Therapeutic Observation on Heat-sensitive Moxibustion plus Acupoint Injection for Ankylosing Spondylitis
2013-07-18LiuMinjuanWangKuiRenChangju
Liu Min-juan, Wang Kui, Ren Chang-ju
1 Acupuncture Department, Taihe Hospital Affiliated to Hubei University of Medicine, Shiyan 442000, China
2 Rehabilitation Department, People’s Hospital Affiliated to Hubei University of Medicine, Shiyan 442000, China
Therapeutic Observation on Heat-sensitive Moxibustion plus Acupoint Injection for Ankylosing Spondylitis
Liu Min-juan1, Wang Kui2, Ren Chang-ju1
1 Acupuncture Department, Taihe Hospital Affiliated to Hubei University of Medicine, Shiyan 442000, China
2 Rehabilitation Department, People’s Hospital Affiliated to Hubei University of Medicine, Shiyan 442000, China
Objective: To observe the clinical efficacy of heat-sensitive moxibustion plus acupoint injection in treating ankylosing spondylitis (AS).
Methods: Totally 116 subjects with AS were randomized into a treatment group and a control group, 58 each. The treatment group was intervened by heat-sensitive moxibustion plus acupoint injection, and the control was by oral medication. Therapeutic efficacy was evaluated after 3 treatment courses.
Results: The markedly effective rate was 38.9% and the total effective rate was 96.6% in the treatment group versus 11.9% and 67.8% in the control group. The markedly effective rate and total effective rate in the treatment group were significantly higher than those in the control group (P<0.05).
Conclusion: Heat-sensitive moxibustion combining with acupoint injection has better therapeutic efficacy than oral medication in treating AS, and it’s easy-to-operate without adverse reactions.
Moxibustion Therapy; Acupoint Injection; Spondylitis, Ankylosing; Sulfasalazine; Diclofenac; Randomized Controlled Trial
Ankylosing spondylitis (AS) is an agnogenic immune system disease majorly manifested by chronic inflammation of the axial joints. Initial symptoms often appear in the sacroiliac joint, hips, and then generally affect the spine and limb joints[1]. Joint and ligament calcification often happens at later stage, in which spine presents bamboo-like shape, or abnormality of spine or other affected joints is developed. Besides lumbago, stiffness and limited movement, fatigue is another significant symptom experienced by a majority of patients[2]. By some specialists’ investigation, AS has a incidence rate of 0.26% in our country[3]. If it’s not intervened at early stage, it will severely influence patient’s joint function and quality of life. Currently, modern medicine mainly adopts non-steroidal anti-inflammatory drugs (NSAIDs) and immunosuppressive agents to treat AS. However, long-term use of these medicines will cause more adverse reactions rather than therapeutic effect. Acupuncture-moxibustion therapy has its advantage in treating AS, and we adopted heat-sensitive moxibustion plus acupoint injection for treatment.
1 Clinical Materials
1.1 Diagnostic criteria
Early-stage AS is diagnosed in accordance with the diagnostic and stagecriteria of AS by the First National Academic Conference on Rheumatology of Traditional Chinese and Western Medicine[4]. With AS, patients present with spinal stiffness and pain, exacerbated by movements, inability to bend or stretch back, bow-shaped back under long-time standing, and loss of work ability.
AS can be diagnosed when item ③ and one of item①, ②, and ④ are met: ① Accelerated erythrocyte sedimentation rate (ESR); ② circulating immune complex (CIC) positive; ③ indistinctness of joint edge or narrowed joint space presenting in spine X-ray; ④rheumatoid factor (RF) weakly positive or positive.
1.2 Inclusion criteria
Conforming to the diagnostic criteria of AS; with no limitation of age or gender; excluded from other treatments during research period; signed the informed consent form.
