阿司匹林相关小麦依赖运动诱发过敏性休克:20例回顾性分析
2014-04-09姜楠楠文利平
姜楠楠,尹 佳,文利平
(中国医学科学院 北京协和医学院 北京协和医院变态反应科,北京 100730)
ChinJAllergyClinImmunol,2014,8(3):181- 187
食物依赖运动诱发过敏性休克(food-dependent exercise induced anaphylaxis,FDEIA)是指患者进食致敏食物后4~6 h内在运动过程中发生的严重过敏反应,其典型的临床表现是皮肤瘙痒、风团样皮疹,呼吸困难,腹痛、恶心、呕吐,严重时可发生休克甚至死亡[1]。Morita等[1]研究示,小麦是日本FDEIA的主要致敏食物,该类型称为小麦依赖运动诱发过敏性休克(wheat-dependent exercise induced anaphylaxis,WDEIA)。Kushimoto和Aoki[2]于1985年首次报道WDEIA;2009年,尹佳和文利平[3]对我国15例WDEIA患者临床资料进行了总结。Palosuo等[4]的研究指出,ω-5醇溶蛋白是小麦主要致敏蛋白。近年来研究显示,FDEIA或食物过敏患者摄入阿司匹林后再进食致敏食物也可诱发或加重休克症状[5-7]。1984年,Cant 等[7]首次提出了阿司匹林可加重食物过敏症状,该文报道了1例14岁男孩因头痛服用阿司匹林600 mg后进食花生诱发过敏性休克,患者在发生此次严重过敏反应前进食花生仅诱发一过性轻微过敏反应。1990年,Dohi等[8]报道了3例FDEIA患者因感冒伴牙痛口服阿司匹林,随后进食致敏食物而诱发FDEIA症状。研究显示,阿司匹林可加重或诱发WDEIA症状,称为阿司匹林相关WDEIA(aspirin-related WDEIA)或阿司匹林诱发的WDEIA(aspirin-provoked WDEIA)[5-6, 9],其机制尚不明确,可能与阿司匹林降低肥大细胞活化阈值和加速小肠对小麦醇溶蛋白的吸收有关[10-11]。目前,检索万方数据、中国知网和维普等中文期刊数据库,尚未见我国有阿司匹林相关WDEIA的文献报道。本研究对2008年9月至2013年12月在北京协和医院变态反应科确诊的20例阿司匹林相关WDEIA病例进行临床资料总结和分析。
