白内障患者眼生物学参数分布特征及变化趋势
2014-07-25张婧鲁建华张文芳周然王万鹏吴彩云
张婧 鲁建华 张文芳 周然 王万鹏 吴彩云
【应用研究】
白内障患者眼生物学参数分布特征及变化趋势
张婧 鲁建华 张文芳 周然 王万鹏 吴彩云
Accepted date:Jun 12,2014
From theDepartmentofOphthalmology,theSecondHospitalofLanzhouUniversity,Lanzhou730000,GansuProvince,China
Responsible author:LU Jian-Hua,E-mail:lujianhua266@sina.com
眼轴;前房深度;分布特征;变化趋势
目的 探讨中老年白内障患者眼生物学参数分布状况及变化规律。方法 选取2012年7月至2013年7月于我院住院手术治疗的40岁以上白内障患者1861例,应用IOL Master测量仪测量眼轴(axial length,AL)、前房深度(anterior chamber depth,ACD),对结果进行统计分析。结果 1861例白内障患者AL均值为23.19 mm(95%可信区间为23.15~23.23 mm),ACD均值为3.14 mm(95%可信区间为3.12~3.16 mm),男性AL、ACD均大于女性,差异均有统计学意义(均为P<0.05);AL、ACD随着年龄的增长而减小或变浅(均为P<0.001)。结论 AL、ACD随着年龄的增长而递减,应用IOL-Master测量仪测量白内障患者的眼生物学参数结果可以反映正常人群的眼解剖参数参考范围及变化趋势。
[眼科新进展,2014,34(12):1164-1167]
目前白内障手术是发达及发展中国家治疗白内障的主要方式。随着显微手术在眼科的应用和显微手术器械的发展、人工晶状体材料和制作工艺的不断进展,眼科医师和患者对白内障术后结果的预期值也在不断增加。精确的眼生物学测量是满足这一需求的关键所在[1]。目前眼科医师常应用光学相干生物测量仪(IOL-Master)来计算白内障术前人工晶状体的度数[2-4],IOL-Masrer较传统接触式A超的测量值更加精确,且具有可重复性、非接触性、操作简单、安全且患者易于接受等特点。然而目前关于眼生物学指标的研究并不多[5-7],且受不同区域、民族、性别、年龄及测量方法等因素的影响,眼生物学指标的参考范围亦不同,因此开展本地区白内障眼生物学指标的分析是十分必要的。
1 资料与方法
1.1 一般资料 选取2012年7月至2013年7月在兰州大学第二医院眼科住院手术治疗的40岁以上白内障患者共1861例,年龄(63.51±10.65)岁,其中男891例,年龄(63.87±11.02)岁,女970例,年龄(63.17±10.30)岁。
1.2 排除标准 影响眼生物学指标测量的疾病:严重角膜疾病如角膜白斑、血管翳、角膜溃疡等;眼超声检查出的严重玻璃体、视网膜疾病,如玻璃体积血、视网膜脱离等;受检眼曾行角膜移植术、角膜屈光手术、玻璃体切割术、巩膜外环扎或垫压术等;1周内曾配戴软性角膜接触镜或3周内曾配戴硬性角膜接触镜。
1.3 检查方法 记录患者眼别、年龄,测量眼压。应用IOL-Master测量仪测量患者眼轴(axial length,AL)、前房深度(anterior chamber depth,ACD),检查方法:受检者下颌置于仪器的下颌托上,令受检者注视仪器中的视标,当仪器的探头离受检者大约5.5 cm时进行对焦,然后依次对AL、ACD进行测量,测量5次,取其平均值。
1.4 统计学方法 采用SPSS 17.0 for windows软件,不同性别间年龄比较采用t检验,眼生物学参数比较采有K-S检验,P<0.05为非正态分布,进行多因素方差分析发现方差不齐,因此两样本间均数比较采用Mann-WhitneyU检验,多独立样本间均数比较采用Kruskal-Mallis检验,AL、ACD与年龄关系采用线性回归分析,以α=0.05作为检验水准。
2 结果
2.1 白内障患者眼生物学指标特征 1861例白内障患者AL值分布见图1,均值为23.19 mm(95%可信区间为23.15~23.23 mm),男性为23.25 mm(95%可信区间为23.19~23.30 mm),女性为23.14 mm(95%可信区间为23.08~23.19 mm),二者差异有显著统计学意义(Z=-3.214,P=0.001),可认为男性AL大于女性。1861例白内障患者ACD值分布见图2,均值为3.14 mm(95%可信区间为3.12~3.16 mm),男性为3.20 mm(95%可信区间为3.18~3.23 mm),女性为3.09 mm(95%可信区间为 3.06~3.12 mm),二者差异有显著统计学意义(Z=-5.838,P<0.001),可认为男性ACD大于女性。
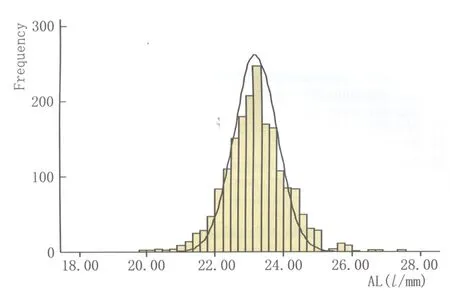
Figure 1 Distribution image of AL AL长度分布图
不同年龄组间AL与ACD比较分析结果见表1。从表1可知,不同年龄组的AL与ACD差异均有显著统计学意义(χ2=41.171、149.350,均为P<0.001),随着年龄的增长,AL长度逐渐变短,ACD逐渐变浅(图3)。