1.3 Exclusion criteria
Not conforming to the diagnostic criteria of AS; with allergies or be allergic to acupuncture-moxibustion treatment or acupoint injection; with acupuncturemoxibustion contraindications, such as skin infection, ulcer, scar or tumor in the to-be-treated areas; in co-morbid with severe primary diseases of cardiocerebrovascular, liver, kidney, hematopoietic system, or psychological conditions; with AS of later stage or severe joint abnormality; with incomplete materials or be unable to follow the current treatment, which will influence the assessment of results.
1.4 General data
All 118 patients were enrolled from the Acupuncture Department, Taihe Hospital Affiliated to Hubei University of Medicine from August 2009 to May 2012. Subjects were randomized into a treatment group and a control group by their visiting sequence, 59 each. According to statistical analysis, there were no significant differences in comparing gender, age, disease duration, and disease severity between the two groups (P>0.05), indicating comparability (table 1).
Table 1. Comparison of general data between the two groups ()

Table 1. Comparison of general data between the two groups ()
Groups n Gender (case) Male Female Average age (year) Average duration (year) Accelerated ESR CIC (+) RF (+) Abnormal X-ray findings Joint space disappeared Calcification of spine Abnormal X-ray of sacroiliac articulation Treatment 59 38 21 25.6±2.3 5.8±2.6 33 22836 6 2 25 Control 59 37 22 26.7±2.4 5.7±2.4 35 20934 6 3 26
2 Treatment Methods
2.1 Treatment group
2.1.1 Heat-sensitive moxibustion
Treated area: Areas centered by Jiaji (EX-B 2) points, Governor Vessel acupoints, tender points, or subcutaneous nodes around spinal segments with restricted motility, in a radius of 3 cm.
Operation: The physician held an ignited moxa stick to apply mild moxibustion to the selected area with the stick 1.5-2 cm away from skin. When patient found mild heat penetrating deeply into the back, heat spreading in a line, or heat radiating around, which were called heat-sensitized phenomena, the initial points were considered to be the heat-sensitized points. The above operation was repeated to find all heat-sensitized points, of which, 3-5 most sensitive points were given moxibustion later. Patient should take a comfortable position with to-be-treated areas thoroughly exposed. First, revolving moxibustion was performed, followed by bird-pecking moxibustion for strengthening the moxibustion effect to activate meridian qi. Mild moxibustion was then used to warm and unblock meridians. The operator should pay attention to skin temperature, and make sure that the patient felt warm but not burnt pain. The burnt ash should be removed at any time during the whole moxibustion process to prevent from burning of skin or clothes.
Moxibustion quantity: Treatment time of heatsensitive moxibustion varies among individuals, from several minutes to an hour, disappearance of heat sensitization should be taken as the signal to end the treatment, and the treatment was given once per day.
2.1.2 Acupoint injection
Acupoints: Bilateral Jiaji (EX-B 2) (restricted to the affected spinal segments).
Operation: 5-6 points were selected each time. Patient took a comfortable position. A 5-mL syringe was used to draw 4 mL Dang Gui (Radix Angelicae) injection and 1 mL (0.5 mg) Vitamin B12injection. The needle was obliquely inserted towards spine by depth of 1-1.5 cm. Lifting-thrusting manipulations were then performed, and the medicinal fluid was injected when there appeared heavy and distending feeling without withdrawal blood, 1 mL for each point. The points were pressed for a while after needle was removed. The treatment was given once every day.
2.2 Control group
The control group was intervened by Western medication. Sulfasalazine was taken by 0.25 g per doze and 3 times a day for the first week; the doze was increased by 0.25 g for the following weeks till the fourth week, in which it would become 1 g per doze and three times a day. Diclofenac Sodium sustained release tablets were taken by 75 mg per doze and once every day. They were both administered after dinner, 10 d as a treatment course, and 3 courses in total.
3 Therapeutic Efficacies
3.1 Criteria of therapeutic efficacy[5]
Markedly effective: Symptoms or major symptoms are gone and joint function is substantially restored; ESR and CIC are back to normal levels; patient can work normally.