对象和方法
对象
2008年9月至2013年12月在北京协和医院变态反应科确诊的阿司匹林相关WDEIA患者20例。
诊断标准
WDEIA诊断标准:参考文献[3]。
阿司匹林相关WDEIA诊断标准:目前尚无明确诊断标准。本研究认为,WDEIA确诊患者若因心血管疾病长期服用阿司匹林或口服阿司匹林后进食小麦制品当天发生过敏性休克,则为阿司匹林相关WDEIA。
小麦诱因判断依据:根据小麦水溶蛋白(f4)、面筋(f79)及ω-5醇溶蛋白血清特异性IgE(specific IgE,sIgE)检测(Phadia250 Detection System,ImmunoCAP,Phadia AB,Sweden)和或皮肤点刺试验结果判断。血清sIgE>0.35 kUL为阳性,皮肤点刺试验操作方法和判定标准参考文献[12]。由于口服激发试验存在诱发过敏性休克的潜在风险,本研究纳入的所有病例均未进行小麦口服激发试验。
过敏性休克诊断标准及严重程度分级:诊断标准参考2006年美国国家过敏及感染性疾病研究院制定的标准[13]。按照文献[14]将临床表现分为3级(轻度、中度、重度)。
临床观察指标
人口统计学资料,合并疾病,过敏性休克发作次数和临床表现,阿司匹林服用情况。
统计学分析
数据统计分析应用SPSS 17.0软件,连续性变量用平均值(均数±标准差)表示,分类变量以百分比或率表示。
结 果
基线资料
20例患者中男13例,女7例;过敏性休克平均发病年龄为55(41~70)岁。70%(1420)患者休克前曾反复发作荨麻疹,荨麻疹平均病程为8.8年(2个月~20年)。
阿司匹林服用情况:所有患者均无阿司匹林及其他非甾体抗炎药(non-steroidal anti-inflammatory drugs,NSAID)过敏史。20例患者服用阿司匹林剂量为40~150 mgd,75%(1520)同时服用抗高血压药物。
小麦诱因判断:20例患者均检测了3种小麦蛋白sIgE,ω-5醇溶蛋白血清sIgE阳性率为100%(2020),小麦水溶蛋白(f4)sIgE阳性率为50%(1020),面筋(f79)sIgE阳性率为90%(1820)(表1)。