2.2 线性回归分析 AL随着年龄的增长而变小(P<0.001),每10 a以0.091 mm的速度递减,其中女性以0.135 mm的速度递减(P<0.001),而男性以0.046 mm的速度递减(P=0.095)。ACD随着年龄的增长而变浅(P<0.001),每10 a以0.100 mm的速度递减,其中女性以0.110 mm的速度递减(P<0.001),男性以0.095 mm的速度递减(P<0.001)。因变量AL、ACD与自变量年龄的回归方程分别为y=23.454-0.091x、y=3.435-0.100x,其中女性AL、ACD与年龄的回归方程为y=23.526-0.135x、y=3.403-0.110x,男性AL、ACD与年龄的回归方程为y=23.383-0.046x、y=3.483-0.095x。
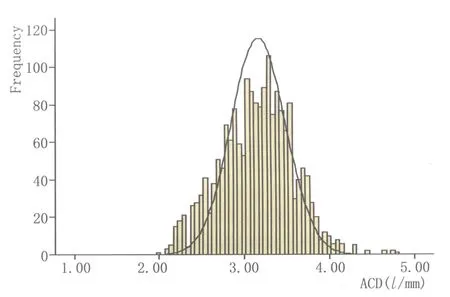
Figure 2 Distribution image of ACD ACD分布图

Figure 3 Linear graph of change tendency of AL and ACD AL、ACD与年龄变化趋势线形图

表1 不同年龄眼生物学指标均数及95%可信区间Table 1 Mean ocular biological parameters and 95% confidence intervals of different age
3 讨论
描述AL的正常参考范围,在选择合适的人工晶状体屈光度中有着重要的参考作用。本研究应用IOL-Master测得40岁以上中老年白内障患者的AL均值为23.19 mm,95%可信区间为23.15~23.23 mm;He等[8]应用A超测得广州市荔湾区1196人(50~93岁)的AL为23.11 mm(95%CI,22.48~23.74 mm),Wong等[5]应用A超测得新加坡1232人(40~81岁)AL为(23.33±1.17)mm,Fotedar等[9]应用IOL-Master测得澳大利亚1321人(>50岁)AL为23.44 mm(95%CI,23.68~23.84 mm),Shufelt等[10]应用A超测得美国5588人(>40岁)AL为(23.38±1.01)mm,Warrier等[11]应用A超测得缅甸1498人(>40岁)AL为(22.76±1.05)mm。本次研究测得AL较新加坡、澳大利亚、美国人眼轴短,较缅甸人长。这种差异可能是由种族及基因的不同引起的[11]。Foteder等[9]、Warrier等[11]、Hashemi等[12]研究均认为男性AL大于女性,本研究亦证实了这一观点。
本次研究发现40岁以后AL随着年龄的增长而减小(P<0.001),与Fotedar等[9]、Warrier等[11]、Foster等[13]及Jivrajka等[14]报道一致。进一步分析发现,40岁以后女性每10 a以0.135 mm的速度递减(P<0.001),而男性以0.046 mm的速度递减(P=0.095)。从婴儿期至青少年期AL逐渐变长容易理解[15],但中年以后AL逐渐变短却很难解释。这一趋势可以用同辈效应解释(即与青年人相比,老年人远视患病率高,近视患病率低),但Gudmundsdottir等[16]研究发现,AL随着年龄逐渐递减,这一观点削弱了这一假说。我们认为中老年人AL随着年龄的增长而递减可能与眼球随着年龄的增大逐渐萎缩有关。
相关研究发现,ACD与年龄呈负相关性[17-19],同时与种族有相关性[11],不同研究显示着不同地区的ACD分布情况[20-23]。本次研究测得40岁以后中老年人的ACD均值为3.14 mm(95%可信区间为3.12~3.16 mm),Shufelt等[10]应用A超测得美国5588人(>40岁)ACD为(3.41±0.35)mm,Warrier等[11]应用A超测得缅甸1498人(>40岁)ACD为(2.82±0.78)mm,本次研究所得ACD较美国人浅,较缅甸人深,主要原因可能是种族不同,ACD不同。本次研究发现,男性ACD较女性深(P<0.05),与其他研究报道[8,12-13]较一致。
本研究发现,40岁以后ACD随着年龄增加而变浅(P<0.001),与He等[8]、Foster等[13]报道一致。男性ACD递减的速度与女性接近。ACD随着年龄变浅与晶状体厚度随着年龄等增长变厚密切相关[24-25]。同时可能与晶状体调节能力下降、睫状肌变弱、晶状体前移有关。提示随着年龄的增长,白内障患者发生闭角型青光眼的危险性增加。
准确的眼生物参数测量对于眼屈光手术人工晶状体屈光度的计算、屈光不正等眼病诊断和治疗具有很重要的临床意义。虽然眼生物学测量在临床上应用广泛,但是国内相关研究并不多,尤其应用IOL-Master测量眼生物学指标的研究更少。白内障患者不会对眼球生物学测量的准确性产生明显的影响,因此本次研究应用IOL-Master测量仪对白内障患者的眼生物学指标进行分析,所得结果可以反映正常人群的眼解剖参数参考范围及变化趋势,并为眼科手术提供解剖学参考和眼病诊断依据。
1 Verhulst E,Vrijghem JC.Accuracy of intraocular lens power calculations using the Zeiss IOL master.A prospective study[J].BullSocBelgeOphtalmol,2001,281(1):61-65.
