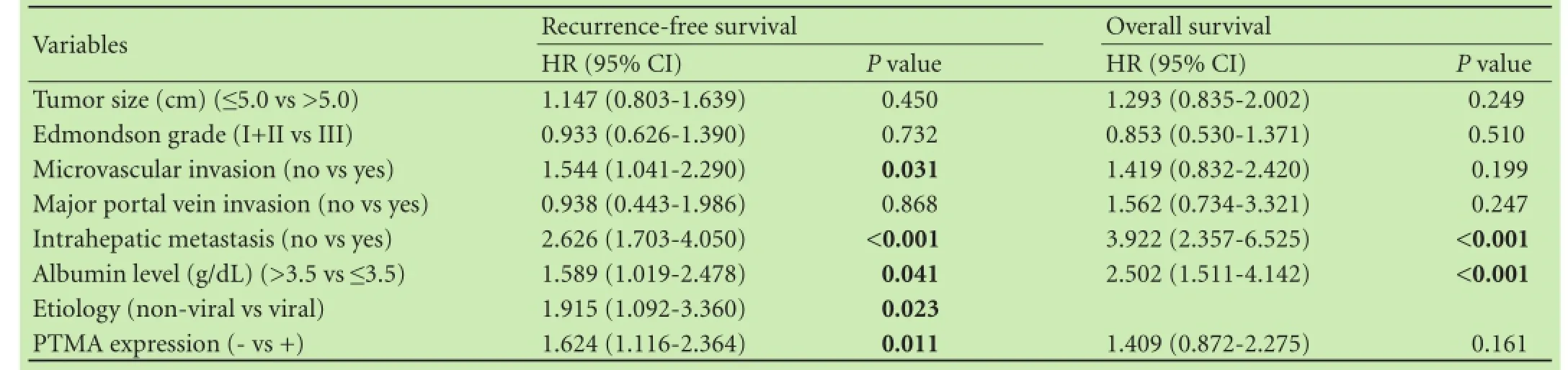
Table 4.Multivariate analyses of recurrence-free survival and overall survival in the 226 HCC patients
Discussion
PTMA overexpression was found in HCC regardless of coexisting cirrhosis or viral hepatitis, and mRNA amounts of PTMA were highly correlated with c-myc.[14]These results support the fnding that PTMA expression is under the regulation of the c-myc gene.[22]Proto-oncogenes like c-myc play an important role in the multiple process of carcinogenesis, including HCC.[23]
In the present study, we evaluated the prognostic signifcance of PTMA protein expression in a large cohort of HCC patients and demonstrated that PTMA expression was signifcantly associated with higher Edmondson grade, microvascular invasion, intrahepatic metastasis, higher AJCC T-stage, and lower albumin level. Moreover, PTMA expression was an independent predictor of early recurrence, suggesting that patients with PTMA expression need the adjuvant intervention to prevent recurrence.
HCC patients with tumor size ≤5.0 cm and patients at AJCC T-stage 1 are generally considered to be at a relatively low risk of recurrence,[24]but 97 (69.3%) of 140 with ≤5.0 cm and 57 (60.0%) of 95 AJCC T-stage 1 showed relapse. In these populations in our study, the PTMA-positive group was still signifcantly associated with poor RFS (P=0.017 andP=0.002, respectively). Serum α-fetoprotein is known to be an important predictor of recurrence of HCC after hepatectomy.[25]However, there is no effective marker for monitoring relapse in α-fetoprotein-negative (≤ 20 ng/mL) patients. Tumor re-currence was detected in 54 (65.1%) of 83 α-fetoproteinnegative patients. In α-fetoprotein-negative patients, the PTMA-positive group was signifcantly correlated with poor RFS (P=0.002). PTMA might be a useful biomarker for detecting recurrence in HCC patients with tumor size≤5.0 cm, AJCC T-stage 1, or α-fetoprotein-negative. In addition, PTMA expression was an independent predictor of shorter RFS. These fndings indicated that PTMA is a new marker for predicting the recurrence risk of HCC patients after curative hepatectomy, and could help clinicians identify patients with a high risk of recurrence. Moreover, undetectable expression of PTMA in normal liver tissues suggested that targeting PTMA for HCC therapy may not damage liver tissue. And small molecule that inhibits PTMA activity is already available.[5]
To our knowledge, this is the frst report to show that PTMA expression is a reliable predictor of early recurrence and a novel predictor of RFS in HCC patients, even those at early stage or with α-fetoprotein-negative after curative hepatectomy. Further study is needed to examine the roles of PTMA protein expression in the progression and prognosis of HCC.
Contributors:PCK proposed the study. HSY and PCK performed research and wrote the frst draft. SDH, HSH and CSY collected and analyzed the data. All authors contributed to the design and interpretation of the study and to further drafts. PCK is the guarantor.
Funding:None.
Ethical approval:This study was approved by the Institutional Review Board of Samsung Medical Center (Seoul, Korea).
Competing interest:No benefts in any form have been received or will be received from a commercial party related directly or indirectly to the subjects of this article.
1 Poon RT. Prevention of recurrence after resection of hepatocellular carcinoma: a daunting challenge. Hepatology 2011;54: 757-759.
2 Llovet JM, Schwartz M, Mazzaferro V. Resection and liver transplantation for hepatocellular carcinoma. Semin Liver Dis 2005;25:181-200.
3 Qin LX, Tang ZY. Recent progress in predictive biomarkers for metastatic recurrence of human hepatocellular carcinoma: a review of the literature. J Cancer Res Clin Oncol 2004;130:497-513.
4 Letsas KP, Frangou-Lazaridis M. Surfng on prothymosin alpha proliferation and anti-apoptotic properties. Neoplasma 2006;53:92-96.