阿司匹林相关WDEIA临床表现及伴发因素
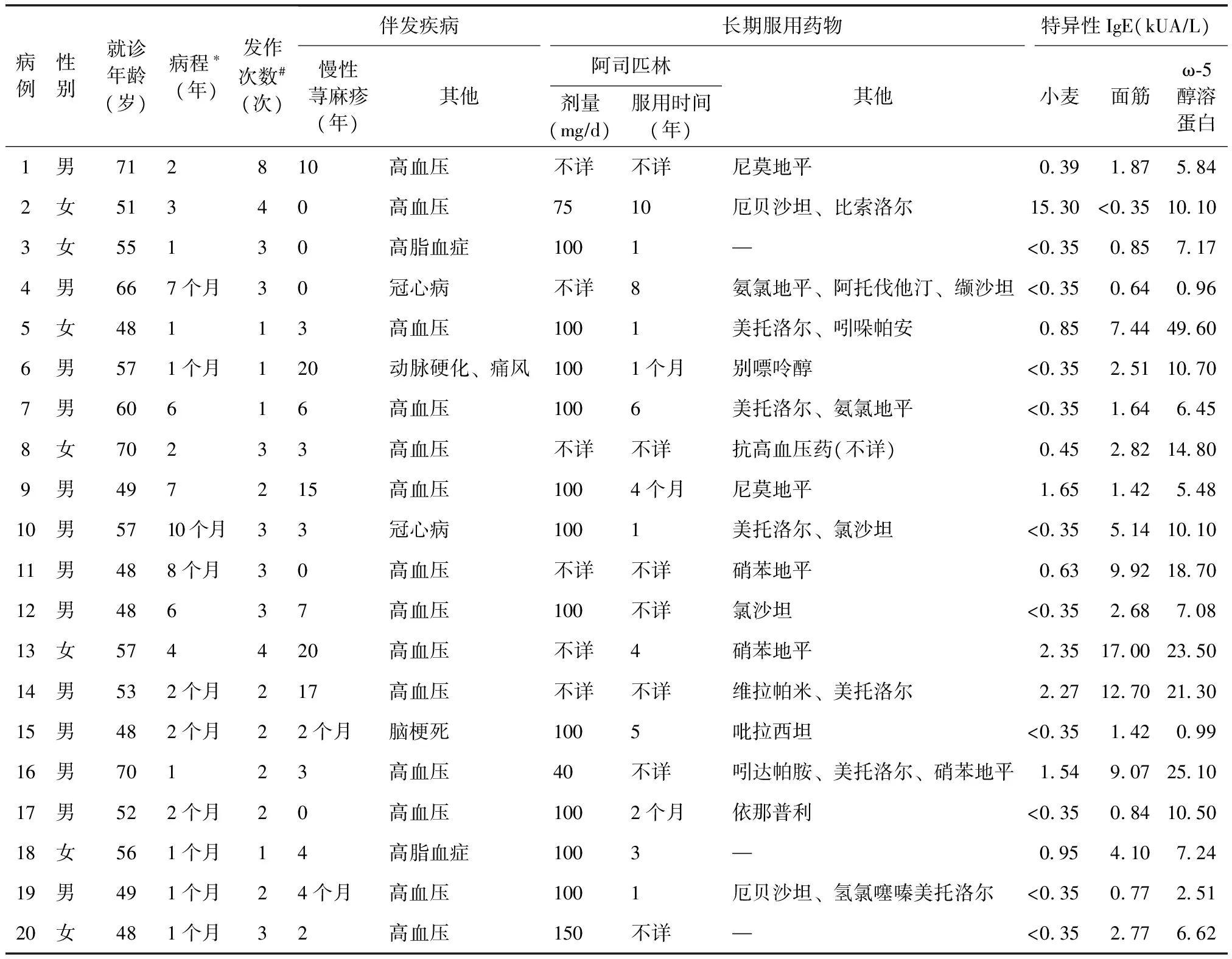
表1 20例阿司匹林相关小麦依赖运动诱发过敏性休克患者基线资料
冠心病:冠状动脉粥样硬化性心脏病;—:无其他用药;*过敏性休克初次发作距临床确诊时间;#就诊前过敏性休克发作次数
治疗
50次过敏性休克中,4次治疗不详。在46次有治疗记录的过敏休克中,15%(746)自行缓解,11%(546)自行口服抗组胺药治疗,74%(3446)急诊治疗。在34次急诊治疗中,19次有记录,其中58%(11/19)应用糖皮质激素,42%(8/19)应用肾上腺素。

表2 20例阿司匹林相关小麦依赖运动诱发过敏性休克患者临床表现
*过敏性休克发作总次数为50次
随访
随访者14例,50%(7/14)患者确诊后停用阿司匹林同时严格禁食小麦类食物后未再发生休克。29%(4/14)患者仅停用阿司匹林未严格禁食小麦制品,其中1例患者进食面食后仍反复发作全身风团样皮疹(与运动无关)但未发生休克,另外3例患者进食面食后避免剧烈运动,未再次发作荨麻疹或严重过敏反应。21%(3/14)患者严格禁食小麦制品但未停用阿司匹林,均无荨麻疹或过敏性休克发作(表3)。
讨 论
过敏性休克是一种严重且威胁生命的全身多系统速发反应,多种因素可诱发或加重其症状,这些因素被视为加重因素或伴发因素。有研究显示,约30%的过敏性休克存在加重因素[15]。除运动外,多种药物(如阿司匹林、抗高血压药物等)也是过敏性休克的加重因素。伴发因素加重休克发生的机制主要是降低效应细胞活化阈值及增加过敏原生物利用度。
本研究共纳入了20例阿司匹林相关WDEIA患者,就诊年龄均≥48岁,且男性多于女性,可能因为我国男性心血管疾病患病率略高于女性[16]。70%(1420)患者休克前曾反复发作荨麻疹,荨麻疹最长病程达20年,这可能与小麦过敏轻微发作有关。8例患者规律口服阿司匹林后原有荨麻疹症状加重或休克频率增加。国内外指南推荐小剂量阿司匹林(75~150 mg)作为心脑血管事件一级预防药物用于高血压、高脂血症、糖尿病等高危人群[17]。本研究所有对象均为小剂量口服阿司匹林(40~150 mgd)。而美国食品与药品管理局(FDA)认为,目前证据尚不支持阿司匹林可用于心脑血管事件一级预防[18]。