2 Haigis W,Lege B,Miller N,Schneider B.Comparison of immersion ultrasound biometry and partial coherence interferometry for intraocular lens calculation according to Haigis[J].GraefesArchClinExpOphthalmol,2000,238(9):765-773.
3 Kiss B,Findl O,Menapace R,Wirtitsch M,Drexler W,Hitzenberger CK,etal.Biometry of cataractous eyes using partial coherence interferometry:clinical feasibility study of a commercial prototype[J].JCataractRefractSurg,2002,28(2):224-229.
4 Packer M,Fine IH,Hoffman RS,Coffman PG,Brown LK.Immersion A-scan compared with partial coherence interferometry:outcomes analysis[J].JCataractRefractSurg,2002,28(2):239-242.
5 Wong TY,Foster PJ,Ng TP,Tielsch JM,Johnson G,Seah SKL.Variations in ocular biometry in an adult Chinese population in Singapore:the Tanjong Pagar Survey[J].InvestOphthalmolVisSci,2001,42(1):73-80.
6 Francois J,Goes F.Ultrasonographic study of 100 emmetropic eyes[J].Ophthalmologica,1977,175(6):321-327.
7 Villarreal MG,Ohlsson J,Abrahamsson M,Sjostrom A,Sjostrand J.Myopisation:the refractive tendency in teenagers.Prevalence of myopia among young teenagers in Sweden[J].ActaOphthalmolScand,2000,78(2):177-181.
8 He M,Huang W,Li Y,Zheng YF,Yin QX,Foster PJ.Refractive error and biometry in older Chinese adults:the Liwan eye study[J].InvestOphthalmolVisSci,2009,50(11):5130-5136.
9 Fotedar R,Wang JJ,Burlutsky G,Morgan IG,Rose K,Wong TY,etal.Distribution of axial length and ocular biometry measured using partial coherence laser interferometry(IOL Master)in an older white population[J].Ophthalmology,2010,117(3):417-423.
10 Shufelt C,Fraser-Bell S,Ying-Lai M,Torres M,Varma R.Refractive error,ocular biometry,and lens opalescence in an adult population:the Los Angeles Latino Eye Study[J].InvestOphthalmolVisSci,2005,46(12):4450-4460.
11 Warrier S,Wu HM,Newland HS,Muecke J,Selva D,Aung T,etal.Ocular biometry and determinants of refractive error in rural Myanmar.the Meiktila Eye Study[J].BritJOphthalmol,2008,92(12):1591-1594.
12 Hashemi H,Khabazkhoob M,Miraftab M,Emamian MH,Shariati M,Abdolahinia T,etal.The distribution of axial length,anterior chamber depth,lens thickness,and vitreous chamber depth in an adult population of Shahroud,Iran[J].BMCOphthalmol,2012,12(1):50.
13 Foster PJ,Alsbirk PH,Baasanhu J,Munkhbayar D,Uranchimeg D,Johnson GJ.Anterior chamber depth in Mongolians:variation with age,sex,and method of measurement[J].AmJOphthalmol,1997,124(1):53-60.