Effective: Major symptoms are substantially relived and joint motility is enlarged; ESR is decreased.
Invalid: Symptoms and signs remain the same after treatment.
3.2 Statistical methods
Measurement data were expressed by mean ± standard deviation (). The inner-group comparison of measurement data was managed by using t-test, and the inter-group comparison was by using Chi-square test. The SPSS 19.0 software was adopted to process all data. P<0.05 was considered to have a statistical significance.
3.3 Treatment results
The inter-group differences of markedly effective rate and total effective rate were both statistically significant (P<0.05), indicating that heat-sensitive moxibustion plus acupoint injection has better therapeutic efficacy than oral Sulfasalazine and Diclofenac Sodium (table 2).
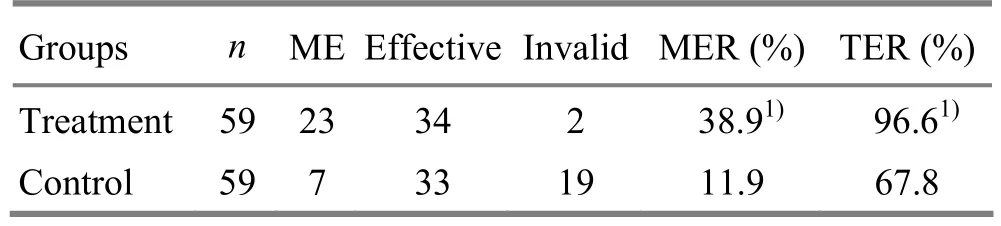
Table 2. Comparison of therapeutic efficacy between the two groups (case)
4 Discussion
AS should be classified under bone Bi-impediment or lumbago, called ‘Gui Bei feng’ or ‘Zhu Jie Feng’ in the ancient time[6]. Medical practitioners through different generations have agreed that the disease is located at lumbosacral or spinal areas, caused by congenital deficiency, liver-kidney insufficiency, impairment of the Governor Vessel, invasion of wind, cold or damp pathogens, which subsequently disturb qi of the Bladder Meridian, block meridian and collaterals, and result in qi-blood stagnation. It’s a syndrome deficient at root and excess at superficial. Young adults often run a high risk without recognizable causes, and the abnormality at later stage can cause a certain level of disability rate[7]. Modern medicine advocates an early combined intervention with regular administration of NSAIDs, Sulfasalazine, Adrenocortical Hormone, and Methotrexate, etc[8]. However, long-term use of these drugs can produce many toxic and adverse reactions.
As a traditional therapy, moxibustion has been persistently studied in the modern time. Although the mechanism of heat-sensitive moxibustion is not clear yet, its analgesic effect is existed and has been widely applied in clinic. The key point of heat-sensitive moxibustion is the selection of heat-sensitized points. The point should be initiated to boost the activation of the meridian qi. When meridian qi comes to the diseased areas, Zang-fu organs and meridians and qi-blood can be regulated, which will therefore promote the therapeutic efficacy[9]. Heat-sensitization of acupoints include heat penetration, heat transmission, heat extension, heat appearing far away from the treated area, heat in deep layer but not in superficial area, and other non-heat feelings[10]. There is a common feature in these phenomena that the involved acupoints are especially sensitive to heat produced by moxibustion. These points can generate a comparatively stronger reaction towards a mild stimulation, while other acupoints can only generate superficial or local heat by moxibustion heat. Heat-sensitized points are the best choices for moxibustion. Studies show that heat-sensitive moxibustion has been widely used to treat various types of pain symptoms and satisfactory results have been achieved[11]. This therapy can warm and unblock meridians and collaterals, toinify qi and consolidate the superficial; meanwhile, it can promote the therapeutic efficacy and improve human immune system.