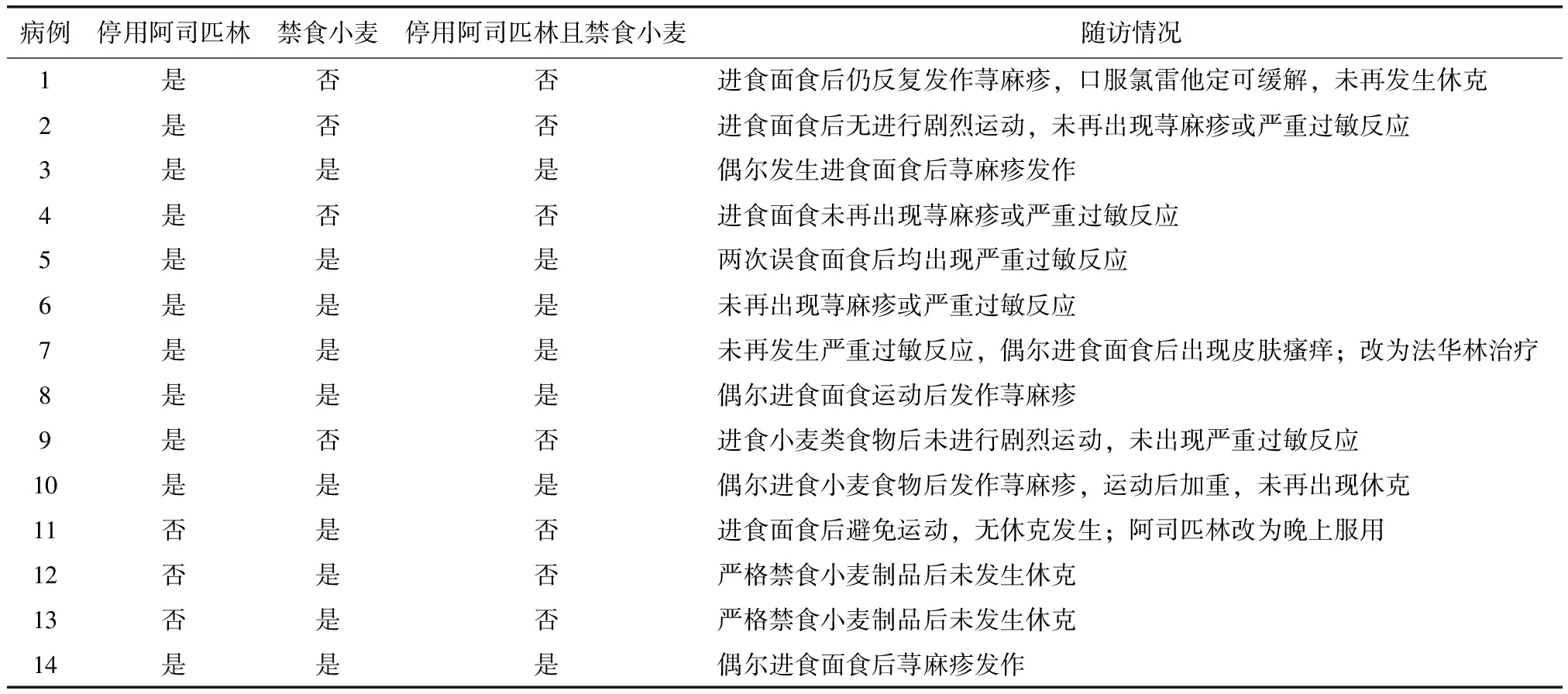
表3 14例阿司匹林相关小麦依赖运动诱发过敏性休克患者随访记录
本研究有记录的50次过敏性休克中,62%发生在运动过程中。运动是最早被人们认识也是目前研究最多的过敏性休克伴发因素。1979年,Maulitz等[19]首次提出了运动是过敏性休克的伴发因素,该文报道了1例患者进食贝类后慢跑过程中出现过敏性休克,但运动和贝类单独激发并不能导致休克,此类疾病即为FDEIA。WDEIA为FDEIA最常见的类型。目前,运动作为伴发因素在WDEIA作用机制主要集中于以下两个方面:(1)运动增加食物过敏原的生物利用度,WDEIA患者进食小麦制品后运动可显著增加血清小麦醇溶蛋白水平,原因可能与运动导致小肠屏障破坏从而使醇溶蛋白吸收增加有关[6]。也有研究显示,只有高强度和长时间(>8 h)的运动才可引起小肠屏障破坏[20]。这一假设仍需进一步深入研究。(2)可能与肠道黏膜谷氨酰胺转胺酶(tTG)活化使效应细胞脱颗粒增加有关。运动后白介素-6表达量增加50~100倍,从而诱导tTG活化,导致ω-5醇溶蛋白肽段聚合[21],使更多的IgE受体交联、活化效应细胞[22]。
本研究中85%过敏性休克累及心血管系统,Simons[33]研究示过敏性休克心血管系统累及比例约为45%。本研究结果相对较高可能与患者基础心血管疾病及服用阿司匹林和抗高血压药有关。
总之,目前研究显示,阿司匹林可诱发或加重FDEIA症状,文献报道抗高血压药尤其是ACEI类和β肾上腺素受体拮抗剂是重度过敏性休克的危险因素。因此,是否给予既往有食物过敏或过敏性休克者服用阿司匹林和抗高血压药取决于个体的利益风险比。
[1]Morita E, Kunie K, Matsuo H. Food-dependent exercise-induced anaphylaxis[J].J Dermatol Sci, 2007, 47:109-117.