5 Jiang X, Kim HE, Shu H, Zhao Y, Zhang H, Kofron J, et al. Distinctive roles of PHAP proteins and prothymosin-alpha in a death regulatory pathway. Science 2003;299:223-226.
6 Magdalena C, Dominguez F, Loidi L, Puente JL. Tumour prothymosin alpha content, a potential prognostic marker for primary breast cancer. Br J Cancer 2000;82:584-590.
7 Sasaki H, Nonaka M, Fujii Y, Yamakawa Y, Fukai I, Kiriyama M, et al. Expression of the prothymosin-α gene as a prognostic factor in lung cancer. Surg Today 2001;31:936-938.
8 Sasaki H, Sato Y, Kondo S, Fukai I, Kiriyama M, Yamakawa Y, et al. Expression of the prothymosin alpha mRNA correlated with that of N-myc in neuroblastoma. Cancer Lett 2001;168:191-195.
9 Leys CM, Nomura S, LaFleur BJ, Ferrone S, Kaminishi M, Montgomery E, et al. Expression and prognostic signifcance of prothymosin-alpha and ERp57 in human gastric cancer. Surgery 2007;141:41-50.
10 Tsai YS, Jou YC, Lee GF, Chen YC, Shiau AL, Tsai HT, et al. Aberrant prothymosin-alpha expression in human bladder cancer. Urology 2009;73:188-192.
11 Jou YC, Tung CL, Tsai YS, Shen CH, Syue-Yi C, Shiau AL, et al. Prognostic relevance of prothymosin-alpha expression in human upper urinary tract transitional cell carcinoma. Urology 2009;74:951-957.
12 Suzuki S, Takahashi S, Takahashi S, Takeshita K, Hikosaka A, Wakita T, et al. Expression of prothymosin alpha is correlated with development and progression in human prostate cancers. Prostate 2006;66:463-469.
13 Tzai TS, Tsai YS, Shiau AL, Wu CL, Shieh GS, Tsai HT. Urine prothymosin-alpha as novel tumor marker for detection and follow-up of bladder cancer. Urology 2006;67:294-299.
14 Wu CG, Habib NA, Mitry RR, Reitsma PH, van Deventer SJ, Chamuleau RA. Overexpression of hepatic prothymosin alpha, a novel marker for human hepatocellular carcinoma. Br J Cancer 1997;76:1199-1204.
15 Edmondson HA, Steiner PE. Primary carcinoma of the liver: a study of 100 cases among 48,900 necropsies. Cancer 1954;7:462-503.
16 Kumada T, Nakano S, Takeda I, Sugiyama K, Osada T, Kiriyama S, et al. Patterns of recurrence after initial treatment in patients with small hepatocellular carcinoma. Hepatology 1997;25:87-92.
17 Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. American Joint Committee on Cancer (AJCC) cancer staging manual, 7th ed. Chicago, IL: Springer;2010.
18 Llovet JM, Brú C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classifcation. Semin Liver Dis 1999;19:329-338.
19 Shimada M, Hamatsu T, Yamashita Y, Rikimaru T, Taguchi K, Utsunomiya T, et al. Characteristics of multicentric hepatocellular carcinomas: comparison with intrahepatic metastasis. World J Surg 2001;25:991-995.
20 Imamura H, Matsuyama Y, Tanaka E, Ohkubo T, Hasegawa K, Miyagawa S, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol 2003;38:200-207.
21 Ahn S, Hyeon J, Park CK. Notch1 and Notch4 are markers for poor prognosis of hepatocellular carcinoma. Hepatobiliary Pancreat Dis Int 2013;12:286-294.
22 Gaubatz S, Meichle A, Eilers M. An E-box element localized in the frst intron mediates regulation of the prothymosin alpha gene by c-myc. Mol Cell Biol 1994;14:3853-3862.
23 Gan FY, Gesell MS, Alousi M, Luk GD. Analysis of ODC and c-myc gene expression in hepatocellular carcinoma by in situ hybridization and immunohistochemistry. J Histochem Cytochem 1993;41:1185-1196.
24 Poon RT, Fan ST, Ng IO, Lo CM, Liu CL, Wong J. Different risk factors and prognosis for early and late intrahepatic recurrence after resection of hepatocellular carcinoma. Cancer 2000;89:500-507.
25 Kim DY, Paik YH, Ahn SH, Youn YJ, Choi JW, Kim JK, et al. PIVKA-II is a useful tumor marker for recurrent hepatocellular carcinoma after surgical resection. Oncology 2007;72:52-57.
Received January 24, 2014
Accepted after revision March 31, 2014
AuthorAffliations:Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea (Ha SY, Song DH, Hwang SH, Cho SY and Park CK)
Cheol-Keun Park, MD, PhD, Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 135-710, Korea (Tel: +82-2-34102766; Fax: +82-2-34100025; Email: ckpark@skku.edu)
© 2015, Hepatobiliary Pancreat Dis Int. All rights reserved.
10.1016/S1499-3872(14)60326-X
Published online December 8, 2015.
杂志排行

Hepatobiliary & Pancreatic Diseases International的其它文章
- Meetings and Courses
- Current strategies for preventing the recurrence of hepatocellular carcinoma after livertransplantation
- Glypican-3 as a specifc biomarker for hepatocellular carcinoma
- Inhibition of pancreatic stellate cell activity by adipose-derived stem cells
- Mutations in thep16gene in DMBA-induced pancreatic intraepithelial neoplasia and pancreatic cancer in rats
- Contrast-enhanced ultrasound in diagnosis of gallbladder adenoma