14 Jivrajka R,Shammas MC,Boenzi T,Swearingen M,Shammas HJ.Variability of axial length,anterior chamber depth,and lens thickness in the cataractous eye[J].JCataractRefractSurg,2008,34(2):289-294.
15 Mutti DO,Mitchell GL,Jones LA,Friedman NE,Frane SL,Lin WK,etal.Axial growth and changes in lenticular and corneal power during emmetropization in infants[J].InvestOphthalmolVisSci,2005,46(9):3074-3080.
16 Gudmundsdottir E,Arnarsson A,Jonasson F.Five-year refractive changes in an adult population:Reykjavik Eye Study[J].Ophthalmology,2005,112(4):672-677.
17 Casson RJ.Anterior chamber depth and primary angle-closure glaucoma:an evolutionary perspective[J].ClinExpOphthalmol,2008,36(1):70-77.
18 Edmonds CR,Wung SF,Pemberton B,Surrett BBS.Comparison of anterior chamber depth of normal and keratoconus eyes using Scheimpflug photography[J].EyeContactLens,2009,35(3):120-122.
19 Rabsilber TM,Khoramnia R,Auffarth GU.Anterior chamber measurements using Pentacam rotating Scheimpflug camera[J].JCataractRefrSurg,2006,32(3):456-459.
20 Buehl W,Stojanac D,Sacu S,Drexler W,Findl O.Comparison of three methods of measuring corneal thickness and anterior chamber depth[J].AmJOphthalmol,2006,141(1):7-12.
21 Elbaz U,Barkana Y,Gerber Y,Avni I,Zadok D.Comparison of different techniques of anterior chamber depth and keratometric measurements[J].AmJOphthalmol,2007,143(1):48-53.
22 Huang J,Pesudovs K,Wen D,Chen S,Wrigh T,Wang X,etal.Comparison of anterior segment measurements with rotating Scheimpflug photography and partial coherence reflectometry[J].JCataractRefrSurg,2011,37(2):341-348.
23 Xu L,Cao WF,Wang YX,Chen CX,Jonas JB.Anterior chamber depth and chamber angle and their associations with ocular and general parameters:the Beijing Eye Study[J].AmJOphthalmol,2008,145(5):929-936.
24 Praveen MR,Vasavada AR,Shah SK,Shah CB,Patel UP,Dixit NV,etal.Lens thickness of Indian eyes:impact of isolated lens opacity,age,axial length,and influence on anterior chamber depth[J].Eye(Lond),2009,23(7):1542-1548.
25 Brown NP,Koretz JF,Bron AJ.The development and maintenance of emmetropia[J].Eye,1999,13(1):83-92.
date:Feb 28,2014
Distribution and change tendency of ocular biological parameters in cataract patients
ZHANG Jing,LU Jian-Hua,ZHANG Wen-Fang,ZHOU Ran,WANG Wan-Peng,WU Cai-Yun
axial length;anterior chamber depth;distribution characteristics;change tendency
Objective To discuss the distribution and variation of ocular biological parameters in cataract patients.Methods This study includes 1681 cataract patients in our hospital from July 2012 to July 2013.The age of patients were above 40 years old.Axial length (AL),anterior chamber depth (ACD)were measured by partial coherence laser interferometry (IOL Master),and the results were statistical analyzed.Results The mean AL of 1861 patients was 23.19 mm(95% CI,23.15-23.23 mm),mean ACD was 3.14 mm(95%CI,3.12-3.16 mm).AL and ACD in male were more than those in female,there were statistical differences (allP<0.05).AL and ACD significantly decreased with age increase (allP<0.001).Conclusion AL and ACD significantly decrease with age increase.The analysis of the ocular biological parameters in cataract patients by IOL Master can indicate the normal value of the ocular anatomic parameters and variation tendency.
张婧,鲁建华,张文芳,周然,王万鹏,吴彩云.白内障患者眼生物学参数分布特征及变化趋势[J]. 眼科新进展,2014,34(12):1164-1167.
10.13389/j.cnki.rao.2014.0323
张婧,女,1989年5月出生,在读硕士研究生。联系电话:15984412890;E-mail:jingzhang2011@lzu.edu.cn
About ZHANG Jing:Female,born in May,1989.Postgraduate student.Tel:15984412890;E-mail:jingzhang2011@lzu.edu.cn
2014-02-28
修回日期:2014-06-12
本文编辑:周志新
730000 甘肃省兰州市,兰州大学第二医院眼科
鲁建华,E-mail:lujianhua266@sina.com
[Rec Adv Ophthalmol,2014,34(12):1164-1167]