[2]Kushimoto H, Aoki T. Masked type-I wheat allergy-relation to exercise-induced anaphylaxis[J].Arch Dermatol, 1985, 121:355-360.
[3]尹佳, 文利平. 小麦依赖-运动诱发的严重过敏反应:15例病例分析[J].中华临床免疫和变态反应杂志, 2010, 4:26-32.
[4]Palosuo K, Varjonen E, Kekki OM, et al. Wheat omega-5 gliadin is a major allergen in children with immediate allergy to ingested wheat[J].J Allergy Clin Immunol, 2001, 108:634-638.
[5]Harada S, Horikawa T, Ashida M, et al. Aspirin enhances the induction of type I allergic symptoms when combined with food and exercise in patients with food-dependent exercise-induced anaphylaxis[J].Br J Dermatol, 2001, 145:336-339.
[6]Matsuo H, Morimoto K, Akaki T, et al. Exercise and aspirin increase levels of circulating gliadin peptides in patients with wheat-dependent exercise-induced anaphylaxis[J].Clin Exp Allergy, 2005, 35:461- 466.
[7]Cant AJ, Gibson P, Dancy M. Food hypersensitivity made life threatening by ingestion of aspirin[J].BMJ, 1984, 288:755-756.
[8]Dohi M, Suko M, Sugiyama H, et al. 3 cases of food-dependent exercise-induced anaphylaxis in which aspirin intake exacerbated anaphylactic symptoms[J].Arerugi, 1990, 39:1598-1604.
[9]Aihara M, Miyazawa M, Osuna H, et al. Food-dependent exercise-induced anaphylaxis:influence of concurrent aspirin administration on skin testing and provocation[J].Br J Dermatol, 2002, 146:466- 472.
[10] Sanchez-Borges M, Capriles-Hulett A, Caballero-Fonseca F. Cutaneous reactions to aspirin and nonsteroidal antiinflammatory drugs[J].Clin Rev Allergy Immunol,2003, 24:125-135.
[11] Wojnar RJ, Hearn T, Starkweather S. Augmentation of allergic histamine release form human leukocytes by non-steroidal anti-inflammatory analgesic agents[J].J Allergy Clin Immunol, 1980, 66:37- 45.
[12] Adkinson NF, Bochner BS, Burks AW, et al. Middleton’s allergy:principles and practice[M].8th. Philadelphia:USA Elsevier Inc, 2014:1119-1132.
[13] Sampson HA, Munoz-Furlong A, Campbell RL, et al. Second Symposium on the Definition and Management of Anaphylaxis:Summary report-Second National Institute of Allergy and Infectious DiseaseFood Allergy and Anaphylaxis Network Symposium[J].Ann Emerg Med,2006, 47:373-380.
[14] Huang F, Chawla K, Jarvinen KM, et al. Anaphylaxis in a New York City pediatric emergency department:Triggers, treatments, and outcomes[J].J Allergy Clin Immunol, 2012, 129:162-168e3.
[15] Wolbing F, Fischer J, Koberle M, et al. About the role and underlying mechanisms of cofactors in anaphylaxis[J].Allergy, 2013, 68:1085-1092.