Acupoint injection is a conjoint therapy combining medication, acupuncture and meridians, producing both mechanical stimulation of acupuncture and chemical stimulation of medication. Clinical and pharmaceutical trials prove that Dang Gui (Radix Angelicae) injection can effectively dilate local vessels, improve nerve nutrition, reduce the levels of inflammatory mediators and the use of analgesics[12-14]. Acupoint injection is easy-to-operate, effective without obvious adverse reactions, and thus should be applied widely in clinic.
[1] Wei YY, Huang HY, Lu HB, Li J, Ma N. Research analysis of HLA-B27 results in 456 ankylosing spondylitis patients. Jingyaotong Zazhi, 2008, 29(1): 41-46.
[2] Bi YZ. Clinical research progress of acupuncturemoxibustion in treating ankylosing spondylitis. Zhenjiu Linchuang Zazhi, 2008, 24(2): 49-52.
[3] Shi GY. Diagnostic and treatment guidance for ankylosing spondylitis (draft). Zhonghua Fengshibing Xue Zazhi, 2003, 7(17): 641.
[4] Wang FX, Wang GS, Cao SQ. Acupuncture-moxibustion plus tuina in treating 48 ankylosing spondylitis patients at early stage. Zhongguo Zhenjiu, 2003, 23(9): 518.
[5] Wang ZM, Bai RX. Diagnostic criteria of integrated traditional Chinese and Western medicine for four rheumatoid diseases. Zhongguo Zhongxiyi Jiehe Zazhi, 1989, 26(1): 13-16.
[6] Lu ZZ, Jiao SD. Practical Rheumatology of Traditional Chinese Medicine. Beijing: People’s Medical Publishing House, 1996: 608-619.
[7] Dai L, Tang MA, Yin PD. Diagnosis and treatment progress of ankylosing spondylitis. Guowai Yixue: Neike Fence, 1998, 26(1): 13-16.
[8] Yao FX, Ma SJ, Chen X. Modern Rheumatology. Beijing: People’s Military Medical Press, 1995: 305.
[9] Chen RX, Kang MF. Heat-sensitization of acupoint and its clinical significance. Zhongyi Zazhi, 2006, 47(12): 905-906.
[10] Chen RX. To guide by heat-sensitization of acupoint and to create a new era of regulating human body by moxibustion. Jiangxi Zhongyi Xueyuan Xuebao, 2007, 19(1): 57-60.
[11] Tian N. Clinical application of heat-sensitive moxibustion to pain symptoms. Linchuang Yixue Gongcheng, 2009, 16(7): 106-107.
[12] Qu BP. Scraping and cupping for 27 ankylosing spondylitis patients. Xin Zhongyi, 2001, 33(10): 49.
[13] Zhang CS, Wu RC. Clinical application of Dang Gui injection. Zhongguo Yiyuan Yaoxue Zazhi, 1995, 15(7): 301.
[14] Liu ZL, Pan QJ. Observations on the efficacy of electroacupuncture plus acupoint injection in treating acute gouty arthritis. Shanghai Zhenjiu Zazhi, 2010, 29(8): 525- 526.
Translator: Hong Jue
R246.2
A
Date: March 20, 2013
Author: Liu Min-juan, senior technician
Ren Chang-ju, supervisor nurse.
E-mail: syzyz@21cn.com
杂志排行
Journal of Acupuncture and Tuina Science的其它文章
- Clinical Observation on Treatment of Insomnia with Puncturing Back-Shu Acupoints
- Clinical Observation on Deep Acupuncture at Huantiao (GB 30) for Patients with Chronic Prostatitis
- Clinical Observation on Acupuncture for Perimenopausal Syndrome
- Therapeutic Efficacy Observation on Acupuncture for Postmenopausal Osteoporosis
- Research Progress of Acupuncture-moxibustion for Insomnia: An Analysis of Literature in Recent 5 Years
- Therapeutic Efficacy Observation on Integrative Acupuncture Therapy for Chronic Urticaria