[16] 顾东风, He J, 吴锡桂, 等. 中国成年人高血压患病率、知晓率、治疗和控制状况[J].中华预防医学杂志, 2003, 37:84-89.
[17] 霍勇, 陆菊明. 国内外指南推荐阿司匹林用于心脑血管疾病一级预防[J].中华内科杂志, 2013, 52:882-885.
[18] FDA. Use of aspirin for primary prevention of heart attack and stroke[EBOL].(2014- 05- 02)[2014- 05-11].http:www.fda.govDRUGSRESOURCESFOR-YOUCONSUMERSUCM390574.HTM#WHYNOW
[19] Maulitz RM, Pratt DS, Schocket AL. Exercise-induced anaphylactic reaction to shellfish[J].J Allergy Clin Immunol, 1979, 63:433- 434.
[20] Robson-Ansley P, Du TG. Pathophysiology, diagnosis and management of exercise-induced anaphylaxis[J].Curr Opin Allergy Clin Immunol, 2010, 10:312-317.
[21] Ostrowski K, Rohde T, Zacho M, et al. Evidence that interleukin-6 is produced in human skeletal muscle during prolonged running[J].J Physiol,1998, 508:949-53.
[22] Palosuo K, Varjonen E, Nurkkala J, et al. Transg- lutaminase-mediated cross-linking of a peptic fraction of omega-5 gliadin enhances IgE reactivity in wheat-dependent, exercise-induced anaphylaxis[J].J Allergy Clin Immunol, 2003, 111:1386-1392.
[23] Fujii H, Kambe N, Fujisawa A, et al. Food-dependent exercise-induced anaphylaxis induced by low dose aspirin therapy[J].Allergol Int, 2008, 57:97-98.
[24] Mortaz E, Redegeld FA, Nijkamp FP, et al. Dual effects of acetylsalicylic acid on mast cell degranulation, expression of cyclooxygenase-2 and release of pro-inflammatory cytokines[J].Biochem Pharmacol,2005, 69:1049-1057.
[25] Suzuki Y, Ra C. Analysis of the mechanism for the development of allergic skin inflammation and the application for its treatment:Aspirin modulation of IgE-dependent mast cell activation:role of aspirin-induced exacerbation of immediate allergy[J].J Pharmacol Sci 2009, 110:237-244.
[26] Lee S, Hess EP, Nestler DM, et al. Antihypertensive medication use is associated with increased organ system involvement and hospitalization in emergency department patients with anaphylaxis[J].J Allergy Clin Immunol,2013, 131:1103-1108.
[27] Rueff F, Przybilla B, Bilo MB, et al. Predictors of severe systemic anaphylactic reactions in patients with Hymenoptera venom allergy:Importance of baseline serum tryptase-a study of the European Academy of Allergology and Clinical Immunology Interest Group on Insect Venom Hypersensitivity[J].J Allergy Clin Immunol, 2009, 124:1047-1054.
[28] Toogood JH. Risk of anaphylaxis in patients receiving beta-blocker drugs[J].J Allergy Clin Immunol, 1988, 81:1-5.
[29] Blais C, Marceau F, Rouleau JL, et al. The kallikrein-kininogen-kinin system:lessons from the quantification of endogenous kinins[J].Peptides, 2000, 21:1903-1940.
[30] Overlack A. ACE inhibitor-induced cough and bronchospasm-Incidence, mechanisms and management[J].Drug Saf, 1996, 15:72-78.
[31] Nussberger J, Cugno M, Amstutz C, et al. Plasma bradykinin in angioedema[J].Lancet, 1998, 351:1693-1697.
[32] Summers CW, Pumphrey RS, Woods CN, et al. Factors predicting anaphylaxis to peanuts and tree nuts in patients referred to a specialist center[J].J Allergy Clin Immunol, 2008, 121:632-638.
[33] Simons FER. Anaphylaxis[J].J Allergy Clin Immunol,2010, 125:S161-S181.
